Surgical Science
Vol.4 No.2(2013), Article ID:27746,5 pages DOI:10.4236/ss.2013.42026
Salivary Gland Tumours at Komfo Anokye Teaching Hospital, Ghana
Komfo Anokye Teaching Hospital, Kumasi, Ghana
Email: *aotiacheampong@yahoo.com
Received November 20, 2012; revised December 22, 2012; accepted December 31, 2012
Keywords: Salivary; Gland; Pleomorphic; Benign
ABSTRACT
In African studies on salivary gland tumours, there are considerable epidemiological differences in different parts of the continent. There is no study of salivary gland tumours from the second largest hospital in Ghana, Komfo Anokye Teaching Hospital. Aim: This study was to look at the prevalence and demographic distribution of salivary gland tumours at the Komfo Anokye Teaching Hospital (KATH). Method: Histopathologically diagnosed salivary gland tumours of consecutive patients were evaluated. The study duration was from 1999 to 2010 October. Result: The total number of salivary gland tumours were 121. Male to female ratio was 1.75:1. Out of the total of 34 salivary malignancies seen, male to female ratio was 1.8:1. Malignant tumour was 28.1% while 71.9% were benign. Mean age for malignancy was 53.5 years (SD = 9.7) and that for benign was 35.5 years (SD = 8.2). Conclusion: The commonest benign tumour of the parotid was Pleomorphic adenoma (48.3%) which is consistent with most of the African and western reports. Warthin’s tumour prevalence was higher than most of the studies from Africa.
1. Introduction
Salivary gland neoplasms are remarkable for their histological diversity and pose a particular challenge to the pathologist because of their complex classification and the rarity of several varieties [1,2]. Most publications in the literature on major and minor salivary gland tumours, find it difficult to evaluate the real frequency and site distribution of salivary gland tumours [2,3]. They are relatively rare, accounting for approximately 2% to 10% of all head and neck tumours [4] worldwide and are more commonly found in the parotid gland.
In African studies on salivary gland tumours, there are considerable epidemiological differences in different parts of the continent. Studies in parts of Nigeria and other parts of Africa show salivary gland neoplasm to constitute between 2.8% and 10% of all Head and Neck malignancies [5,6]. There is no study of salivary gland tumours from the second largest hospital in Ghana, Komfo Anokye Teaching Hospital.
2. Method and Statistics
Histopathologically diagnosed salivary gland tumours of consecutive patients were retrieved from the hospital records and decoded to protect the identity of patients.
The study duration was from 1999 to 2010 October. Data was entered into Microsoft Excel and summarized as mean standard deviation for continuous variables and percentages for categorical variables.
3. Results
The total number of salivary gland tumours were 121 as presented in Table 1. Male to female ratio was 1.75:1. Out of the total of 34 salivary malignancies seen, male to female ratio was 1.8:1 (Table 2). Malignant tumour was 28.1% while 71.9% were benign as represented in Table 1. Mean age for malignancy (Table 2) was 53.5 years (SD = 9.7) and that for benign was 35.5 years (SD = 8.2).
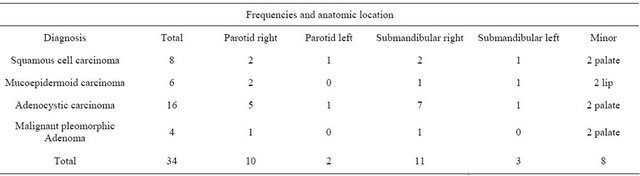
A total of 77 salivary tumours were seen in males (Tables 1 and 2) and 22 (29.3%) were malignant (Table 2). In females, out of the 44 cases, 12 (26.0%) were malignant (Table 2). The parotid was the commonest location of all salivary gland tumours (Table 3). The submandibular gland had more malignant tumours, representing 47.4% (Table 4). A total of 10 out of 38 tumours in the right parotid (Table 4) were malignant, representing 26% as against a total of eight out of 22 cases of the minor salivary glands being malignant, i.e. 36%. Six cases of the minor salivary gland malignancies representing 75% were located on the palate (Table 4).
Pleomorphic adenoma was the commonest salivary
Table 1. Sex and age distribution of salivary gland tumours.
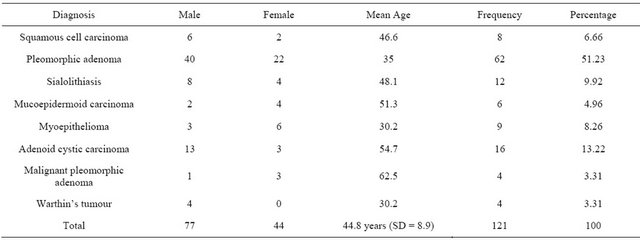
Table 2. Sex and age distribution of salivary gland malignancies.
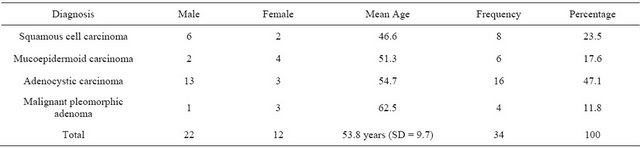
Table 3. Anatomic locations of benign salivary gland tumours.
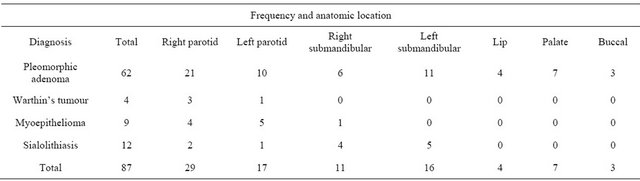
Table 4. Anatomic location of salivary gland malignancies.
gland tumour, constituting 50% of total salivary gland tumours and 69% of all the benign salivary gland tumours (Table 1). Warthin’s tumour constituted 3.3% of all salivary tumours (Table 1).The commonest malignant tumour was Adenoid cystic carcinoma (Table 2), which was 13.22%.
4. Discussion
The traditional distribution of salivary gland tumours between sites has followed a rule of 100:10:10:1 ratio for the parotid, submandibular, minor salivary glands and sublingual glands respectively. Many studies in Africa have demonstrated that this general distribution of site is not so typical of the African population.
5. Age and Sex Distribution
According to Table 1, 96% of patients were between second to sixth decades similar to what was seen by Otoh et al. [7]. Mean age for salivary malignancy was 53.5 years and that for benign was 35.5 years. The male to female ratio of all the salivary neoplasm was 1.6:1 and in terms of the malignancies was 1.8:1. The mean age of benign tumour was similar to that reported by Edda [8] of 38.1 years, which also male to female ratio of 1:1.3 compared to the 1.6:1 in this present study.
This sex distribution is consistent with most western [9] reports which gave equal sex distribution of malignant tumours although the incidence for salivary gland tumours show a male to female ratio of 1.3:1 [10]. Female predominance has also been seen in an African series [11].
6. Site Distribution
Apart from the sublingual gland that was not affected, all the major glands were involved. The percentage distribution according to Tables 3 and 4 was 47.9%, 32.9% and 18.9% for the parotid, submandibular and minor salivary glands respectively, giving approximate ratio of 3:2:1. This finding is slightly different from the Uganda [8] study which gave a ratio of almost 1:1:1 but similar to the study in Kano, Nigeria by Ochicha [12] which gave percentages of 49%, 26% and 24% respectively. In this study, 31.4% of tumours originated from the right parotid gland alone. This observation will need further investigations from other centres to ascertain the true anatomic distribution of parotid tumours.
7. Parotid Region
The parotid gland was the commonest site for salivary gland tumuors accounting for about 48% of all the Salivary gland tumours and similar to findings by Ochicha [12].The right side was more affected and accounted for 38% and 29% benign and malignant tumours respectively.
The commonest benign tumour of the parotid was Pleomorphic adenoma (48.3%) which is consistent with most of the African and western reports [4,10]. All the Warthin tumours also occurred in the parotid and this is also consistent with reports from the West [13] and Africa [10] respectively.
The commonest malignancy in this region was adenoid cystic carcinoma. This malignancy formed 47% of all the salivary gland malignancies and out of this, 37.5% occurred in the parotid gland alone of which 83% occurred in the right parotid. The right side of the parotid was more prone to neoplasm, a finding that is in agreement with another previous study in Ghana by Parkins [14]. The parotid was the site with most malignancies i.e. 47%, which is similar to some African [15] studies but higher than the 22% observed by Parkins [14].
8. Submandibular Region
A total of 40 cases were seen in this region representing 32.9%. There were 27 (67.55%) benign and 14 (35%) malignant tumours. Most (78.6%) of the malignant tumours occurred on the right side similar to the parotid region (Tables 3 and 4).
In terms of comparative analysis, of the total 34 malignant cases, 14 (41.2%) came from the submandibular gland, 12 (35.3%) and 8 (23.5%) parotid and minor Salivary glands respectively. This means that more malignant tumours were seen in the submandibular gland, which is the opposite of what was seen by Edda [8] in Uganda where more malignancies occurred in the parotid and minor salivary glands. However the finding is consistent with some western series [4].
9. Minor Salivary Glands
There were 22 minor salivary gland tumours, comprising of 18% of all salivary gland tumours. This was made up of 14 (63.6%) benign and 8 (36.4%) malignant tumours. All the benign tumuors were pleomorphic adenoma. The palate was the most common site and this is in agreement with some African study [10]. The percentage of malignancy in minor salivary glands out of the total salivary gland neoplasm was 6%, which is similar to 8% reported by Silas [11], from Jos University hospital in Nigeria.
The palate was the most commonly affected site of all the malignancies in the minor salivary glands, i.e. 6 (75%) out of the eight malignancies seen. This is slightly lower, compared to 87.5% of palatal malignancies seen by Otoh [16].
This means that in this study, the palate had a total of 13 (59%) of tumours, out of which 6 (46%) were malignant which is higher than the 23% observed by Parkins
[14]. Palatal tumours however represented only 10.7% of the tumours seen in this study, lower than Parkins [17] finding of 31%.
10. Benign Tumours
In a recent publication by Adeyemi [18], 62% of salivary gland tumours were malignant, while 38% were benign. In this study, benign tumours comprised 87 (71.9%). Pleomorphic adenoma was the commonest of all salivary gland tumours (50%) and 69% of all the benign salivary gland tumours.
This percentage of 69% occurrence is slightly higher than the 62% reported by Parkins [14]. Pleomorphic adenomas (50%) were mostly located in the parotid. This finding is consistent with most of the African including Kolude et al. [19], but lower than that by Masanja [20] in Tanzania 75%. The next significant finding in this study was the occurrence (3.3%) of Warthin’s tumour, which according to most Africa studies is rare.
Most of the studies in the West [13] and Asia [21] have observed that Warthin’s tumour is second to pleomorphic adenoma, usually in males and the parotid is the usual anatomic site. This finding calls for a review of most of the benign salivary tumour slides to know the actual occurrence of this tumour in the African population.
11. Malignant Tumours
There are varied reports about the commonest salivary gland malignancy. Whereas most studies in the West [4] and Asia [21] put Adenoid cystic carcinoma slightly ahead of mucoepidermoid carcinoma, in Africa [10] it is usually the opposite as in the study by Otoh et al. [7], in which Mucoepidermoid carcinoma (10.1%) was the most common salivary gland malignancy.
In this present study the commonest malignancy was adenoid cystic carcinoma and is comparable to a study in Ghana by Parkins. Most of the tumours were in the submandibular gland 14 (41.2%) followed by parotid 12 (35.2%) with about 65% mostly affecting right side of parotid and submandibular glands.
12. Conclusion
The parotid gland was the commonest site for salivary gland tumours. The commonest benign tumour of the parotid was Pleomorphic adenoma. The right side of the parotid was more prone to neoplasm. Warthin’s tumour prevalence was higher than most of the studies from Africa.
REFERENCES
- M. de L. S. de A. Morais, P. R. Azevedo, C. H. Carvalho, L. Medeiros, T. Lajus and A. de L. L. Costa, “Clinicopathological Study of Salivary Gland Tumors: An Assessment of 303 Patients,” Cadernos de Saúde Pública, Vol. 27, No. 5, 2011, pp. 1035-1040. doi:10.1590/S0102-311X2011000500020
- E. Ben Brahim, M. Ferchiou, O. Khayat, S. Zribi, C. M’barek, N. Labbène, A. El Khedim, M. Ben Ayed and A. Chadli-Debbiche, “[Tumors of Salivary Glands: Anatomical Study and Clinical Epidemiology of a Series of 180 Cases],” La Tunisie Medicale, Vol. 88, No. 4, 2010, pp. 240-244.
- M. de L. S. de A. Morais, P. R. Azevedo, C. H. Carvalho, L. Medeiros, T. Lajus and A. de L. L. Costa, “Clinicopathological Study of Salivary Gland Tumors: An Assessment of 303 Patients,” Cadernos de Saúde Pública, Vol. 27, No. 5, 2011, pp. 1035-1040. doi:10.1590/S0102-311X2011000500020
- A. V. Jones, G. T. Craig, P. M. Speight and C. D. Franklin, “The Range and Demographics of Salivary Gland Tumours Diagnosed in a UK Population,” Oral Oncology, Vol. 44, No. 4, 2008, pp. 407-417. doi:10.1016/j.oraloncology.2007.05.010
- A. L. Ladeinde, W. L. Adeyemo, M. O. Ogunlewe, O. F. Ajayi and O. G. Omitola, “Salivary Gland Tumours: A 15-Year Review at the Dental Centre Lagos University Teaching Hospital,” African Journal of Medicine and Medical Sciences, Vol. 36, No. 4, 2007, pp. 299-304.
- B. Kolude, J. O. Lawoyin and E. E. Akang, “Salivary Gland Neoplasms: A 21-Year Review of Cases Seen at University College Hospital, Ibadan,” African Journal of Medicine and Medical Sciences, Vol. 30, No. 1-2, 2001, pp. 95-98.
- E. C. Otoh, N. W. Johnson, H. Olasoji, I. S. Danfillo and O. A. Adeleke, “Salivary Gland Neoplasms in Maiduguri, North-Eastern Nigeria,” Oral Diseases, Vol. 11, No. 6, 2005, pp. 386-391. doi:10.1111/j.1601-0825.2005.01137.x
- E. A. M. Vuhahula, “Salivary Gland Tumors in Uganda: Clinical Pathological Study,” African Health Sciences, Vol. 4, No. 1, 2004, pp. 15-23.
- P. M. Speight and A. W. Barrett, “Salivary Gland Tumours,” Oral Diseases, Vol. 8, No. 5, 2002, pp. 229-240. doi:10.1034/j.1601-0825.2002.02870.x
- M. A. Yaor, “The Pattern of Presentation of Salivary Gland Tumors in Africa: A Review of Published Reports,” Ear, Nose & Throat Journal, Vol. 89, No. 2, 2010, pp. E17-E21.
- O. A. Silas, G. O. Echejoh, A. N. Manasseh and B. M. Mandong, “Patterns of Malignant Salivary Gland Tumours in Jos University Teaching Hospital (JUTH), Jos: A Ten-Year Retrospective Study,” Nigerian Journal of Medicine, Vol. 18, No. 3, 2009, pp. 282-285.
- O. Ochicha, S. Malami, A. Mohammed and A. Atanda, “A Histopathologic Study of Salivary Gland Tumors in Kano, Northern Nigeria,” Indian Journal of Pathology & Microbiology, Vol. 52, No. 4, 2009, pp. 473-476. doi:10.4103/0377-4929.56121
- A. Faur, E. Lazăr, M. Cornianu, A. Dema, C. G. Vidita and A. Găluşcan, “Warthin Tumor: A Curious Entity— Case Reports and Review of Literature,” Romanian Journal of Morphology and Embryology, Vol. 50, No. 2, 2009, pp. 269-273.
- G. Parkins and M. O. Boamah, “Tumours of Salivary Gland in Ghana,” Asian Journal of Oral Maxillofacial Surgery, Vol. 21, 2009, pp. 96-100.
- M. K. A. Kayembe and M. M. R. Kalengayi, “Salivary Gland Tumours in Congo (Zaire),” Odontostomatologie Tropicale, Vol. 25, No. 99, 2002, pp. 19-22.
- E. C. Otoh, N. W. Johnson, H. O. Olasoji, I. S. Danfillo and O. A. Adeleke, “Intra-Oral Carcinomas in Maiduguri, North-Eastern Nigeria,” Oral Diseases, Vol. 11, No. 6, 2005, pp. 379-385. doi:10.1111/j.1601-0825.2005.01134.x
- G. E. Parkins, G. A. Armah and Y. Tettey, “Orofacial Tumours and Tumour-Like Lesions in Ghana: A 6-Year Prospective Study,” British Journal of Oral and Maxillofacial Surgery, Vol. 47, No. 7, 2009, pp. 550-554. doi:10.1016/j.bjoms.2008.11.003
- B. F. Adeyemi, G. O. Ogun and E. E. Akang, “Retrospective Analysis of Intra-Oral Salivary Gland Tumours in Ibadan, Nigeria,” West African Journal of Medicine, Vol. 29, No. 2, 2010, pp. 98-103.
- B. Kolude, J. O. Lawoyin and E. E. Akang, “Mucoepidermoid Carcinoma of the Oral Cavity,” Journal of the National Medical Association, Vol. 93, No. 5, 2001, pp. 178-184.
- M. I. Masanja, B. M. Kalyanyama and E. N. M. Simon, “Salivary Gland Tumours in Tanzania,” East African Medical Journal, Vol. 80, No. 8, 2003, pp. 429-434.
- K. Subhashraj, “Salivary Gland Tumors: A Single Institution Experience in India,” British Journal of Oral and Maxillofacial Surgery, Vol. 46, No. 8, 2008, pp. 635-638. doi:10.1016/j.bjoms.2008.03.020
NOTES
*Corresponding author.