Health
Vol.5 No.3(2013), Article ID:28583,7 pages DOI:10.4236/health.2013.53051
Associations of social participation, demographic, socioeconomic and disease factors with nutritional risk in a group of older Hong Kong adults
![]()
Department of Health and Physical Education, The Hong Kong Institute of Education, Hong Kong, China; *Corresponding Author: chungmy@ied.edu.hk
Received 22 January 2013; revised 23 February 2013; accepted 4 March 2013
Keywords: Malnutrition; Social Participation; Mini Nutritional Assessment; Old Aged Care; Malnutrition Risk; Community Care
ABSTRACT
Aims: To identify the impact of social participation, socio-demographic, socio-economic and disease factors on nutritional risk among older persons in Hong Kong. Background: Few published work has investigated the relative risks of social participation, demographic, socioeconomic and disease factors with malnutrition in community-living older people, this study is to investigate the associations of these risk factors on the nutritional status in better nutrition support for the old age group. Design: A cross-sectional study. Methods: It was a secondary analysis of a database in a mobile community centre between January 2008 and December 2009. One thousand seven hundred and thirty one participants aged between 54 and 103 were collected. With 319 full Mini Nutritional Assessment (MNA) completed, the participants’ demographic, socioeconomic data, diseases, and nutritional status were analyzed with relative risk and 95% confidence interval level to identify the factors that make them vulnerable to nutritional risk. Results: The prevalence of malnutrition in the communitydwelling old was 3.95% and 83.7% of the sample was at risk of malnutrition. Living on allowances, young old who was socially engaged and good relationship with family members were at less risk to malnutrition. Conclusions: Special attention should be taken to these groups as they are prone to develop malnutrition.
1. INTRODUCTION
Social participation is defined as people’s social involvement and interaction with others. Participation on paid work, formal or informal volunteering, and caregiving activities are examples to it [1]. The problem in “unengaged elders” or sometimes used interchangeably with “hidden elders” is increasing. Statistics from a community survey found that around 10.8% of the assessed older people were unengaged or hidden [2]. According to the Hong Kong Commission on Poverty (CoP), these hidden older people are those who “are disengaged from the community and disadvantaged yet not helped by the available services and support” [3]. The report of the CoP states that older adults’ withdrawal from social interaction impacts on other aspects of their lives, such as their diet, because they disconnect from service providers and are thus vulnerable to malnutrition. Although studies found that higher levels of social participation is associated with lower morbidity and mortality rates [4,5], few of them document the relative risks of social unengagement other than the hospitalized and institutionalized groups. This study aims to explore the relative risks as compared with other social variables and disease factors on nutritional risk in the older population group.
2. BACKGROUND
Malnutrition occurs when an individual’s nutritional intake fails to meet their nutritional requirements [6]. It is known that malnutrition can be lethal for geriatric patients. In addition to mortality, malnutrition increases the re-admission rate of patients and the cost of hospital care in terms of length of stay [6]. Previous studies have found that malnutrition in older people is more common in groups with less education, higher depression scores, and lower cognitive and physical functioning, as these factors affect their food choices and thus their overall nutrition intake [7]. Other factors, such as modified feeding and chronic lung diseases have also been found to be significant risk factors for malnutrition [8]. Chewing and swallowing problems and reduced appetite are more often reported by those at risk of being malnourished [9].
Although the severe health consequences of malnutrition have been highlighted [6,10,11], nutritional intervention is only administered to hospitalized and institutionalized older adults in poor health [12]. With the increasing prevalence and risk of malnutrition in the older age community [13,14], malnourishment among older persons has become an urgent global health care problem. However, as a result of limited health care resources, the long term nutritional care of independent older adults living in the community, not to mention the highly vulnerable unengaged older persons disconnected from society, tends to be neglected.
The CoP study documented four observable characteristics of unengaged older adults: the inability to seek help from available services and networks; weak family, friend, and community help networks and inadequate formal service networks; the perception that seeking help is morally wrong; and earlier negative or unfavorable welfare experiences [3]. As a result of these factors, social workers and community nurses find it difficult to contact members of this group, know nothing about their needs, and are unable to connect them with the available resources and support. In this study, demographic, socioeconomic and disease factors were analyzed along with the nutritional status of community-dwelling older persons. The study’s objective was to determine the relative risks of various social participation, socio-demographic, socio-economic and disease factors on nutritional status among older persons in Hong Kong.
3. METHOD
3.1. Design and Setting
This was a secondary analysis of a database with older age visitors to a mobile community centre.
3.2. Participants
Participants of the present study were communitydwelling old adults receiving services in a mobile integrative health centre (MIHC) between January 2008 and December 2009. They were asked to give their informed consent for their health assessment results to be used in the research. Demographic information, health history, mental assessment and nutritional status were documented by advanced practice nurses. A total of 1793 participants aged between 54 and 103 were found in the database maintained by the MIHC. The study was approved by the university ethics committee.
3.3. Demographic Information
The demographic factors included gender and agewhile socio-economic factors included financial status, relationship with family members, type of residency, marital status and social participation status. All the above demographic factors except social participation status were data from face-to-face interviews conducted by the advanced practice nurses. Social participation status was identified by the social workers who referred the participants to MIHC. The social participation status was classified as unengaged if the participants were disconnected to any activities, most of the time staying at home and did not have any connection with their neighbours. The social participation status was classified as potentially unenegaged if the participants showed outside activities like walking around and going to market, but still they refused to have any connection with their neighbours and stayed at home most of the time.
3.4. Assessment of Nutritional Status
Nutritional status was assessed by the Mini Nutritional Assessment (MNA) questionnaire, which is a validated instrument designed for older persons [15] with high sensitivity and specificity in screening protein deficient malnutrition in the older community [16]. Past research has found a high correlation between Body Mass Index (BMI) and MNA scores [17,18]. In this study, nutritional status was assessed by advanced practice nurses using the Chinese version of Mini Nutritional Assessment (MNA). The MNA is an 18-item assessment, comprising anthropometric measurements, dietary questions, global health and social assessments, and a subjective assessment of health and nutrition. It is validated by Hui et al. [19] with modification in the cut-offs of body mass index as recommended by the World Health Organization (WHO) for Asian subjects [20]. The maximum score of the Chinese MNA is 30. The scoring and ranking of the Chinese MNA follows the English version. That is, an MNA score under 17 represents malnutrition, a score between 17 and 23.5 represents at risk, and a score above 23.5 represents adequate nourishment.
3.5. Statistical Analysis
The independent variables used in this study included age, gender, financial status, relationship with family members, type of residency, marital status, social participation and three health related illnesses that can affect nutritional status: cancer, respiratory illness and cardiovascular illness [21]. Descriptive analysis was performed to determine prevalence in the categories assessed by the MNA. In this study, the MNA scores were analyzed in relation to demographic, socio-economic, and disease factors to see if gender and age distribution affected the nutritional indicators. The continuous MNA scores were categorized into two groups: at risk of malnutrition or malnutrition (MNA <23.5) and well-nourished (MNA >23.5). The categorical MNA groups, together with gender, financial groups, social participation, marital status, residency and relationship with family members were analyzed by cross tabulation with measure of relative risk and 95% confidence intervals, setting MNA <23.5 as the exposure group whereas MNA >23.5 as the control group. Since age affected nutritional status of the older adults, measures of association were analyzed by confounding two age groups (young old aged <75 and older old aged ³75) as age 75 was the age one entering from young-old to aged.
4. RESULTS
4.1. Descriptive Statistics
4.1.1. Sex, Age Groups, Nutritional Status
Among the 1731 participants in the database, the mean and standard deviation of age were 74.5 and 7.6. It was found 274 participants did not have any MNA assessment and with the 1519 participants having MNA assessment, 1200 participants only received fast screening by completing the first six questions. According to the MNA assessment, if the total scores of the first six questions were lower than 11, the rest of the assessment must be continued; otherwise, the rest of the assessment could be skipped. Since we did not have the final total scores for these participants as comparisons with other participants, only those completed the 18-items MNA assessment were selected for further statistical analysis.
4.1.2. Association of Social Participation and Financial on Nutritional Status
Sixty participants in the database were found malnutrition that we estimated the prevalence of malnutrition in the community-dwelling old population was 3.95% [(60/1519) × 100%] in the accessible population and the percentage of at risk malnutrition was 83.7% [(267/319) × 100%] in our sample (Table 1). Significant difference was found in nutritional status with higher percentage of older old prone to risk of malnutrition (p = 0.016). The relative risk was 1.0 (95% C.I.: 0.95, 1.13, p = 1.126) for the total sample in gender, indicating male and female had similar risk to malnutrition. It was found that exposed risk of malnutrition was found similar by confounding age groups.
Financial status was found statistical significant in nutritional status (p = 0.001). Those financial independent had less risk (RR = 0.9, 95% C.I.: 0.81, 0.94) to malnutrition to those depending on allowances. However, the relative risk between the two became significantly lower (RR = 0.8, 95% C.I.:0.72, 0.90, p = 0.002) in the young old and the same (RR = 1.0, 95% C.I.:0.87, 1.05, p = 0.223) in the older old.
Table 1. Demographic profile of the participants.
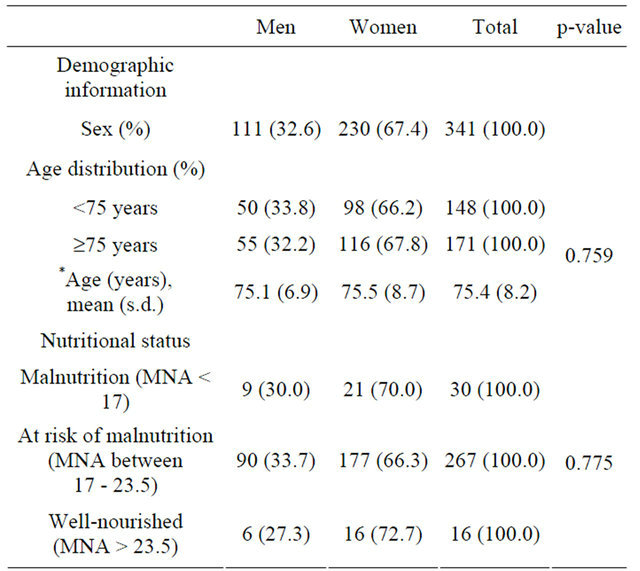
*6 male and 16 female did not report their age.
Social participation was found no observed association with nutritional status (RR = 1.0, 95% C.I.: 0.88, 1.05, p = 0.248). With confounding age groups, those engaged young old was found less exposed risk (RR = 0.9, 95% C.I.: 0.79, 1.05, p = 0.192) of malnutrition as compared with those unengaged or potentially unengaged young old. However, there was no difference between the social participation status among the older old (RR = 1.0, 95% C.I.: 0.92, 1.13, p = 0.460).
4.1.3. Association of Marital Status, Residency and Relationship with Family Members on Nutritional Status
For those living on their own (single/widowed/separated/divorced), it was found that the relative risk was 1.0 (95% C.I.: 0.92, 1.08, p = 0.506) as compared with those married. Statistical analysis with different age groups showed the same relative risk as the total sample. The results in the type of residency were the same as those in the marital status (Table 2).
For the self-reported relationship with their family members, the participants with good relationship with their family members were found at similar risk (RR = 1.0, 95% C.I.: 0.87, 1.08, p = 0.372) of malnutrition than those with fair or poor relationship with their family members. We did find lower risk of malnutrition in both age groups with confounding by age (age < 75: RR = 0.9, 95% C.I.: 0.78, 1.14, p = 0.362; age ³ 75: RR = 0.9; 95% C.I.: 0.89, 0.99).
4.1.4. Association of Diseases on Nutritional Status
For the three diseases related to nutritional status, only 2 cancer cases were found in the database. Both cases were found at risk of malnutrition. The relative risk of cancer to malnutrition was 0.9 (95% C.I.: 0.84, 0.91, p = 0.758) which could be subjected to sampling bias. We suggested those with severe cancer may be too weak to have health assessment in MIHC, thus the number of cases was few in the database. For those having cardiovascular diseases, the relative risk of them to be malnutrition was equal to those not having cardiovascular diseases (RR = 1.0, 95% C.I.: 0.86, 1.06, p = 0.296). However, those having cardiovascular diseases in the young old were found less risk as compared with those not having the diseases (Table 3). For those having respiratory diseases, their relative risk to be malnutrition was significantly higher than those not having the diseases (RR = 1.1, 95% C.I.: 1.00, 1.18, p = 0.037). The risk of being malnutrition for the respiratory disease group significantly increased (RR = 1.2, 95% C.I.: 0.98, 1.37, p = 0.049) in the young old with confounding age.
Table 2. Measures of association of risk factors on nutritional status by MNA, with confounding by age.
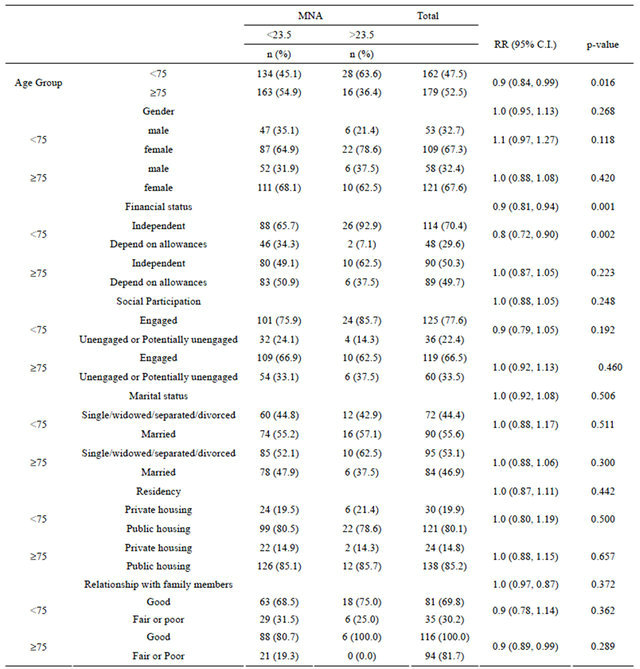
Participants living in nursing home or elderly homes were excluded in data analysis. MNA = Mini Nutritional Assessment; RR = relative risk; C.I. = confidence interval.
Table 3. Measures of association of diseases on nutritional status by MNA, with confounding by age.
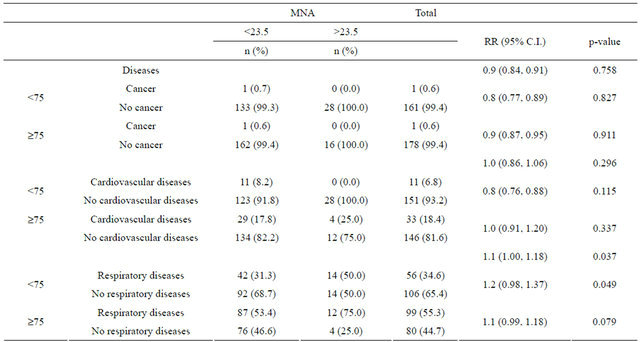
MNA = Mini Nutritional Assessment; RR = relative risk; C.I. = confidence interval.
5. DISCUSSION
Current literature did not have much data on the prevalence of malnutrition in the community-dwelling old adults. This study confirmed a low rate of malnutrition but a high rate of at risk malnutrition found among the older population in a urban city. More than 80% of the male and female participants were found to have risk at malnutrition, reflecting an urgent need for the Health Department to include nutritional care in its policy planning. However, policymakers should not attempt to remedy this issue using a “cure and treatment” approach. The problem of malnutrition risk among the older population may be a psycho-social-nutritional consequence of an individual’s context, rather than simply nutritional intake. Therefore, it is worth identifying the relevant psychosocial factors that may influence the nutritional status of older persons before recommending a supported nutritional strategy.
The results of this study showed that age advancement affected the participants’ nutritional status as assessed by the MNA score. The strength of association in the cut-off point of age 75 was significantly high. This confirmed the older olds in the community may have difficulty in sufficient nutrient intake, especially the protein intake as assessed by MNA scores. The socioeconomic factors explored in this study possibly provide some explanations to the risk of malnutrition in the old population living in the community. It was found that those depending on allowances, unengaged or potentially unengaged young old group were at higher risk of malnutrition than their counterparts. This provided some insights in the vulnerability of socially unengaged young old in maintaining sufficient nutrition values and there could possibly lack of nutrition support from the community network. The statistical significance in financial status also shed light on the strength of association in the policy of allowance and the nutritional status. With limited budget, the old population may not put food expense on the top priority and this eventually made them more hazardous with risk of malnutrition.
In addition to the socioeconomical findings, the results found that marital status and type of residency contributed little observable effect on the risk of malnutrition. This indicated marriage was not a main nutrition support in regards to have sufficient nutrients and public housing could be a good subsidized living for the older group. The expenditure of rent in public housing was low, to which the older group living there had similar budget allocation than those living in private housing, and this may need further research for investigation.
The results revealed that if the older adults had good relationship with their family members, they were prone to less risk of malnutrition. The findings were similar in both young old and older old, giving positive indication on the family support was critical factor in preventing malnutrition in the old aged group.
In regards to the disease factors, respiratory disease was found to have a significant negative effect on nutritional status. This confirms the finding of Lee et al. [8] that chronic lung disease is a significant risk for malnutrition among older aged populations. In this study, the risk for malnutrition was found higher if the old person was younger than age 75. This could be due to the complications related to the respiratory diseases which caused poor appetite in food intake.
6. LIMITATION OF STUDY
Since the study is a secondary analysis of health profile assessed for the older adults living in the community, the study design did not include food security factors such as food availability, food access, and food use. However, this study provided statistical evidence in the risk of malnutrition and the possibly socioeconomic factors associated with it. The findings could lead to further research to explore how food security affect nutritional risk.
7. IMPLICATIONS FOR PRACTICE
Numerous studies have shown that malnutrition affects clinical outcomes, prevents older patients from achieving rehabilitation, and incurs high health service costs like increasing hospital admission rates and lengthening hospital stay [22]. With the factors identified in this study, it provides specific older sector who is vulnerable to nutritional risk at the prevention stage. Accordingly, community nurses and social workers could blend the explored factors into community planning of holistic old aged care.
8. CONCLUSION
Older adults aged 75 or above were found to be at risk of being malnutrition. Special attention should be taken to those potentially unengaged, living on allowances, had fair or poor relationships with family members and those had respiratory diseases as they are prone to develop malnutrition.
9. ACKNOWLEDGEMENTS
The community centre was funded by the philanthropist Mr. Edwin S.H. Leong.
REFERENCES
- Zedlewski, S.R. and Schaner, S.G. (2005) Older adults’ engagement should be recognized and encouraged. The Retirement Project—Perspectives on Productive Aging. http://www.urban.org
- Centre for Integrative Digital Health (2008) Leong mobile integrative health centre. Quarterly Report, Q2. http://myweb.polyu.edu.hk/~hscidh/MIHCpublications/Quarterly%20Report%202.pdf
- Central Policy Unit, Hong Kong Special Administrative Region (2008) A qualitative study on “hidden elderly” in Hong Kong. The Chinese University of Hong Kong, Hong Kong.
- Seeman, T. (2000) Health promoting effects of friends and family on health outcomes in older adults. American Journal of Health Promotion, 14, 362-370. doi:10.4278/0890-1171-14.6.362
- Holt-Lunstad, J., Smith, T.B. and Layton, J.B. (2010) Social relationships and mortality risk: Meta-analytic review. PLOS Medicine, 7, Article ID: el000316. doi:10.1371/journal.pmed.1000316
- Shum, N.C., Hui, W.W.H., Chu, F.C.S., Chai, J. and Chow, T.W. (2005) Prevalence of malnutrition and risk factors in geriatric patients of a convalescent and rehabilitation hospital. Hong Kong Medical Journal, 11, 234- 242.
- Feldblum, I., German, L., Castel, H., Harman-Boehm, I., Bilenko, N., Eisinger, M., Fraser, D. and Shahar, D.R. (2007) Characteristics of undernourished older medical patients and the identification of predictors for undernutrition status. Nutrition Journal, 6, 37-45. doi:10.1186/1475-2891-6-37
- Lee, C.K.L., Kong, B.M.H., Chan, E.L.W. and Ku, P.S.M. (2000) The prevalence and risk factors of protein-energy malnutrition in three different institutions for elderly Chinese in Hong Kong. Journal of the Hong Kong Geriatric Society, 10, 5-9.
- Saletti, A., Johansson, L., Yifter-Lindgren, E., Wissing, U., Osterberg, K. and Cederholm, T. (2005) Nutritional status and a 3-year follow-up in elderly receiving support at home. Gerontology, 51, 192-198. doi:10.1159/000083993
- Neumann, S.A., Miller, M.D., Daniels, L. and Crotty, M. (2005) Nutritional status and clinical outcomes of older patients in rehabilitation. Journal of Human Nutrition and Dietetics, 18, 129-136. doi:10.1111/j.1365-277X.2005.00596.x
- Visvanathan, R., Macintosh, C., Callary, M., Penhall, R., Horowitz, M. and Chapman, I. (2003) The nutritional status of 250 older Australian recipients of domiciliary care services and its association with outcomes at 12 months. Journal of the American Geriatric Society, 51, 1007-1011. doi:10.1046/j.1365-2389.2003.51317.x
- Gazzotti, C., Arnaud-Battandier, F., Parello, M., Farine, S., Seidel, L., Albert, A. and Petermans, J. (2003) Prevention of malnutrition in older people during and after hospitalization: Results from a randomized controlled clinical trial. Age and Ageing, 32, 321-325. doi:10.1093/ageing/32.3.321
- Tsai, A.C., Ku, P.Y. and Tsai, J.D. (2008) Populationspecific anthropometric cutoff standards improve the functionality of the mini nutritional assessment without BMI in institutionalized elderly in Taiwan. Journal of Nutrition Health and Aging, 12, 696-700.
- Kulnik, D. and Elmadfa, I. (2008) Assessment of the nutritional situation of elderly nursing home residents in Vienna. Food, Nutrition and Health Promotion, 52, 51-53.
- Guigoz, Y., Vellas, B. and Garry, P.J. (1996) Assessing the nutritional status of the elderly: The mini nutritional assessment as part of the geriatric evaluation. Nutrition Reviews, 54, S59-S65. doi:10.1111/j.1753-4887.1996.tb03793.x
- Vellas, B., Lauque, S., Andrieu, S., Nourhashemi, F., Rolland, Y., Baumgartner, R. and Garry, P. (2001) Nutrition assessment in the elderly. Current Opinion in Clinical Nutrition & Metabolic Care, 4, 5-8. doi:10.1097/00075197-200101000-00002
- Thomas, D.R., Zdrowski, C.D., Wilson, M.M., Conright, K.C., Lewis, C., Tariq, S. and Morley, J.E. (2002) Malnutrition in subacute care. American Journal of Clinical Nutrition, 75, 308-313.
- Saletti, A., Lindgren, E.Y., Johansson, L. and Cederholm, T. (2000) Nutritional status according to mini nutritional assessment in an institutionalized elderly population in Sweden. Gerontology, 46, 139-145. doi:10.1159/000022149
- Hui, W.H., Law, C.B., So, K.Y., Wong, S.L., Chan, V., Kan, I., Lo, Y.M. and Li, E. (2001) Validating a modified version of the mini-nutritional assessment in institutionalized elderly Chinese People. Hong Kong Journal of Gerontology, 15, 35-43.
- World Health Organization (2000) The Asia-Pacific perspective: Redefining obesity and its treatment. Health Communications Australia, Melbourne.
- Brantervik, A.M., Jacobsson, I.E., Grimby, A., Wallen, T.C.E. and Bosaeus, I.G. (2005) Older hospitalized patients at risk of malnutrition: Correlation with quality of life, aid from the social welfare system and length of stay? Age and Ageing, 34, 444-449. doi:10.1093/ageing/afi125
- Sandars, J. (2002) The importance of nutrition in the elderly: Evidence based approach. Geriatric Medicine, 32, 35-38.