International Journal of Otolaryngology and Head & Neck Surgery
Vol.3 No.4(2014), Article
ID:47536,5
pages
DOI:10.4236/ijohns.2014.34030
Single Flap Otoendoscopic Myringoplasty for Large Central Perforation—A Pilot Study
Vikram Kulkarni*, Mudit Mittal
Department of Otorhinolaryngology, Chirayu Medical College and Hospital, Bhopal, India
Email: *drvikubaba@hotmail.com
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 20 April 2014; revised 19 May 2014; accepted 18 June 2014
ABSTRACT
Introduction: Otoendoscopic myringoplasty has been successfully used for repair of small to medium sized perforation using various materials. Very few studies have used this method for repair of large central perforation. Goals: To evaluate the transcanal otoendoscopic approach to reconstruct large central perforation by raising single flap. Methods Utilized: Pilot study on forty patients with chronic suppurative otitis media dry stage with large central perforation in medical college hospital and research centre was conducted. A zero degree 4 mm otoendoscope and custom made suction elevator was used for myringoplasty. Results: The perforation of thirty eight patients had healed by the end of two months. Conclusion: Otoendoscopic myringoplasty is effective in managing large central perforation and patients need to be observed for longer period to calculate the successful rate.
Keywords:Endoscope, Tympanic Membrane, Perforation, Otitis Media

1. Introduction
Myringoplasty is one of the frequently undertaken procedures for the treatment of chronic suppurative otitis media. The procedure can be performed in 3 different ways, viz., post aural approach, endaural approach, and endomeatal approach with use of operating microscope. Endoscopic approach to the middle ear is a recent concept and it is minimally invasive. Otoendoscope has advantages of better visualization of the middle ear structures and greater degree of freedom in negotiating the external auditory canal bulges [1] [2] . It has been successfully used in reconstruction of small to medium sized perforation [3] [4] and very few numbers of large central perforation are taken up for otoendoscopic myringoplasty with tympanomeatal flap elevation. Here we performed the otoendoscopic myringoplasty technique for the patients with chronic suppurative otitis media with large central perforation with good graft take up rate.
2. Methods
A total number of 40 patients who came with chronic suppurative otitis media with large central perforation were selected for the study. All these patients underwent otoendoscopic myringoplasty during the period from June 2012 to December 2012. The criterion for inclusion included dry stage of chronic suppurative otitis media, central perforation with more than 50 percent involvement of the pars tensa, hearing loss of not more than 50 dB. All the subjects underwent detailed endoscopic examination and the finging were carefully documented (Figure 1). The preoperative endoscopic examination revealed that none of the patients had active mucosal disease at the time of surgery.
Surgical Technique
All selected patients underwent the procedure under general anaesthesia. Using a zero degree otoendoscope, an endomeatal circumferential incision was made 6 mm from the tympanic annulus, single tympanomeatal was elevated from the underlying bone and annulus was lifted from the sulcus (Figure 2 and Figure 3). The entire flap was elevated from inferior to superior till the flap is having a pedicle attached to the superior canal skin. Care is taken to separate the skin from the underlying mucosa so that the graft replaces the fibrous middle layer
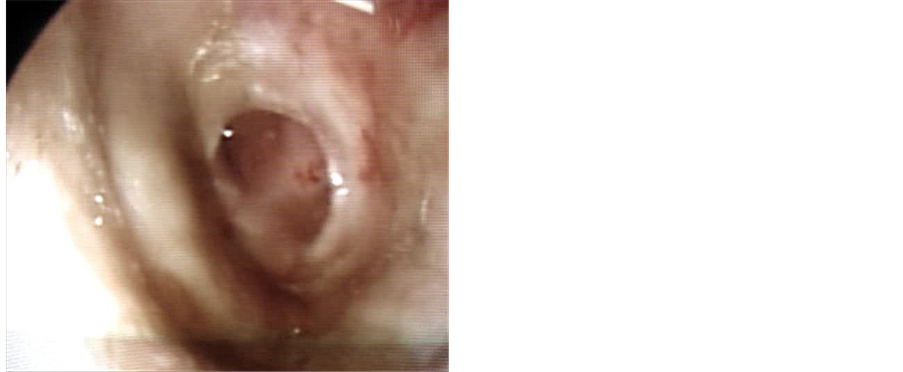
Figure 1. Large central perforation.
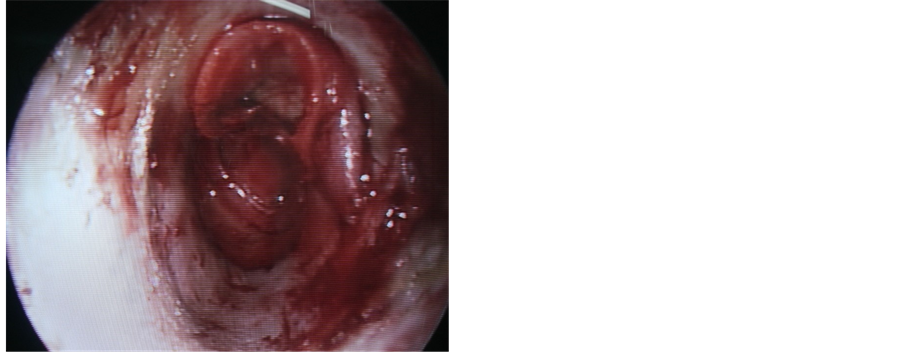
Figure 2. Partially elevated TM flap.
of the tympanic membrane. The middle ear was inspected for any epithelial residue and ossicular mobility was confirmed by eliciting round window reflex. Temporal fascia graft or perichondrum was used as graft material. The Middle ear was filled with gel foam and the flap was repositioned appropriately all over the circumference to overlap the graft material (Figure 4). External auditory canal was packed with medicated gel foam and a small cotton pack was placed over the gel foam for 5 days. After 5 days, external cotton pack was removed and instructed the patient to avoid entry of water in the ear for another 10 days. After about another 15 days patient was followed and external auditory canal was cleaned of remaining gel foam and the neodrum was examined using endoscope (Figure 5). All the patients underwent audiometry evaluation at the end of 2nd month.
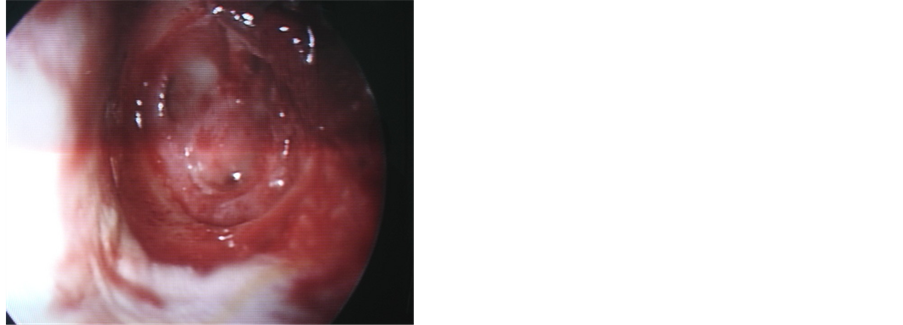
Figure 3. Completely elevated TM flap.
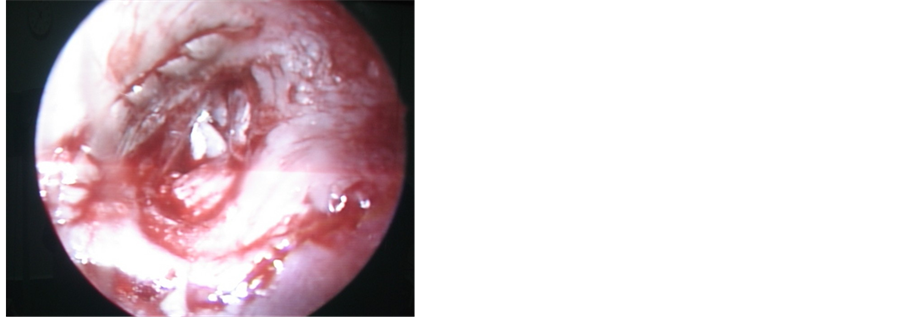
Figure 4. Graft positioned in place.
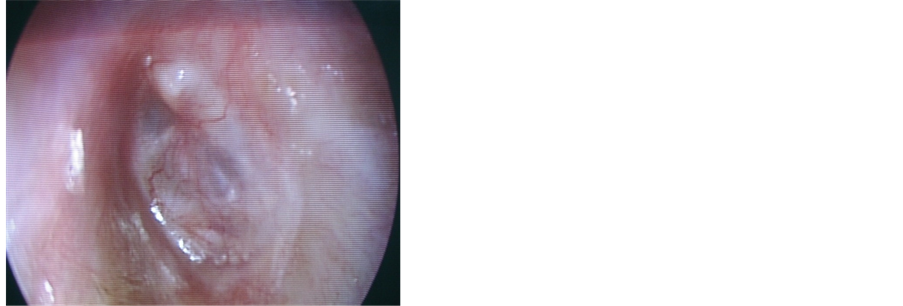
Figure 5. Healed perforation.
3. Results
Forty patients were categorized into 20 male patients and 15 female patients. Age of the patients ranged from 15 years to 55 years. All the patients had history of chronic ear discharge for more than 3 months. Age of the patients ranged from 15 years to 55 years. All patients had history of chronic ear discharge for more than 3 months duration with mean being 2 years. One patient had unhealed traumatic perforation.
A detailed ENT and head and neck examination confirmed the tympanic membrane perforation using zero degree 4 mm otoendoscope and hearing assessment was done with pure tone audiometry. Mean conductive hearing loss was 35 dB. None of the patients had sensorineural hearing loss. Active ear discharges of the patients were treated medically and allowed to remain dry for at least one month before taking up for operation.
Mean duration of the surgery was one hour. Thirty eight patients had their perforation closed at the end of one month. Two patients developed acute upper respiratory tract infection following which developed small central perforation and treated medically and had their perforation closed at the end of third month. At the end of three months all 38 patients were examined and pure tone audiometric investigation was done and mean air bone gap closure was within 25 dB.
4. Discussion
Otoendoscopic myringoplasty is a procedure which involves reconstruction of tympanic membrane. Initially otoendoscope was used as a diagnostic tool to closely inspect the tympanic membrane and the middle ear structures [5] . First use of the endoscope was done in the year 1967 by Mer et al. to examine the middle ear [6] . Later on with the advent of rigid Hopkins rod telescopes, otoendoscopes are now routinely used for the examination of the intact tympanic membrane and its abnormalities and middle ear surgeries [7] . However, in due course it was used as an alternative to the microscope in reconstruction of the tympanic membrane. There are basically 3 approaches to visualize the tympanic membrane, postaural, endaural, and transcanal. Of all these approaches used by the microscope, postaural and endaural approaches usually make an external incision and leave a scar and post operative morbidity [8] . Further, in selected cases with wide and straight external auditory canal the transcanal approach rendered no external scar and minimal morbidity post operatively.
Otoendoscope made this approach more popular in treatment of small central perforations with close inspection of the middle ear structures. In the literature, there are various graft materials that have been used for this method of transcanal endoscopic reconstruction of the tympanic membrane with small central perforation [4] [9] [10] [11] . There are very few reported cases in which the large central perforations are explored and reconstructed using the endoscope. Most suitable graft material for the reconstruction is either temporalis facia or perichondrium for large perforations. In majority of the endoscopic transcanal myringoplasty, endomeatal skin flap are not raised because of the technical difficulty with one had only free [12] . In our study we have also used a single flap technique to prepare the bed for the graft material. However, this can be overcome with suitable designed (Figure 6) suction elevator [13] .

Figure 6. Customised suction elevator.
Endoscope allows for better visualization and elevation of the skin and fibrous layer from the underlying mucosa. Because, remnant of the mucosa hinders the growth of the epithelium it should be meticulously separated from the overlying fibrous layer. The basic principle using superiorly based skin flap is its thickness which makes it stronger to reposition back over the graft [14] . Endoscope allows the graft to be secured firmly below the annulus entirely in the pars tensa area and placing the overlying gel foam.
5. Conclusion
Otoendoscope in recent days has been successfully used in the reconstruction of tympanic membrane, which is performed without the elevation of the tympanomeatal flap for small to medium sized perforations. In the present study, the otoendoscopic procedure is used for the closure of the large central perforations with endomeatal elevation of the tympanomeatal flap. This procedure is least morbid with early recovery. Further, the otoendoscopic procedure can be done by the properly designed custom made suction elevator which can overcome the restriction of one hand surgery.
Conflicting Interest
NIL.
Ethical Committee
Pilot study of myringoplasty surgeries with informed consent, full length of study is planned with ethical committee approval.
References
- Liu, Y., Sun, J.-J., Lin, Y.S., et al. (2010) Otoendoscopic Treatment of Hidden Lesions in Otomastoiditis. Chinese Medical Journal, 123, 291-295.
- Usami, S., Iijima, N., Fujita, S. and Takumi, Y. (2001) Endoscopic-Assisted Myringoplasty. Journal for Oto-Rhino-Laryngology and Its Related Specialties, 63, 287-290. http://dx.doi.org/10.1159/000055759
- Yadav, S.P.S., Aggarwal, N., Julaha, M., et al. (2009) Endoscopic Assisted Myringoplasty. Singapore Medical Journal, 50, 510.
- Karhuketo, T.S., Ilomäki, J.H. and Puhakka, H.J. (2001) Tympanoscope Assisted Myringoplasty. Journal for Oto-Rhino-Laryngology and Its Related Specialties, 63, 353-358. http://dx.doi.org/10.1159/000055773
- Rosenberg, S.I., Silverstein, H., Willcox, T.O. and Gordon, M.A. (1994) Endoscopy in Otology and Neurotology (English). The American Journal of Otology, 15, 168-172.
- Mer, S.B., Derbyshire, A.J., Brushenko, A. and Pontarelli, D.A. (1967) Fiberoptic Endoscopies for Examination of the Middle Ear. Archives of Otolaryngology, 85, 387-393. http://dx.doi.org/10.1001/archotol.1967.00760040389009
- El-Begermy, M. (2003) Endoscopic Assisted Stapedectomy. International Congress Series, 1240, 919-925. http://dx.doi.org/10.1016/S0531-5131(03)00687-3
- Coskun, B.U., Cinar, U., Seven, H., et al. (2006) The Effects of the Incision Types in Myringoplasty Operations on Cosmesis. European Archives of Otorhinolaryngology, 263, 820-822. http://dx.doi.org/10.1007/s00405-006-0069-z
- Harugop, A.S., Mudhol, R.S. and Godhi, R.A. (2008) A Comparative Study of Endoscope Assisted Myringoplasty and Microscope Assisted Myringoplasty. Indian Journal of Otolaryngology and Head & Neck Surgery, 60, 298-302. http://dx.doi.org/10.1007/s12070-008-0099-5
- Li, P., Yang, Q.-T., Li, Y.-Q., et al. (2010) The Selection and Strategy in Otoendoscopic Myringoplasty with Autologous Adipose Tissue. Indian Journal of Otolaryngology and Head and Neck Surgery, 62, 25-28.
- Alzoubi, F.Q., Tarifi, A.A., Khader, Y., et al. (2010) Comparison between Transtympanic and Elevation of Tympanomeatal Flap Approaches in Tympanoplasty. Otology & Neurotology, 31, 773-775. http://dx.doi.org/10.1097/MAO.0b013e3181e40a41
- Semenov, F.V. and Misiurina, Iu.V. (2010) Advantages and Disadvantages of the Application of Endoscopic Techniques at Different Stages of Tympanoplasty. Vestnik Otorhinolaryngologii, 6, 48-50.
- Raman, R. and Omar, R. (2011) Suction Elevator for Ear Surgery. Indian Journal of Otolaryngology and Head and Neck Surgery, 63, 302.
- Gupta, S.C. (2000) Myringoplasty with a Single Flap. Ear Nose Throat Journal, 946-951.
NOTES

*Corresponding author.