Open Journal of Gastroenterology, 2013, 3, 314-316 OJGas
http://dx.doi.org/10.4236/ojgas.2013.37055 Published Online November 2013 (http://www.scirp.org/journal/ojgas/)
Idiopathic gastric partial necrosis*
Rocío González López#, M. Muinelo Lorenzo, J. Pérez Grobas, L. Muíños Ruano, L. Ramírez Ruíz,
A. Mohammed Salem, M. Rodríguez González, J. A. Costa Buján
Department of General Surgery and Digestive Diseases, Lucus Augusti University Hospital, Lugo, Spain
Email: #rgonlop@gmail.com
Received 21 August 2013; revised 28 September 2013; accepted 12 October 2013
Copyright © 2013 Rocío González López et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
We present the case of an elderly patient, who had
orthopaedic surgery and suffered in the early post-
operative period an idiopathic gastric partial necrosis.
We reviewed the literature and it is an extraordinar-
ily infrequent entity. Partial resections have already
been described in case of limited necrosis, as reported
in our case. Prompt diagnosis of idiopathic gastric
necrosis and aggressive treatment are mandatory.
Further awareness of this strange entity and its risk
factors can lead to a quicker diagnosis and higher
possibilities of survival for the patient.
Keywords: Gastric; Necrosis; Orthopedic Surgery
1. INTRODUCTION
Gastric partial necrosis is an extraordinarily infrequent
entity with very few cases described in literature. It has
been attributed to numerous aetiologies, such as lifestyle,
underlying morbidities, acute necrotising inflammation,
acute vascular insufficiency, post-operative complica-
tions, etc. [1].
The onset of symptoms is generally catastrophic and
surgical therapy must be urgent, as a delay in the diagno-
sis or treatment in these types of pathologies causes a
significant increase of morbimortality [1].
We describe the case of an elderly patient, who had
orthopaedic surgery and suffered in the early postopera-
tive period an idiopathic gastric partial necrosis. We re-
viewed the literature and it is the second case described
of idiopathic gastric partial necrosis attributable to or-
thopedic surgery.
2. CASE REPORT
An 82-year-old man with a history of severe chronic ob-
structive pulmonary disease and hypertension under-
goes orthopedic surgery: total right hip replacement. 48
hours after the operation, he presents with distension and
abdominal pain, so urgent blood tests are carried out
showing acute renal failure, without leuko cytosis or neu-
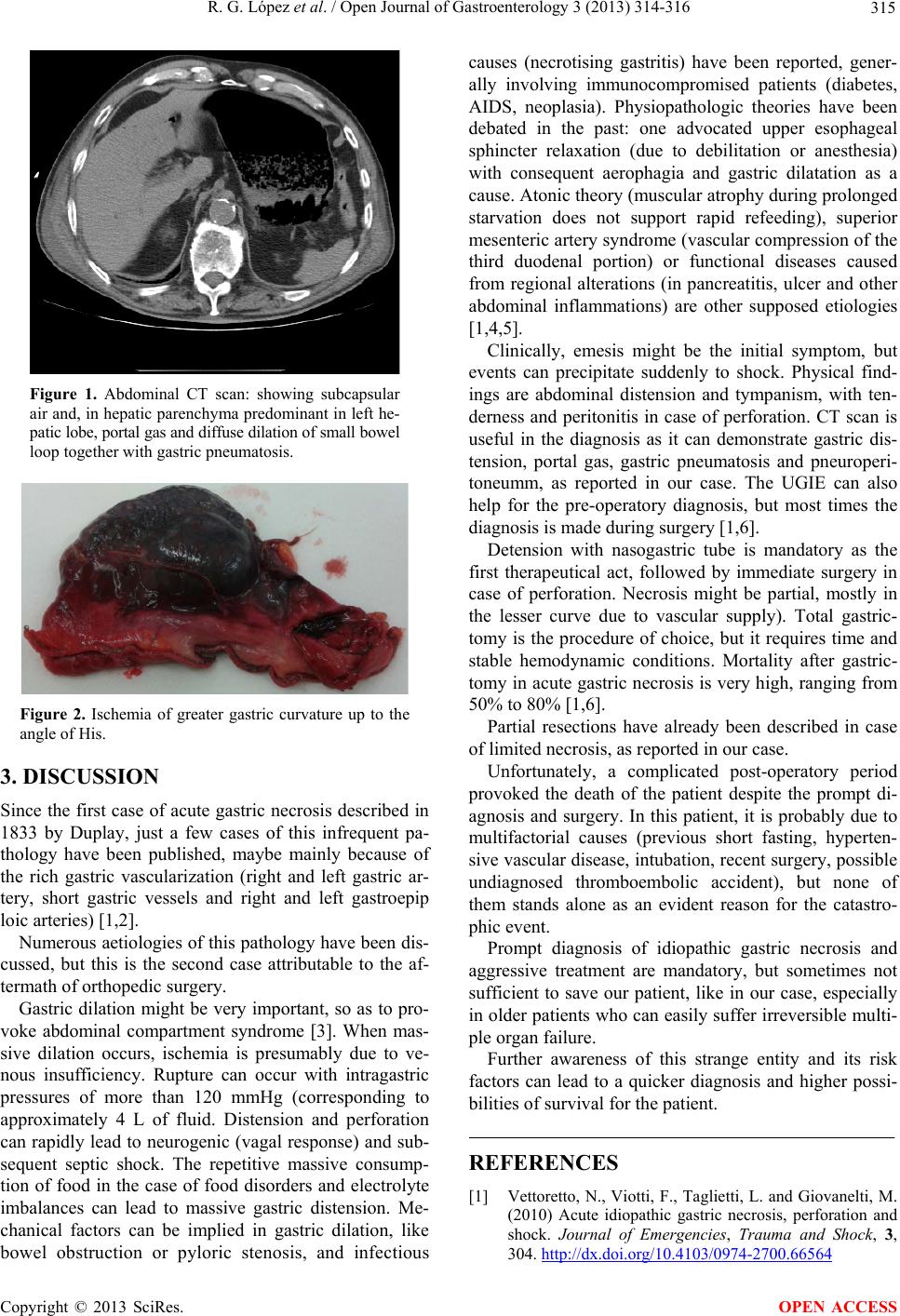
trophilia. Given the suspicion o f intra-abdomin al free gas
in the simple abdominal X-rays, an urgent computed
axial tomography (CAT) is made, showing subcapsular
air and, in hepatic parenchyma predominant in left he-
patic lobe, portal gas and diffuse dilation of small bowel
loop together with gastric pneumatosis (Figure 1). The
patient is transferred to the Service of General Surgery,
where the yield of abundant amount of content in coffee
ground through nasogastric tube is noticed (NG tube), so
urgent upper gastrointestinal endoscopy (UGIE) is re-
quested, showing severe ischemia of the gastric wall in
the greater gastric curvature and gastric body. Given the
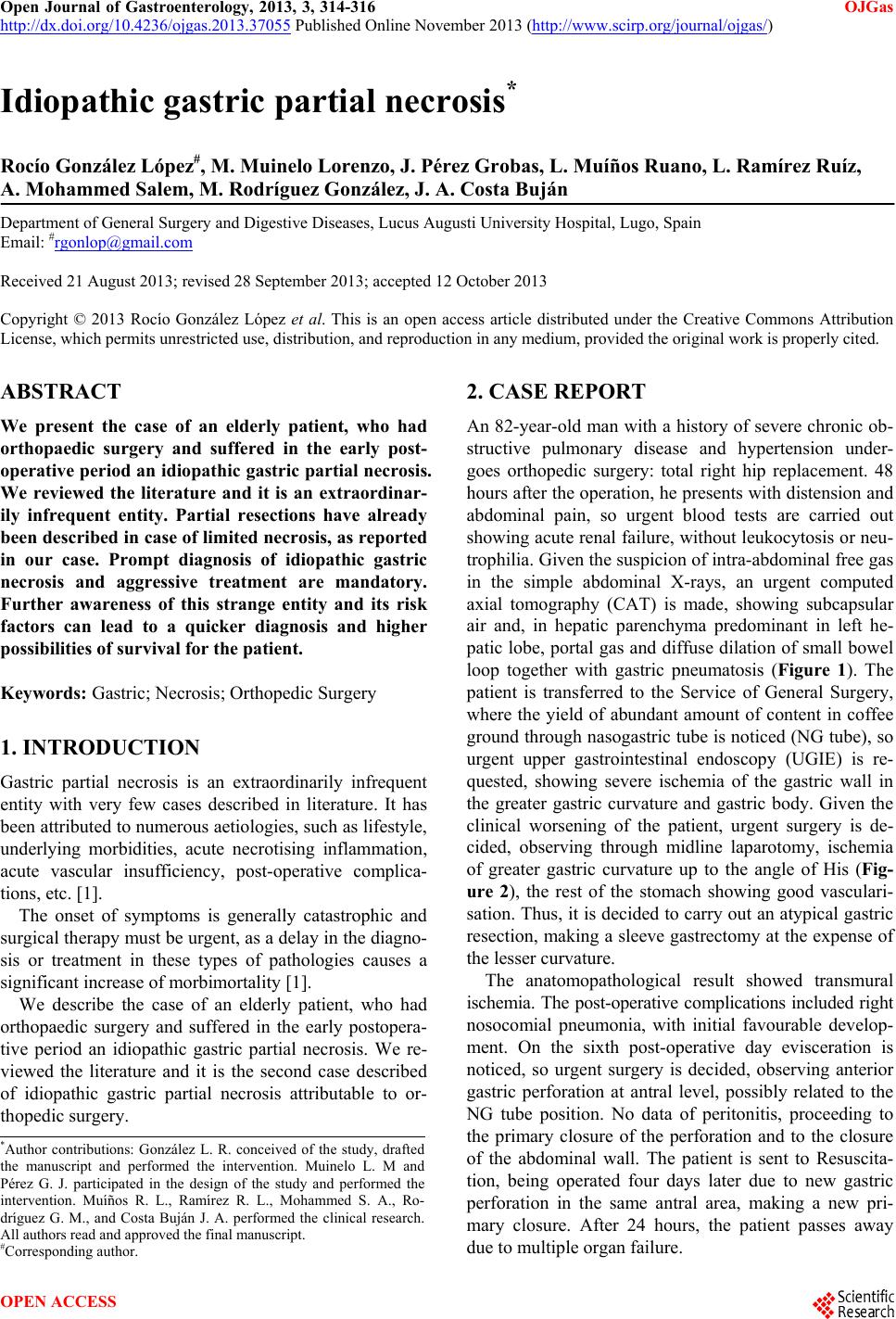
clinical worsening of the patient, urgent surgery is de-
cided, observing through midline laparotomy, ischemia
of greater gastric curvature up to the angle of His (Fig-
ure 2), the rest of the stomach showing good vasculari-
sation. Thus, it is decided to carry out an atypical gastric
resection, making a sleeve gastrectomy at the expense of
the lesser curvature.
The anatomopathological result showed transmural
ischemia. The post-operative complications included right
nosocomial pneumonia, with initial favourable develop-
ment. On the sixth post-operative day evisceration is
noticed, so urgent surgery is decided, observing anterior
gastric perforation at antral level, possibly related to the
NG tube position. No data of peritonitis, proceeding to
the primary closure of the perforation and to the closure
of the abdominal wall. The patient is sent to Resuscita-
tion, being operated four days later due to new gastric
perforation in the same antral area, making a new pri-
mary closure. After 24 hours, the patient passes away
due to multiple organ failure.
*Author contributions: González L. R. conceived of the study, drafted
the manuscript and performed the intervention. Muinelo L. M and
Pérez G. J. participated in the design of the study and performed the
intervention. Muíños R. L., Ramírez R. L., Mohammed S. A., Ro-
dríguez G. M., and Costa Buján J. A. performed the clinical research.
All authors read and approved the final manuscript.
#Corresponding autho
.
OPEN ACCESS