Open Journal of Stomatology
Vol.04 No.09(2014), Article ID:49545,10 pages
10.4236/ojst.2014.49061
Phenytoin Effects on Proliferation and Induction of IL1β and PGE
Surena Vahabi1, Masomeh Moslemi2, Bahareh Nazemisalman3*, Zahra Yadegari4
1Periodontics Department, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Pedodontic Department, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Pedodontic Department, Dental School, ZUMS, Zanjan, Iran
4Biotechnology, Shahid Beheshti Medical University, Tehran, Iran
Email: Ivsure1@gmail.com, masume_moslemi@yahoo.com, *Nazemisalmanb@yahoo.com, z_yadegary@yahoo.com
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 1 July 2014; revised 19 August 2014; accepted 31 August 2014
ABSTRACT
Background: Gingival Overgrowth (GO) is a well documented and unwanted side effect that occurs mainly as a result of certain antiseizure, phenytoin. The aim of this study was to compare the ef- fect of phenytoin on proliferation and production of IL1β and PGE
Keywords:
Phenytoin, Gingival Overgrowth, Fibroblast, Interleukin, Children

1. Introduction
Medication-induced gingival overgrowth (GO) is a common subsequent of consuming anti-epileptic drug, im- munosuppressive drug, and calcium-channel-blockers [1] . This side-effect may cause delayed eruption of teeth and disturbances in speech, mastication, and aesthetic [2] . The highest prevalence of gingival overgrowth has been reported to be occurred in the anti-epileptic drugs group [3] , which is one of the most influent drugs on central nervous system, and other than seizure, is widely prescribed in cases of psychiatric disorders, migraine prophylaxis, and neuropathic pain [4] . Phenytoin is an anti-epileptic drug, which is vastly used solely or in com- bination with other drugs. Some advantages include a maximum anti-epileptic effect without suppressing central nervous system, availability, low cost and periodic use [5] . Nevertheless, skeletal, endocrine, immunological and connective tissue disturbances are some of reported side-effects of phenytoin [6] . Gingival overgrowth, first re- ported in 1939 [7] , is one of the most known side-effects of phenytoin that occurs in nearly 50% of consumers [8] . According to epidemiologic studies, it is more prevalent in male children [9] -[11] and adolescents [12] -[14] . Use of alternative drugs such as valproic acid and carbamazepine [14] [15] , proper oral hygine [16] -[18] , gingi- vectomy and periodontal flap are the common methods of prevention and treatment of gingival overgrowth [19] . However, phenytoin-induced pathogenesis is unknown, and it might recur 3 to 6 months following periodontal surgery [20] .
Several mechanisms such as functional heterogeneity of the human gingival fibroblast, [21] accumulation of extracellular matrix (ECM) proteins such us collagen, [21] -[23] impaired homeostasis in the connective tissue, increase production of glycosaminoglycans, [3] disturbances in secretion of ECM enzymes such as Matrix Metallo Proteinases (MMPs), and tissue inhibitors [24] -[26] have been recognized for this overgrowth in previous studies. Recent studies have suggested that impaired balance of cytokines plays a major role in gingival over- growth. This impaired balance has been attributed to local alterations of fibrogenic cytokines such as Tumor Necrosis Factor-α (TNF-α) and various interleukins such as Interleukin-1 (IL-1) in response to phenytoin [3] [14] [27] . IL-1 is a part of cytokine family in inflammatory lesions, which is capable of stimulating bone resorption as well as biosynthesis of Prostanoids and enhancing extracellular matrix synthesis and collagenase in human gingival fibroblasts [28] .
Brunius et al. have showed that phenytoin increases the production of interleukin-1β (IL-1β), and Prostaglan- din E2 (PGE2) which has been induced by TNF-α; and have suggested that PGE2 and IL-1β play a key role in pathogenesis of phenytoin-induced gingival overgrowth [29] . Tumor necrosis factor (TNF-α), an inflammatory cytokine, induces cellular proliferation and inhibits synthesis and phagocytosis of collagen by human gingival fibroblasts [30] . This factor has been shown to stimulate IL-1α production. Researchers have suggested that these cytokines might induce the production and secretion of collagenase, which is a necessary enzyme in ECM breakdown [31] . It is still unknown that how TNF-α and IL-1 manage such contrasting functions in breaking down and producing gingival matrix and collagen metabolism in drug-induced overgrowth [29] . Moreover, the nature of inflammatory lesions in pediatrics is different from that in adults [32] -[34] . According to Gillet, B-small lymphocytes do not change form, and constitute the majority of inflammatory infiltrates. In result, clini- cal lesions remain unaggressive and undeveloped. It is a phenomenon that might be the combination in cell in- filtrate in latent lesions of adults [35] [36] . According to Longhorst et al. [37] and Seymour et al. [38] , cell infil- trations is predominantly constituted of T cells, and when the lesions become aggressive, the infiltration of B cells increases.
There is little known about the reasons for the differences in gingival overgrowth prevalence in pediatrics and adults, and also about the details of phenytoin and inflammatory mediators in these two groups. According to this lack of knowledge, prevalent usage of phenytoin in treatment of central nervous system diseases [39] and seizure, particularly in pediatrics, and with regard to the main role of fibroblasts in phenytoin-induced gingival overgrowth and in producing inflammatory mediators and ECM and in regulating collagen metabolism [19] , this study was performed to investigate the influence of phenytoin on proliferation of fibroblasts and production of inflammatory mediators, IL1β and PGE2, by gingival fibroblasts in adults and pediatrics.
2. Materials and Methods
2.1. Cell Culture
The pediatric samples were obtained from 4 healthy children, aging from 4 to 11 years, during a procedure of the mesiodense or impacted canine teeth whom have been referred due to orthodontic treatments. In addition, adult fibroblast samples were derived from 4 healthy adults who were submitted to crown lengthening surgery. The age range was 35 - 42 years. All of the persons were in good periodontal, oral and systemic health situation without any signs of inflammations in the site of biopsies. Pregnant women, addicted persons, systemic drug us- ers and any person with systemic diseases which might have any effects on periodontium were excluded from the study. Due to natural constraints in primary cell culture, some pediatric samples were lost during in the ex- periment, so that 22 adult samples and 19 pediatric samples were obtained in total. In both cases, a fragment of excess tissue was removed under local anesthesia at the moment of the surgery. Informed consent was obtained from each donor prior to the taking of samples and parent of each child was informed about the study and con- sent forms were signed by them. Experimental protocol was approved by the Ethics Committee in Shahid Be- heshti Medical University. The tissues were rinsed three times in sterile normal saline solution and transported in complete media including: Dulbecco’s Modified Eagle’s Medium (DMEM; Gibco USA) supplemented with 10% fetal bovine serum (FBS; Gibco USA), 100 μg/ml streptomycin, 100 U/ml penicillin and 0.25 μg/ml Am- photericin B. Minced pieces of the tissue were explanted to 4 cm2 plates, and incubated at room temperature for 10 - 15 minutes and then the culture plate was flooded with complete media. Then samples were incubated at 37˚C in a humidified incubator containing 5% CO2. Samples were regularly controlled for contamination and cell growth, and were fed with fresh medium if necessary. When fibroblasts grew out from the explants, they were trypsinized and shifted to
2.2. Enzyme-Linked Immunosorbent Assay (
Gingival fibroblasts were seeded into 24-well plates (Nunc, Copenhagen, Denmark) at a density of 60 × 103 cells/well. For every individual fibroblast derived samples 6 wells were cultured but due to natural constraints in primary cell culture, several pediatric samples were lost during in the experiment, so that 22 adult samples and 19 pediatric samples were obtained in total. Wells were divided into control and experimental groups (3 wells for each group or triplicate). After 48 hours, the media of cell cultures was exchanged and Phenytoin (Sigma- Aldrich, St. Louis, MO, USA) (20 μg/ml) was added to the experimental wells and in control groups only com- plete media was added. Samples were then incubated at 37˚C in 95% humidified atmosphere containing CO2 for 48 hours.
In order to assess the amount of inflammatory mediators produced by gingival fibroblasts, supernatant fluid of each control and experimental well was collected. The concentration of PGE2, IL-1β was determined by En- zyme-Linked Immunosorbent assay (ELISA) using the ELISA kits [PGE2 (R & D systems, Minneapolis, MN, USA Cat No. KGE004B)]. IL-1β (R & D systems, Minneapolis, MN, USA Cat No. DLB50).
2.3. MTT Assay
Gingival fibroblasts were seeded into 96-well plates (Nunc, Copenhagen, Denmark) at a density of 5 × 103 cells/ well, and were cultured in a 200 μl medium. For every individual fibroblast derived samples 6 wells were cul- tured. After 48-hour incubation, the samples were divided into control and experimental groups (3 wells for each group or triplicate). Phenytoin was added to the experimental wells. MTT stock solution [tetrazolium salt 3-[4, 5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide (MTT; Merk, Darmstadt, Germany)] was prepared in phosphate-buffer saline (PBS; Sigma-Aldrich, St. Louis, MO, USA) in proportion to 5 mg/ml. After 48 hours of incubation, the medium was replaced with 200 μl of a fresh medium containing a final concentration of MTT salt as 0.5 mg/ml. Cells were then incubated at 37˚C in 95% humidified atmosphere containing CO2 for 4 hours. Acidic Isopropanol (
2.4. Statistical Analysis
Data which has been released by ELISA were then tested by Kolmogrov Simonov test to evaluate normal dis- tribution of adult and pediatric gingival cell population. (Mean value of triplicate was calculated and every indi- vidual experiment and related control data were compared). ANOVA was used for statistical evaluation. Results between the two groups were compared by student’s T-test. p value < 0.05 was considered statistically signifi- cant.
3. Results
3.1. Rate of Fibroblast Proliferation in Adults and Pediatrics
Rate of fibroblast proliferation in both adults and pediatrics groups increased in the presence of phenytoin. How- ever, these changes did not reach a significant level. The difference between phenytoin-induced proliferation in adults group and in pediatrics group was not significant (Graph 1).
3.2. Synthesis of IL1β by Adults and Pediatrics Fibroblasts
Phenytoin did not cause a significant raise in synthesis of IL-1β in adult fibroblasts. In contrast, the pheny- toin-induced synthesis of IL-1β significantly increased in pediatric fibroblasts (p < 0.05). The change in produc- tion of IL-1β caused by presence of phenytoin was significantly higher in pediatrics than that in adults group (p < 0.05) (Graph 2).
3.3. Synthesis of PGE2 by Adults and Pediatrics Fibroblasts
In the adults group, the level of synthesized PGE2 decreased in presence of phenytoin, but this reduction did not reach a significant level. The production of PGE
4. Discussion
In this study, no significant increase was perceived in the rate of proliferation of pediatrics and adults fibroblasts after exposure to phenytoin. Also, the rate of proliferation was not significantly different between adults and pe- diatrics. In agreement with our results, Hassel et al. [21] and Vamada et al. [22] have also reported that no sig- nificant increase is perceived in levels of hyperplasia in treated fibroblasts. In contrast, Al-Ubaidy et al. [40] have shown that phenytoin significantly increases the mitotic activity and mitotic index of gingival fibroblasts. Another study performed on
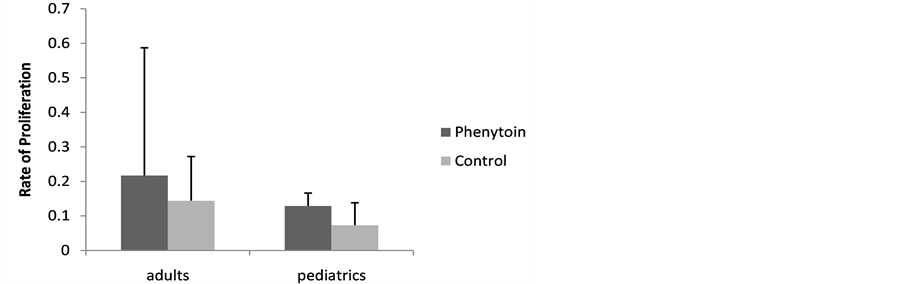
Graph 1. Rate of proliferation (mean + standard deviation) in adult and pediatric fibroblasts in both control group and phenytoin-treated group.
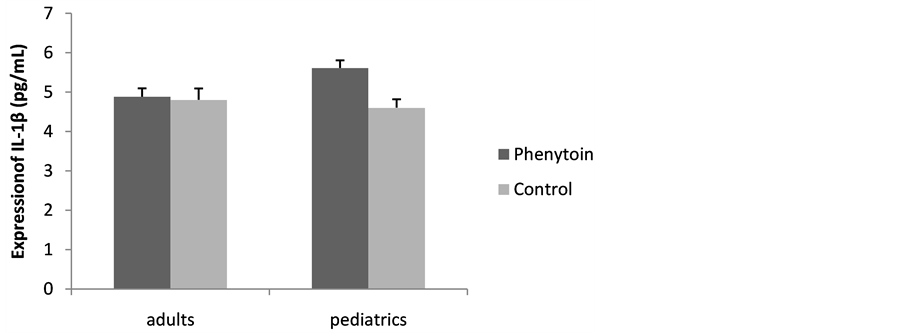
Graph 2. The expression of released IL-1β (mean + standard deviation) in adult and pediatric fibroblasts in both control group and phenytoin-treated group.
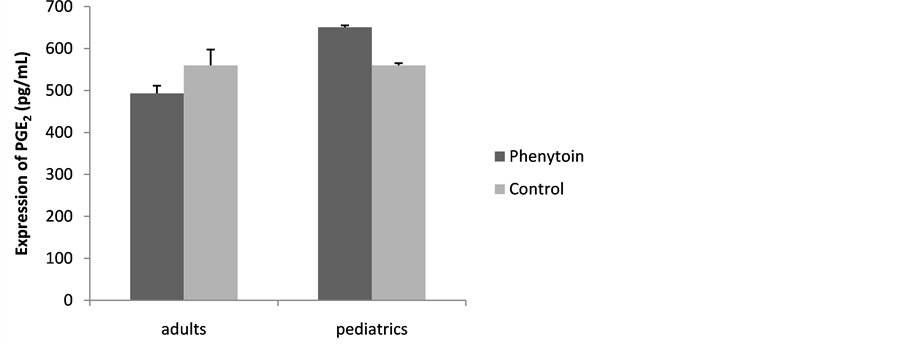
Graph 3. The expression of released PGE2 (mean + standard deviation) in adult and pediatric fibroblasts in both control group and phenytoin-treated group.
Phenytoin stimulated pediatrics fibroblasts to produce more levels of IL1β. However, in the adults group, no significant change was perceived. The study of Modeer et al. [30] agrees with our results, and also shows that the inhibitive effect of IL-1β on expression of collagen genes increases in presence of phenytoin. One other study has showed that the simultaneous presence of TNF-α and phenytoin stimulates the production of IL-1α by fibroblasts and suggested that the simultaneous presence of three inflammatory mediators, TNF-α, IL-1α, and PGE2, could raise the effects of collagenase enzyme [43] . Brunius et al. [29] have proposed that phenytoin can- not stimulate the IL-1β production solely, and that the concurrent presence of TNF-α is necessary for inducing IL-1β and PGE2 production.
In this study, after exposure to phenytoin, pediatric fibroblasts produced higher levels of PGE2; while in adults group, the PGE2 production decreased. Levels of produced PGE2 by treated pediatric fibroblasts were sig- nificantly higher than those by treated adult’s fibroblasts. These results are consistent with Modeer et al., who have shown the increase in PGE2 production of treated fibroblasts in both in vitro [44] and in vivo [45] studies. In the in vitro study, the concurrent presence of IL-1β and TNF-α was necessary for PGE2 production by treated fibroblasts [46] ; however, in an in vivo case, the PGE2 production occurred with or without existence of IL-1β and TNF-α [43] . Since phenytoin is capable of regulating intracellular Ca2+, and since phospholipase A2 is a Ca2+ related enzyme, the higher levels of PGE2 production has been attributed to the increased activity of A
It seems that several mechanisms such as increased inflammatory activities and altered immunological pro- cesses and disturbed homeostasis of cytokines, as well as secretion of inflammatory mediators as TNF-α, PGE2; and IL-1β, could affect the gingival fibroblasts and cause some disturbances in ECM homeostasis, in cell proli- feration, and in homeostasis of connective tissue proteins. Studies have reported that phenytoin causes distur- bance in cell population, which subsequently results in alternations in production of growth factors and receptors such as EGF and PDGF, and stimulates production of IL-1β and PGE2. These phenomena, in turn, causes gin- gival overgrowth [3] [29] .
IL-1β, a member of pleiotropic cytokines, is known to be influent on immunological processes, fibroblast’s growth, and inflammatory lesions, and to be capable of stimulating collagenase and prostaglandins such as hya- luronic acid [46] . This cytokine probably causes a decrease in the expression of procollagen and an increase in expression of procollagenase, and so could be known as a stimulator for destroying collagen. Noguchi [47] showed that at the presence of phenytoin, the number of IL-1 β receptors increase, by the way, the IL-1β which has been produced by local immune cells has more paracrine attachment.
These results support the hypothesis that IL-1β plays an important role in regulating ECM in gingival tissue. However, the reports on this issue are inconsistent, e.g. Gonzales et al. have shown that phenytoin raises the in- hibitive effect of IL-1β [3] .
PGE2 is another inflammatory mediator that takes part in regulating the production of collagen and in ECM turn over. Yucel et al. [29] have shown that the PGE2 produced by phenytoin-treated gingival fibroblasts in presence of TNF-α, causes a reduction in IL-1β production. Moreover, adding exogenous PGE2, dose-depen- dently decreases the production of IL-1β. In a similar study, Brunius et al. have shown that the PGE2 that is pro- duced by stimulus of phenytoin and IL-1β is influent on synthesis of glucose amino glycan’s and on inhibition of procollagen α production. They have also reported that adding exogene PGE2 to fibroblast culture results in reduced levels of collagen type I production [29] .
Recent studies have proposed different processes for drug-induced inflammatory trends. For example, one possible explanation is the role of pathogen-sensitive sensors such as Toll-like receptors (TLR) [48] [49] , that are continually present on fibroblasts and are capable of responding to bacterial components. No study has yet reported the probable effects of phenytoin on TLR-related signals. However, based on similar pharmacologic function of phenytoin and Lignocaine, which is a Na+ channel-blocker that inhibits the effects of lipopolysac- charides on mitoionic activator proteins in macrophages, one might propose that phenytoin reduces the fibrob- lasts-related signals [50] . By considering the hyperplasia of phenytoin-treated fibroblasts, it might be concluded that this inhibitive influence is restricted to inflammatory responses and is not related to the drug cytotoxicity. Unlike cyclosporine, phenytoin decreases the production of cytokines and the expression of CD54 as one major marker in immigrating and persistence of inflammatory cells in periodontal diseases [44] . The different functio- nality of cyclosporine and phenytoin could be attributed to the role of phenytoin in reducing the infiltration of inflammatory cells, an effect that is perceived not only in gingival overgrowth but also in under treatment ance- phalomilites [51] . Nevertheless, some studies have reported that phenytoin, solely or in association with IL-1, can raise the production of Interleukin-6 (IL-6) and Interleukin-8 (IL-8) in cultured fibroblasts. This phenome- non can be attributed to the inhibitive impacts of phenytoin in cultures containing serum protein [52] . Modeer et al. [45] have also suggested that phenytoin is responsible for semi-inflammatory changes in gingival overgrowth, and that phenytoin stimulates the secretion of factors such as IL-1β and PGE2. These factors take the latent fi- broblasts to the s stage or synthesis of mitosis cycle, and cause an increase in noncollogenous ECM production. Evidences confirm that in the treatment process, the number of mononuclear cells, especially T lymphocytes, increases in gingival tissue and in not inflammatory overgrown sites, and with the increased expression of CD4, the medial marker between T lymphocytes and fibroblasts, more cytokines can emerge. Eventually, activity and interaction between these cells and the periodontal tissue cells causes the gingival overgrowth [53] .
According to our literature review, this study compared the effect of phenytoin on fibroblasts is investigated through two age groups for the first time. According to epidemiological studies, age is a determinant factor in the occurrence of gingival overgrowth. Doufexi et al. [8] have reported that the gingival overgrowth, especially in anterior regions, is more common in pediatrics and teenagers. Also, Seymour et al. [54] have shown that tee- nagers are more susceptible to gingival hyperplasia. The prevalence of cyclosporine-induced gingival over- growth is 52% in pediatrics in comparison to that of 30% in adults [54] . Moreover, the prevalence of phenytoin- induced gingival overgrowth is reported 67% in pediatrics, while it is 50% in adults [55] . In Majola et al. [56] study, no linear relationship was perceived between the side-effects of phenytoin and length of drug consump- tion, but the lesions were more prevalent in younger patients. Although animal studies have confirmed such re- sults, no specific in vitro study has been conducted on this issue yet, and the reduced synthesis of protein and collagen by fibroblasts in the phenytoin- or cyclosporine-induced gingival overgrowth has not shown to be cor- related with age [57] [58] .
Regarding to our results, the levels of two important inflammatory mediators was increased in pediatric group, and no significant difference was perceived in the cell proliferation. These results suggest that more prevalence of gingival overgrowth in pediatrics in comparison with adults might be attributed to the different immunologi- cal trends in pediatrics, as well as levels and responses of inflammatory cytokines. Unlike this study, the study of Sooriyamorthy did not resulted in a relationship between age and clinical features, a phenomenon which was attributed to the unique phonotype of fibroblasts or to androgynous metabolism influences. Monolayer cultures from gingival fibroblasts can clearly metabolize labeled testosterone into its active metabolite, 5α-dihydrotes- tosteron. Levels of this metabolite increases in presence of phenytoin [59] . Similarly, an increased androgenic metabolism is perceived in parted tissues from Niphedipine- or Cyclosporine-induced overgrown gingiva [60] . On the basis of these results, Sooriyamorthy suggested that the increase in androgenic metabolism is effective in pathogenesis drug-induced gingival overgrowth. Seymour et al. [14] have suggested that active androgenic me- tabolite can target a specific subgroup of gingival fibroblasts and causes an increase in collagen production or a decrease in collagenase enzyme activity. In fact, 5α-dihydrotestostron (DHT) increases in the inflammation and overgrowth process, and stimulates the production of connective tissue [61] . Soory et al. study [61] showed that in presence of IL-1 and phenytoin, the DHT production by fibroblasts doubles. Considering these studies and the present study, phenytoin is probably related to androgenic metabolism in fibroblasts. The increase in production of DHT is one of possible mechanisms in creating overgrowth and subsequent inflammatory trends such as pro- voking glycosaminoglycan and remodeling of connective tissue. Since consumption of phenytoin, Niphedipine and cyclosporine does not always result in gingival overgrowth, recent studies have suggested that genetic fac- tors are possibly influent on the pathogens of these lesions in pediatrics and teenagers [62] . One of genetic risk factors is the gingival fibroblasts response to different dosages and cultures in terms of proliferation and the changes in synthesis of proteins such as collagen [54] . Fibroblasts of different strains demonstrate a natural functional heterogeneity in producing collagenase and other tissue inhibitor of matrix metallo proteinases before and after exposure to drugs that can bring about overgrowth. The variety of activities of cytochrome oxidase P450, the agent of metabolism for phenytoin, cyclosporine and Niphedipine in liver, is genetic factors which are related to gingival overgrowth [8] . Pinkham has suggested that the low levels of Cytochromoxidose p450 and its gradual oxidation causes an incomplete and sudden functionality of this enzyme in digestion and detoxification of phenytoin and so the clinical effects of this drug and the probability of toxicity increases as the levels of P450 decrease [63] . Trackman et al. have also proposed that the reduced metabolism and liver’s dispel of phenytoin could be another cause of gingival overgrowth. This hypothesis, however, is not confirmed yet [27] .
Dental plaque is another factor in phenytoin- and cyclosporine-induced gingival overgrowth especially in younger patients. Studies have suggested that the prevalence and intensity of gingival overgrowth is positively correlated with dental plaque [8] . Doufexi et al. have reported that incubation of monocytes and macrophages could increase the Platelet-derived growth factor (PDGF) and stimulates gingiva growth [8] . The presence of in- flammatory cells and their produced mediators in drug-induced gingival overgrowth condition corroborates the relation between overgrowth and preexisting inflammation. Since the majority of studies are cross-sectional, it is not yet clear whether the improper oral hygiene is the initial reason of gingival overgrowth or not. In a 2-year study on pediatrics, Dalhoof et al. [64] showed that proper oral hygiene and educational programs can not solely hinder the phenytoin-induced overgrowth. Nevertheless, oral hygiene could inhibit the subsequent changes in inflammatory condition and so hamper further overgrowth.
Bonding of plasma proteins is another probable cause of difference in overgrowth of gingiva in pediatrics and adults. There is neither linear relationship between the duration nor intensity of treatment and the levels of plasma proteins. Reduction in the levels of these proteins and their bonding to phenytoin causes the drug to dis- perse in the tissues, especially in the tissues with high affinity to phenytoin, e.g. gingival fibroblast tissues [53] .
The discussed reasons for different response of gingival fibroblasts to phenytoin in pediatrics and adults are briefly demonstrated in Figure 1.
The present study is the only research that has compared the effects of phenytoin on gingival fibroblasts in children and adults, however, further studies are necessary to confirm the discussed results. Unlike other studies,

Figure 1. The discussed reasons for different response of gingival fibroblasts to phenytoin in pediatrics and adults.
this study was designed to investigate different aspects of drug influence. This study was conducted without cell lines genetic manipulations or retentive materials, features that are potential advantages of this study.
The different results of variant studies could be attributed to different sources of fibroblasts, the location of biopsies, age of patients or small population of samples. The natural heterogeneity of fibroblasts in response to phenytoin might be another reason for such differences. In order to prevent such issues in this study, those cul- tures, among cell lines extracted from different patients, were chosen that had shown rather similar responses to phenytoin, and the coefficient of correlation among different wells was calculated at the end [3] . Groups were divided into two responsive and nonresponsive groups on the basis of the perceived growth of gingiva. Genetic differences result in larger dimensions of fibroblasts and greater capacity of secretion of ECM proteins and so- luble factors in members of the responder group. Gonzalez et al. have not reported any difference among the expression of fibroblast-related markers in healthy, responder and non-responder groups [3] [25] . So, the gin- gival fibroblasts in 3 groups are capable of responding to LPS intra oral pathogens such as P. gingivalis and F. nucleatum. Fibroblasts can also disturb the toll-like 2, 4 receptors, which play a role in immune processes. As a result, any disturbance in ECM metabolisms during the treatment period can be occurred [27] .
5. Conclusion
No significant difference was perceived between proliferations of these two groups. The significant increase in production of IL-1β and PGE
Acknowledgements
There is no conflict of interests. Authors would like to thank research council of dental school, Shahid Beheshti University of Medical sciences for its financial support of this study.
References
- Maitu, E., Sato, M. and Yamaki, K. (2004) Effect of Tranilast on Martin Metalloproteinase-1 Secretion from Human Gingival Fibroblast in Vitro. Journal of Periodontology, 75, 1054-1060. http://dx.doi.org/10.1902/jop.2004.75.8.1054
- Brunet, L., Miranda, J., Fere, M., Berini, L. and Mendieta, C. (1996) Gingival Enlargement Induced by Drugs. Drug Safety, 15, 219-231. http://dx.doi.org/10.2165/00002018-199615030-00007
- Gronzalez, O. and Gonzalez, J.M. (2009) Morphological and Phenotypic Difference in Fibroblasts Obtained from Gin- gival Overgrowth Secondary to Phenytoin: Pilot Study. Revista Odontologica Mexicana, 13, 17-23.
- Perucca, E. (2005) An Introduction to Antiepileptic Drugs. Epilepsia, 46, 31-37. http://dx.doi.org/10.1111/j.1528-1167.2005.463007.x
- Lucches, J., Cortelli, S.H. and Rodrigues, J. (2008) Server Phenytoin-Induced Gingival Enlargement Associated with Periodontitis. General Dentistry, 56, 199-203.
- Reynolds, E.H. (1975) Chronic Antiepileptic Toxicity, a Review. Epilepsia, 16, 319-352. http://dx.doi.org/10.1111/j.1528-1157.1975.tb06062.x
- Bhatia, A. and Prakash, S. (2004) Topical Phenytoin for Wound Healing. Dermatology Online Journal, 10, 5.
- Doufexi, A., Mina, M. and Loannidou, E. (2005) Gingival Overgrowth in Children: Epidemiology, Pathogenesis and Complications, a Literature Review. Journal of Periodontology, 76, 3-10. http://dx.doi.org/10.1902/jop.2005.76.1.3
- Morisaki, K.K., Loyola-Rodriguez, J.P., Nagata, T., and Ishida, H. (1993) Nifediphine-Induced Gingival Overgrowth in the Presence or Absence of Gingival Inflammation in Rats. Journal of Periodontal Research, 28, 396-403.
- Ishikawa, S., Nagata, T., Morisaki, I., Oka, T. and Ishida, H. (1996) Pathogenesis of Drug Induced Gingival Over- growth, A Review of Studies in the Rat Model. Journal of Periodontology, 67, 463-471. http://dx.doi.org/10.1902/jop.1996.67.5.463
- Seymour, R.A. (1992) Heasann PA: Drugs and the Periodontium. Journal of Clinical Periodontology, 19, 1-11. http://dx.doi.org/10.1111/j.1600-051X.1992.tb01140.x
- Hassel, T.M. and Hefti, A.F. (1991) Drug Induced Gingival Overgrowth: Old Problem, New Problem. Critical Reviews in Oral Biology Medicine, 2, 103-137.
- Barclay, S., Thomason, T.M., Idle, J.R. and Seymour, R.A. (1992) The Incidence and Severity of Nifediphine Induced Gingival Overgrowth. Journal of Clinical Periodontology, 19, 311-314. http://dx.doi.org/10.1111/j.1600-051X.1992.tb00650.x
-
- Easley, J. (1967) Methods of Determining Alveolar Osseous Form. Journal of Periodontology, 38, 112.
- Friedman, N. (1955) Periodontal Osseous Surgery, Osteoplasty and Osteoectomy. Journal of Periodontology, 26, 257.
- Goldman, H.M. and Cohen, D.W. (1958) The Infrabony Pocket: Classification and Treatment. Journal of Periodontology, 29, 272. http://dx.doi.org/10.1902/jop.1958.29.4.272
- Ochsenbein, C. (1986) A Primer for Osseous Surgery. The International Journal of Periodontics and Restorative Dentistry, 6, 9.
- Carranza, F.A., Take, H. and Newman, M. (2006) Clinical Periodontology. Cha
- Guncu, G.N., Caglayan, F., Dincel, A., Bozkurt, A., Sayg, S. and Karabulut, E. (2006) Plasma and Gingival Curricular Fluid Phenytoin Concentrations as Risk Factors for Gingival Overgrowth. Journal of Periodontology, 77, 2005-2010. http://dx.doi.org/10.1902/jop.2006.060103
- Seymour, R. (2006) Effects of Medications on the Periodontal Tissues in Health and Disease. Journal of Periodontology, 40, 120-129.
- Yamada, H., Nishimura, F., Naruishi, K., Chou, H. and Takashiba, S.H. (2000) Phenytoin and Cyclosporine a Suppress the Expression of MMP-1, TTMP-1 and Cathepsin, but Not Cathepsin B in Cultured Gingival Fibroblasts. Journal of Periodontology, 71, 955-960. http://dx.doi.org/10.1902/jop.2000.71.6.955
- Kataoka, M., Kido, J., Shinohara, Y. and Nagata, T. (2005) Drug-Induced Gingival Overgrowth―A Review. Biological and Pharmaceutical Bulletin, 28, 1817-1821. http://dx.doi.org/10.1248/bpb.28.1817
- Halmoon, W.W. and Rossmann, J.A. (1999) The Role of Drugs in the Pathogenesis of Gingival Overgrowth, a Collective Review of Current Concepts. Periodontology 2000, 21, 176-196. http://dx.doi.org/10.1111/j.1600-0757.1999.tb00175.x
- Everts, V., Van der zee, E., Creemers, L. and Beertsen, W. (1996) Phagocytosis and Intracellular Digestion of Collagen Its Role in Turn over and Remodeling. The Histochemical Journal, 28, 229-245. http://dx.doi.org/10.1007/BF02409011
- O’valle, F., Mesa, F.L., Gomez-Murales, M., et al. (1994) Immunhistochemical Study of 30 Cases of Cyclosporine A-Induced Gingival Overgrowth. Journal of Periodontology, 65, 742-730. http://dx.doi.org/10.1902/jop.1994.65.7.724
- Trackman, P.C. and Kantarci, A. (2004) Connective Tissue Metabolism and Gingival Overgrowth. Critical Reviews in Oral Biology Medicine, 15, 165-175. http://dx.doi.org/10.1177/154411130401500305
- Okahashi, N., Kato, T., Ohno, T., Inaba, H., Kawai, S. and Amano, A. (2006) Effect of Phenytoin on Collagen Accumulation by Human Gingival Fibroblasts Exposed to TNF-α in Vitro. Oral Diseases, 12, 156-162. http://dx.doi.org/10.1111/j.1601-0825.2005.01175.x
- Yucel-Linberg, T., Brunius, G., Shinoda, K. and Modeer, T. (1996) Effect of Phenytoin on Interlukin-1β Production in Human Gingival Fibroblasts Challenged to Tumor Necrosis Factor α in Vitro. European Journal of Oral Sciences, 104, 27-33. http://dx.doi.org/10.1111/j.1600-0722.1996.tb00042.x
- Modeer, T., Anduren, I., Bengston, A. and Anderson, G. (1996) Interleukin-1β and Phenytoin Reduce α1 (1) Procollagen mRNA Expression in Human Gingival Fibroblasts. Journal of Periodontal Research, 31, 563-568. http://dx.doi.org/10.1111/j.1600-0765.1996.tb00521.x
- Yucel-Lindberg, T., Leiner, U.H. and Modeer, T. (1995) Effects and Interactions of Tumour Necrosis Factor α and Bradykinin on Interleukin-1 Production in Gingival Fibroblasts. Journal of Periodontal Research, 30, 186-191. http://dx.doi.org/10.1111/j.1600-0765.1995.tb01272.x
- Newman, M.G., Takei, H.H. and Carranza, F.A. (2002) Clinical Periodontology. Chap. 25. 9th Edition, W.B. Saunders Co., Philadelphia, 406-408.
- Lindhe, J., Liljenberg, B. and Listgarten, M. (1980) Some Microbiological and Histological Features of Periodontal Disease in Man. Journal of Periodontology, 51, 264-269. http://dx.doi.org/10.1902/jop.1980.51.5.264
- Mattson, L. (1978) Development of Gingivitis in Preschool Children and Young Adults: A Comparative Experimental Study. Journal of Clinical Periodontology, 5, 24-28. http://dx.doi.org/10.1111/j.1600-051X.1978.tb01903.x
- Gillett, R., Cruckley, A. and Johnson, N.W. (1986) The Nature of the Inflammatory Infiltrates in Childhood Gingivitis, Juvenile Periodontitis and Adult Periodontitis: Immunocytochemical Studies Using a Monoclonal Antibody to HLA Dr. Journal of Clinical Periodontology, 13, 281-286. http://dx.doi.org/10.1111/j.1600-051X.1986.tb02223.x
- Gillette, R., Longhurst, P. and Johnson, N.W. (1980) Electron Microscope Quantification of Inflammatory Infiltrates in Childhood Gingivitis. Journal of Periodontal Research, 15, 255-258. http://dx.doi.org/10.1111/j.1600-0765.1980.tb00282.x
- Longhurst, P., Johnson, N.W. and Hopps, R.M. (1977) Differences in Lymphocyte and Plasma Cell Densities in Inflamed Gingival from Adults and Young Children. Journal of Periodontology, 48, 705-709. http://dx.doi.org/10.1902/jop.1977.48.11.705
- Seymour, G.J., Grouch, M.S. and Powell, R.N. (1982) The Identification of Lymphoid Cell Subpopulations in Section of Human Lymphoid Tissue and Gingivitis in Children Use in Monoclonal Antibodies. Journal of Periodontal Research, 17, 247-252. http://dx.doi.org/10.1111/j.1600-0765.1982.tb01151.x
-
- Al-Ubady, S.H., Al-Janabi, N. and Suhaila, A. (1981) Effect of Phenytoin on Mitotic Activity of Gingival Tissue and Cultured Fibroblast. Journal of Periodontology, 52, 747-749. http://dx.doi.org/10.1902/jop.1981.52.12.747
- Pour Abbas, R., Niknafs, B. and Shirmohamadi, A. (2006) The Effect of PHT on PDL and Gingival Fibroblasts Proliferation in Cell Culture. Medical Journal of Tabriz University of Medical Sciences & Health Services, 28, 45-48.
- Modeer, T., Karsten, J., Weintraub, A., Gidlund, M. and Sundqvist, K.G. (1989) Phenytoin Induces Interlukin-1 Production in Vitro. Life Sciences, 44, 35-40. http://dx.doi.org/10.1016/0024-3205(89)90215-4
- Kato, T., Okahashi, N., Kaeai, S., Kato, T., Inaba, H., Morisaki, I. and Amano, A. (2005) Impaired Degradation of Matrix Collagen in Human Gingival Fibroblast by the Antiepileptic Drug Phenytoin. Journal of Periodontology, 76, 941- 950. http://dx.doi.org/10.1902/jop.2005.76.6.941
- Brunius, G., Modeer, T., Inuma, M. and Lerner, U.H. (1992) Phenytoin Potentiates Interlukin-1 Induced Prostaglandin Biosynthesis in Human Gingival Fibroblast. British Journal of Pharmacology, 106, 574-578. http://dx.doi.org/10.1111/j.1476-5381.1992.tb14377.x
- Modeer, T., Brunius, G. and Lerner, H. (1992) Enhanced Prostaglandin Biosynthesis in Human Gingival Fibroblasts Isolated from Patients Treated with Phenytoin. Journal of Oral Pathology Medicine, 21, 251-255. http://dx.doi.org/10.1111/j.1600-0714.1992.tb01005.x
- Bartold, P.M. (1988) The Effect of Interleukin-1 β on Hyaluronic Acid Synthesized by Adult Human Gingival Fibroblasts in Vitro. Journal of Periodontal Research, 23, 139-147. http://dx.doi.org/10.1111/j.1600-0765.1988.tb01347.x
- Noguchi, K., Tominaga, Y., Matsushita, K., Izumi, Y., et al. (2001) Upregulation of Matrix Metalloproteinase-1 Production by Prostaglandin F2α in Human Gingival Fibroblasts. Journal of Periodontal Research, 36, 334-339. http://dx.doi.org/10.1034/j.1600-0765.2001.360510.x
- Mahanonda, R., Sa-Ard-Iam, N., Montreekachon, P., et al. (2007) IL-8 and IDO Expression by Human Gingival Fibroblasts via TLRs. The Journal of Immunology, 178, 1151-1157. http://dx.doi.org/10.4049/jimmunol.178.2.1151
- Yu, M.J., Yang, P.S. and Ge, S.H. (2008) Biological Effects on Phenytoin on Cultures Human Periodontal Ligament Fibroblasts in Vitro. West China Journal of Stomatology, 26, 215-218.
-
- Black, J.A., Liu, S., Itanis, S.C. and Saab, C.Y. (2006) Long-Term Protection of Central Axons with Phenytoin in Monophasic and Chronic-Relapsing EAE. Brain, 129, 3196-3208. http://dx.doi.org/10.1093/brain/awl216
- Domeij, H., Mdeer, T., Anduren, I., Mustafa, M. and Brunius, G. (2000) Effect of Phenytoin on Production on Interlukin-6 and Interleukin
- Dongari, A.I., Warren, D.W. and Berton, M.T. (1997) CD40 Expression by Gingival Fibroblasts: Correlation of Phenotype with Function. International Immunology, 9, 1233-1241. http://dx.doi.org/10.1093/intimm/9.9.1233
- Seymour, R.A., Ellis, S.S. and Thomason, J.M. (2000) Risk Factors for Drug Induced Gingival Overgrowth. Journal of Clinical Periodontology, 27, 217-223. http://dx.doi.org/10.1034/j.1600-051x.2000.027004217.x
- Greenwood, R., Tennison, M.B. and Maguire, J.H. (1986) Phenytoin-Induced Gingival Overgrowth and Antiepilep- tic Co-Administration. Epilepsia, 27, 540.
- Majola, M., Mcfadyen, M., Connolly, C., Nair, Y., Govender, M. and Laher, M. (2000) Factors Influencing Phenytoin-Induced Gingival Enlargement. Journal of Clinical Periodontology, 27, 506-512. http://dx.doi.org/10.1034/j.1600-051x.2000.027007506.x
- Kitamura, K., Morisaxi, I., Adachi, C., et al. (1990) Gingival Overgrowth Induced by Cyclosporine A in Rats. Archives of Oral Biology, 35, 483-486. http://dx.doi.org/10.1016/0003-9969(90)90213-T
- Johnson, B.D, Natayanon, A. and Pieters, H. (1990) Effects of Cell Donor Age on Synthetic Properties of Fibroblasts Obtained from Phenytoin-Induced Gingival Hyperplasia. Journal of Periodontal Research, 25, 74-80. http://dx.doi.org/10.1111/j.1600-0765.1990.tb00895.x
- Sooriyamorthy, M., Horvey, W. and Gower, D.B. (1968) The Use of Human Gingival Fibroblasts in Cultured for Studying the Effect of Phenytoin on Testosterone Metabolic. Archives of Oral Biology, 33, 353-359. http://dx.doi.org/10.1016/0003-9969(88)90069-6
- Sooriyamorhy, M., Gower, D.B. and Eley, B.M. (1990) Androgen Metabolism in Gingival Hyperplasia Induced by Nifedipine and Cyclosporine. Journal of Periodontal Research, 25, 25-30. http://dx.doi.org/10.1111/j.1600-0765.1990.tb01204.x
- Soory, M. and Kasasa, S.C. (1997) The Effects of Epidermal Growth Factor, Interleukin-1, and Phenytoin, Alone and in Combination, on C19 Steroid Conversions in Fibroblasts. Journal of Periodontology, 68, 819-826. http://dx.doi.org/10.1902/jop.1997.68.9.819
-
- Pinkham, J.R. and Cassmassimo, P.S. (2005) Pediatric Dentistry Infancy through Adolescence. 4th Edition, W.B. Saunders Co., Philadelphia, 394-413.
- Dahllof, G. and Modeer, T. (1986) The Effect of a Plaque Control Program on the Development of Phenytoin-Induced Gingival Overgrowth. A 2-Year Longitudinal Study. Journal of Clinical Periodontology, 13, 845-849. http://dx.doi.org/10.1111/j.1600-051X.1986.tb02241.x
NOTES
*Corresponding author.