Open Journal of Nursing
Vol.3 No.4(2013), Article ID:35694,9 pages DOI:10.4236/ojn.2013.34049
Developing an educational framework for the teaching of simulation within nurse education
![]()
School of Nursing and Midwifery, Keele University, Stoke-on-Trent, UK
Email: m.humphreys@keele.ac.uk
Copyright © 2013 Melanie Humphreys. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 15 May 2013; revised 15 June 2013; accepted 29 July 2013
Keywords: Nursing; Simulation; Education; Pedagogy; Curriculum
ABSTRACT
The use of simulations as a teaching and learning tool within health care has increasing importance; simulations are seen as the major teaching method for practicing and assessing developing skills, knowledge, attitudes and meaningful decision-making within the field of nursing. Certainly the utilisations of simulations feature widely within many aspects of health care; a greater understanding of the key conceptual notions will serve to benefit all of those engaged within their application. This literature review has enabled the construction of a conceptual model for the teaching of simulation and can serve to promote the continued positive development of simulations within education. Through a consistent and insightful approach to teaching, dynamic learning will be assured within this very important aspect of engaging the nursing student within the learning process.
1. INTRODUCTION
Student anxiety and employer dissatisfaction with the level of practical competence in newly qualified nurses have prompted numerous reports [1-3]. Students cite anxiety about feeling “clinically incompetent” [4,5], and perceive themselves inadequately prepared for clinical practice [6]. Employers report a need to provide substantial support for new nurses in making the transition into the workforce [7]. These issues are not isolated to nursing, but also reported in the literature relating to medical education too [8,9]. Whilst there is clear recognition of issues associated with skill acquisition, there is limited research about what might constitute a solution. To date, the major emphasis in the literature has been on assessment, simulation, and single case reports of innovative teaching strategies [5]. There is growing interest in the use of simulation techniques to support clinical learning, in both nursing and medical education [1,2,10]; more recently with the publication of the draft National Simulation Strategy [11].
Health care educators are facing great challenges in keeping up with the demands required to prepare graduates for 21st century health care practice. Health care environments are complex, and they require high-tech, problem solving, and decision making skills, as well as a strong knowledge background. With the explosion of technologies within education confronting these changes and challenges demands the continual exploration of new and innovative teaching learning methods that strive for the achievement of high quality education that is equitable, cost effective and sustainable.
The current push for IPE and the development of core competencies has placed an increasing emphasis on communication and [12]. Simulation can also be used to promote and support excellence through continued development. Established professionals and teams can use simulation-based techniques to keep up to date and refine their practice. Technology-enhanced learning allows the workforce to engage in continued development both alone and as members of teams as they strive to become excellent. This ability of simulation to enhance performance through “mission” rehearsal is widely used in other high-reliability organisations such as aviation and the military but has been less widely adopted in healthcare [13].
Within the Framework for Technology Enhanced Learning [11], it is recognised that simulations allow complex ideas, techniques or concepts to be explored. Indeed, simulations have the potential to test new ideas and explore how professionals and patients interact with each other [14].
There is an inherent assumption in the literature that clinical laboratories are necessary within nurse education, but there has been limited discussion of what constitutes the ideal pedagogical approach that can facilitate effecttive learning within them. This paper, through a review of the literature, seeks to identify how simulation practises are underpinned and driven forward within the nursing curriculum, in order to identify pedagogies that promote teaching and learning for simulation.
2. LITERATURE REVIEW
2.1. Defining Simulation
Within health care education there are two types of simulation tool; computer based simulation tools within which the student will work through a computer programme answering questions and making clinical decisions, and advanced human patient simulators (AHPS) which can be described as a human mannequin animated with a variety of electromechanical or pneumatic devices that produce respiratory movement, palpable pulses, heart and lung sounds and realistic airway anatomy [14].
A simulation can be described as an imitation of some facet of life, usually in a simplified form. It aims to put learners in a position where they can experience some aspect of real life by becoming involved in activities that are closely related to it [15]. Within a recent report conducted on behalf of the West Midlands Strategic Health Authority [16] the following definition was posed by an expert panel:
Simulation is defined as:
An approach to facilitating learning through which participants develop and demonstrate skills and behaveiours in a controlled environment which affords opportunities for exploration and rehearsal. It utilises engineered situations designed to be sufficiently authentic to promote the acquisition and development of skills, behaviours and understanding required for effective working.
If nurse education is to benefit from the integration of simulation it would appear fundamental to address the underlying pedagogical theory that serves to inform this particular learning modality.
2.2. Philosophical Underpinning
There are many theoretical frameworks that have been applied to simulation work. For instance, Waldner and Olson [17] present an interesting literature review where they make links to existing theoretical models and their application to simulation experiences. They offer a workable model for utilising both Benner’s [18] model of skill acquisition and Kolb’s [19] experiential theory to guide academics in their decision making within nurse education. Benner [18] distinguishes among five levels of competency; novice, advanced beginner, competence, proficiency, expert. Differentiation among the levels is determined by the nurses’ focus of attention, involvement in the situation, and perception of responsibility or accountability. Waldner and Olson [17] claim that the transformation from novice to expert nurse occurs when experience is incorporated into existing knowledge patterns through a process of active reflection and concepttualisation of experience.
Sewchuck [20] details how experiential learning theory takes into account four different learning styles. Accommodating learners learn from experience and internalise learning through active experimentation. Diverging learners also learn best from experience, but they internalise the knowledge by reflecting on the experience. Converging learners learn from abstract ideas and internalise the abstract ideas by experimentation. Assimilating learners learn from abstract ideas and internalise those ideas through reflection. Interestingly, Kolb [19] categorised nursing as a profession that attracts diverging learners, this perhaps goes some way in explaining the increased preference that learners have for this method of education [21]. Waldner and Olson [17] conclude that in applying simulation within nurse education, one could use Benner’s [18] model to determine what is, should, or could be taught using a particular simulation. Kolb’s [19] theory of experiential learning could help determine how simulation can accomplish learning goals. Waldner and Olson [17] offer the combination of these models to provide a theoretical scaffold for building the progression of simulation experiences in the development of students’ nursing knowledge; claiming that the utilisation of such models is important for ensuring that students’ experiences reflect the appropriate sequence of developing knowledge.
Whilst many skills have their basis in theory, the main emphasis within simulations is the acquisition of practical techniques, so it is important to teach in a way that helps learners to cope with real-life situations. Whilst simulations imitate they do not duplicate reality, thus the use of a simulation has the potential to create a sense of effectiveness, enabling learners to face consequences, encourage an increase in knowledge, empathy, critical thinking and decision-making in a risk-free setting [14].
Parker & Myrick [21] explore the value of two educaional methodologies within their review, they believe that both constructivism and behaviourism can provide a basis for the incorporation of simulation within the nursing curriculum. They consider that behaviourist-based simulation is more effective in the development of psychomotor skills and rote learning of factual knowledge. Conversely, constructivist-based simulation is deemed more valuable in developing clinical-judgement skills, problem-solving, collaboration, and group process. Whilst they [21] discuss educational underpinnings and state that the behaviourist approach centres on the concept that laws govern human behaviour; they do not acknowledge individual differences to learning processes, in the way in which Sewchuck [20] does.
Individuals learn through the responses of others to their behaviour that lead to satisfying results, and the repetition of these satisfying results causes learning. In contrast the constructivist approach to teaching and learning is based on the concept that learners create their own meaning through interaction with the environment [22], which is especially true when integrating simulation. For the constructivist, learning is constructed knowledge, and knowledge is viewed as a symbolic construct in the learner’s mind [23]. Compared to behaviourism, constructivist pedagogy argues that knowledge transmissions not inertly passed from teacher to learner, but rather, is created by individual learners, or in some cases groups of learners, by processing experiences and interactions with their environment [21]. It could be claimed that the constructivist methodology would have greater appeal for the advancing nursing student as it attempts to draw out the clinical judgement skills and meaningful decision making—that appears so attractive to nurse educators. A behaviourist approach has much appeal as a simple skills acquisition model, and is currently utilised quite extensively within nursing [24], this methodology is based on repetition and reinforcement which is useful for skills teaching, but has limits in its application to simulation encounters.
2.3. Simulation Process
According to the social constructivist approach, educators need to adapt to the role of facilitators and not traditional teachers [25]. The emphasis thus turns away from the instructor and the content, and towards the learner [26]. This change in traditional role, in facilitating simulation, implies that as a facilitator the educator needs to display a different set of skills [27]. This in itself can be a challenge to the educator new to simulation teaching [28,29]. Today’s learner, through their familiarity and comfort with web-based interaction and virtual environments, has developed a preference for immersion as a learning methodology [29] and simulation embraces this philosophy. However, the responsibility for facilitating the environment and therefore optimising learning remains with the instructor.
Simulation is a powerful learning tool, and the facilitator would be expected to adapt the learning experience “in mid-air” by using his or her own initiative in order to steer the learning experience to where the learners want to create value. This idea of social constructivism, strongly influenced by Vygotsky’s [30] work, suggests that knowledge is first constructed in a social context and is then appropriated by individuals. According to social constructivists, the process of sharing individual perspectives—called collaborative elaboration [31]—results in learners constructing understanding together that wouldn’t be possible alone [32]. Indeed, most social constructivist models, such as that proposed by Duffy and Jonassen [33], also stress the need for collaboration among learners, in direct contradiction to traditional competitive teaching and learning approaches. One Vygotskian notion that has significant implications for peer collaboration is that of the zone of proximal development; defined as the distance between the actual developmental level, as determined by independent problem-solving, and the level of potential development, as determined through problem-solving under adult guidance or in collaboration with more capable peers. Through a process of “scaffolding” a learner can be extended beyond their current limitations of skills to one of achievement [30].
It is evident from the literature reviewed, that many researchers hold firm beliefs regarding what constitutes an effective learning environment within simulation. From the studies three themes emerged of theoretical importance when managing simulations as an educational tool, which firstly, when brought together have the potential to enable the educator to facilitate such a scaffold [30], and secondly, warrant further exploration and development within future research. The three themes identified are;
• Preparedness
• Activation
• Reflection The themes are quite broad, but reflect the current issues addressed in the literature, and highlight where future research energies can be directed (see Table 1 for summary of the initial thematic analysis). In addition, the themes identified suggest commonalities between organisations in the way in which simulation use has evolved. Not surprisingly, although the interpretation of use varies, the activities identified in the evidence base illustrated that academics are utilising these broad areas to support student nurses in their personal and professional development.
2.4. Preparedness
The theme “preparedness” refers to the activities that are undertaken to ensure that the simulation session has the potential to run effectively, and fundamentally, the preliminary events. This would include considerations to the environment, resources, underpinning curriculum and learning outcomes to be achieved. The way by which we view a situation is influenced greatly by past experiences; structured educational techniques that provide experience through simulation, seek to help the learner gain insight into the management of critical events [21]. The facilitator needs to assess the knowledge, understanding and experience of an individual learner in order to build on their current abilities in a constructive way; an experienced facilitator will utilise these to engage the learner
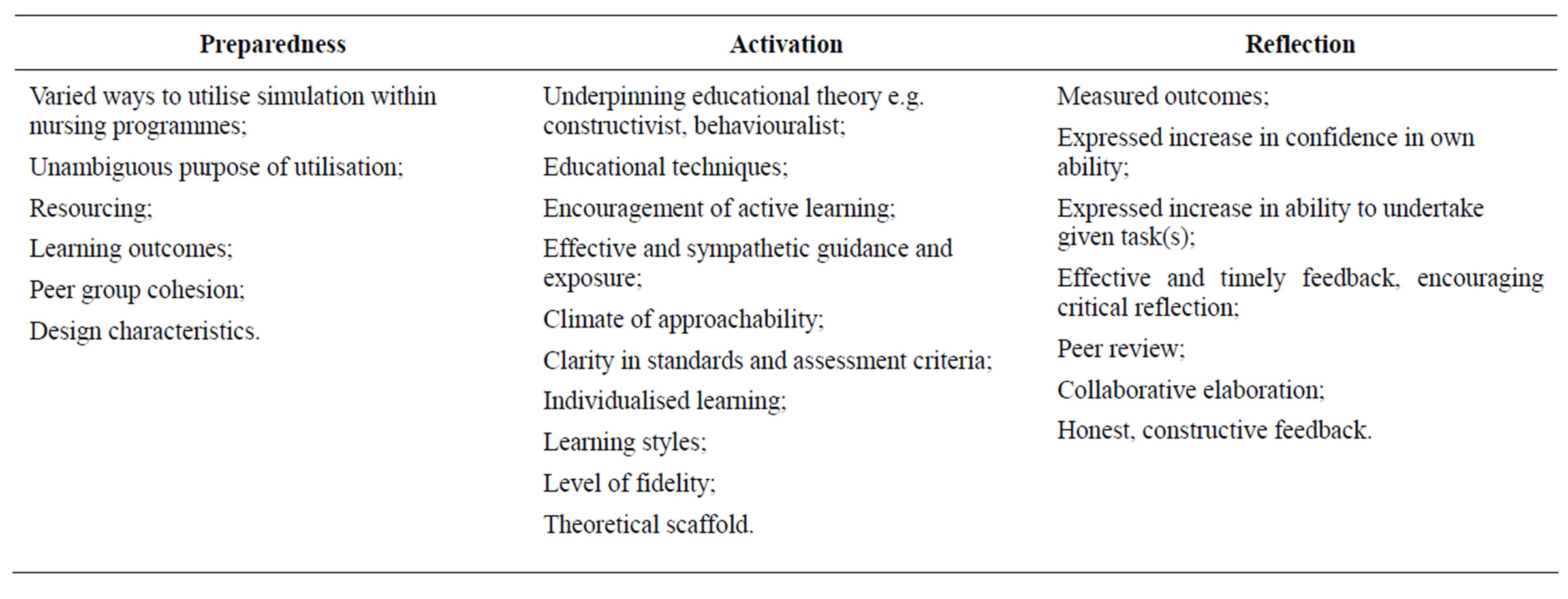
Table 1. Findings from simulation literature reviewed: dimensions of engagement.
within the learning process [34].
Fink [35] discusses the creation of significant learning experiences. Based in educational research, he has compiled six major dimensions to formulate significant learning goals. In considering these learning goals, areas can be identified that demonstrate how simulation complements nursing education to meet programme goals and outcomes. Whilst many critical interventional techniques have their basis in theory, policy and guidelines, within simulation the main emphasis appears to be upon the practical application of knowledge and techniques; it is expressed within the literature that one of the most important aspects is to teach in a way that helps learners to cope with real-life situations [36]. Within the theme of preparedness, it would appear that orientation of the students is critical to the success of the simulation experience [37]. Thoughtfully crafted, the use of simulation has the potential to create a sense of effectiveness, enabling learners to face consequences, encourage an increase in knowledge, empathy, critical thinking, decision-making and finally concepts and skills together [38]. Indeed peer group cohesion has been reported in several studies as having great importance, the need for the group to feel safe and risk free is essential for successful learning within simulation [24,38,39].
Scherer et al. [40] undertook a comparative study to determine the most effective method on Nurse Practitioner students’ knowledge and confidence, comparing simulation with a clinical seminar approach and their distinctive features in terms of educational methodology. The participants within this study reported that working within an educational environment where simulation was utilised particularly challenging, this could be explained by the fact that the University did not routinely utilise this within their curriculum—therefore, students had no previous engagement and lead into this approach to learning. This would further support the notion that the “ease-in” is of great importance, thus preparedness has great significance.
Past experiences and confidence will have an effect on willingness to participate [41], specifically Jeffries details these variables as being the programme of study, the level and age of the student. The student may be cautious, reticent and reluctant to risk making errors—these behaviour types will have an effect on the dynamics within the encounter—often described as the “presage variables” [42]. It will be a challenge for the educator to motivate and enthuse the learners who may be displaying these behaviour types before the session commences [43]. It can be suggested that the success of simulation-based education is upon its interactive nature.
It can be concluded that through the literature much importance is placed within the preparedness phase, this does not solely lie with the educators ability to assess prior knowledge, perspectives and experiences and build upon these in a constructive way; but also the ability to develop peer group cohesion before the engagement of activities commences, this needs to be supported through the planning and subsequent execution of realistic goals.
2.5. Activation
The theme “activation” refers to the activities that are undertaken during the simulation learning encounter to ensure that learning opportunities are maximised, this would include the educational theory utilised to underpin the session, degree of active learning, appeal to learning styles and fidelity. Activation is encapsulated within the notion of “engagement”; and essentially is the phase when the activities to achieve the learning outcomes are undertaken. The concept of simulation is about the development and reinforcement of key learned skills, without doing the patient any harm [21]. The use of simulation enables the practitioner to develop confidence and competence when using their skills [44].
The activities that are undertaken within the process of engagement can be described as the “process variables” [42]. During this phase of teaching and engagement it is the behaviour of both the teacher and learner that will shape the process of the dynamic environment. Indeed, the relationship between teacher behaviour, student behaviour and student achievement have been described as existing in a reciprocal way and therefore can be represented as cyclical or circular [45]. This is because teacher behaviour affects student behaviour, which in turn affects student achievement. Clearly simulation-based education requires educators to take a proactive approach to clinical exposure by designating an optimal learning environment to serve the educational objectives. In contrast to learning from actual clinical encounters which are constrained by chance, availability, and conflict with clinical operations, simulation-based education provides the opportunity to have full control over the clinical curriculum in terms of content, degree of difficulty, sequence, clinical setting and the variety of clinical scenarios [46].
Simulation is a learner-centred educational experience, and according to some authors, benefits from a constructivist underpinning [21]. Models and frameworks have been proposed and utilised to help conceptualise the role of simulation in nursing education. One such model describes a simulation protocol based on the work of Benner [18], and utilises a cue-based system with escalating prompts to move students through recognition to assessment to intervention to problem resolution. Unlike the model proposed by Waldner and Olson [17] which focuses specifically upon skills acquisition; Larew’s model recommends that the instructor highlights one problem at a time, allowing the scenarios to be student directed with time for processing in the pacing of the scenario, and wholly encompassing of the patient situation. What is interesting is that increasingly frameworks are being presented based on the seminal work of Benner [18] and this would seem to be a logical proposition given that Benner’s work aligns well with the theoretical and conceptual foundations of nursing education.
The role of the teacher in guiding and coaching the learning through the simulation event whilst ensuring fidelity is a recurring theme [17,24,21]. Fritz et al., [47] emphasises the need to consider that beyond technological fidelity, there are actually three levels of fidelity: environmental, equipment and psychological.
• Environmental fidelity: The realism of the environment in which the simulation takes place;
• Equipment fidelity: Hardware and/or software realism of the simulator;
• Psychological fidelity: Reflects the degree to which the trainee perceives the simulation to be a believable representation of the reality it is duplicating.
2.6. Scenarios within Simulations
Students use a synthesis of past experiences to pool best practices into actual practice [48], one of the important hallmarks of simulation is that the learners are not required to act out any kind of script; they are expected to behave and react in any way they feel is appropriate. In other words, the activation phase involves the learners being themselves, and dealing with situations using their normal, everyday behaviour [29,36]. Scenarios are a tool that enables the students to work through a clinical event; they can be seen as the “lead-in” on which the simulation encounter is based. Whatever the scenario of the simulation may be, the learners are expected to be themselves and to deal with the situations presented. Therefore, it is considered essential within the literature and in order that maximum learning takes place that the scenario created is as near as possible to the real-life situation that the learner will encounter, so that the established behaviours and procedures can be transferred easily to the new setting [10,49].
Within this developing model, the activation phase should be well structured. In terms of the teachers’ role in facilitating the learning process, the following four essential elements appear to emerge, emanating from the seminal work of Janes & Cooper [50];
• Complexity
• Interaction
• Control
• Reality The maintenance of motivation becomes increasingly important as the complexity of the scenario increases [17]. The teacher’s personal style, commitment and enhusiasm are all major factors that motivate learners and maintain the momentum once the practice is under way. Mazlow’s [51] classical theory of motivation asserts that the principle of voluntarism is a key feature of successful adult learning experiences. Furthermore, teachers need to exert control over the learners during the simulation. The degree of control necessary will vary with the type of simulation. It may be quite low when learners have gained confidence and expertise and are performing well—for example after many practices. Higher levels of control are necessary in more structured or guided scenarios, which aim to encourage specific behaviour, which would be appropriate in the early stages of practice. These notions link well with the theory of Novice to Expert [18].
It can be concluded that through the literature much importance is placed within the activation phase. The identification of a suitable theory to guide this dynamic interface is of fundamental importance. Here the use of constructivist theory [30], in conjunction with a guiding framework such as that developed by Benner [18] leading from novice to expert has been explored. Other important aspects include effective and sympathetic guidance by the educator and the maintenance of fidelity.
2.7. Reflection
The theme “reflection” emanates from the overwhelming believe within the literature that for simulation to be a positive learning experience, nurses need the opportunity to discuss their findings, and anchor their experiences to the cognitive frameworks they already possess. To this end, reflection can be encapsulated within the notion of “post-engagement”; this is the phase when the debriefing of the simulation experience occurs; many of the writers emphasise this process is essential as this is where the greatest learning occurs [17,38].
Within the study of Lasater [38] one of the unexpected themes of the focus group was stated spontaneously and discussed throughout the session by most of the participants: a strong desire for more direct feedback from the simulation facilitator. Most of the feedback given during the study focused on being supportive, pointing out the positive aspects of the students’ performances and building on their strengths. However, most of the focus group participants wanted more definitive and straightforward feedback, including the severity of the patient outcomes if the judgements they exercised had been followed in reality. Reflecting upon performance within the peer group, facilitated by the teacher is a means of communication whereby individuals receive information about their progress in mastering skills or activities or achieving their learning objectives [48]. The learner learns from direct self-generated feedback on the overall success of the encounter.
In complex simulations, interruptions to discuss decisions and situations are likely to interrupt the ongoing scenario. Videotaping these sessions would be preferred for debriefing purposes. The debriefing process is particularly important when the simulation is complex [52]. For learning to take place, students need to be able to go through the process of reflection and conceptualisation to adapt and reconstruct their cognitive frameworks. Thiagarajan [52] suggests creating a structured debriefing process that touches on certain steps. For example, allowing students to vent their emotions will promote more objecttive reflection; sharing insights will provide generalisations for discussion; hypothesis generation can create principles for further exploration; “what-if” questions facilitate expansion of principles. All of these steps in structured debriefing process aid in creating meaning for students and making the simulation a learning experience. To enhance learning further, Carlson et al., [52] encouraged students to describe their practical learning experiences and use Benner’s [18] model to assess their level of proficiency. Indeed, self-assessments may help clarify to students where they are in the development of nursing skills and clarify what they are striving for.
Within the findings of the study undertaken by Lasater [38] she suggested that improved reflection through the debriefing process following the simulation experience was key to facilitate the clinical judgment process. Indeed, debriefing, conducted with student peers, allows students to reflect on their experiences and integrate the new cognitive learning from the simulation exercise [54,55].
It can be concluded that the literature suggests that reflection upon the learning experience is essential for true learning to take place. This process is enhanced if the feedback is honest and constructive in its nature. Collaborative elaboration within a peer group would appear to further facilitate learning by all within the group.
3. CONTRIBUTION TO KNOWLEDGE AND PRACTICE
From the literature reviewed, it can be established that clear phases are advocated in every simulation session with a suitable underpinning educational philosophy, a constructivist approach has many merits in facilitating meaningful learning and developing clinical judgement [21,38]. Also, the integration of a model of escalation from novice to expert, such as that proposed by Benner [18], within the activation phase would be considered advantageous. The following framework (Figure 1) is presented, which is drawn from the current literature; the themes as discussed above can be conceptualised as a useful workable model in which to guide the simulation process with due consideration to the preparedness, activation and reflection phases. The application, development and refining of such a model through practitionerresearch will serve to inform the continued development of simulations within nurse education and seek to
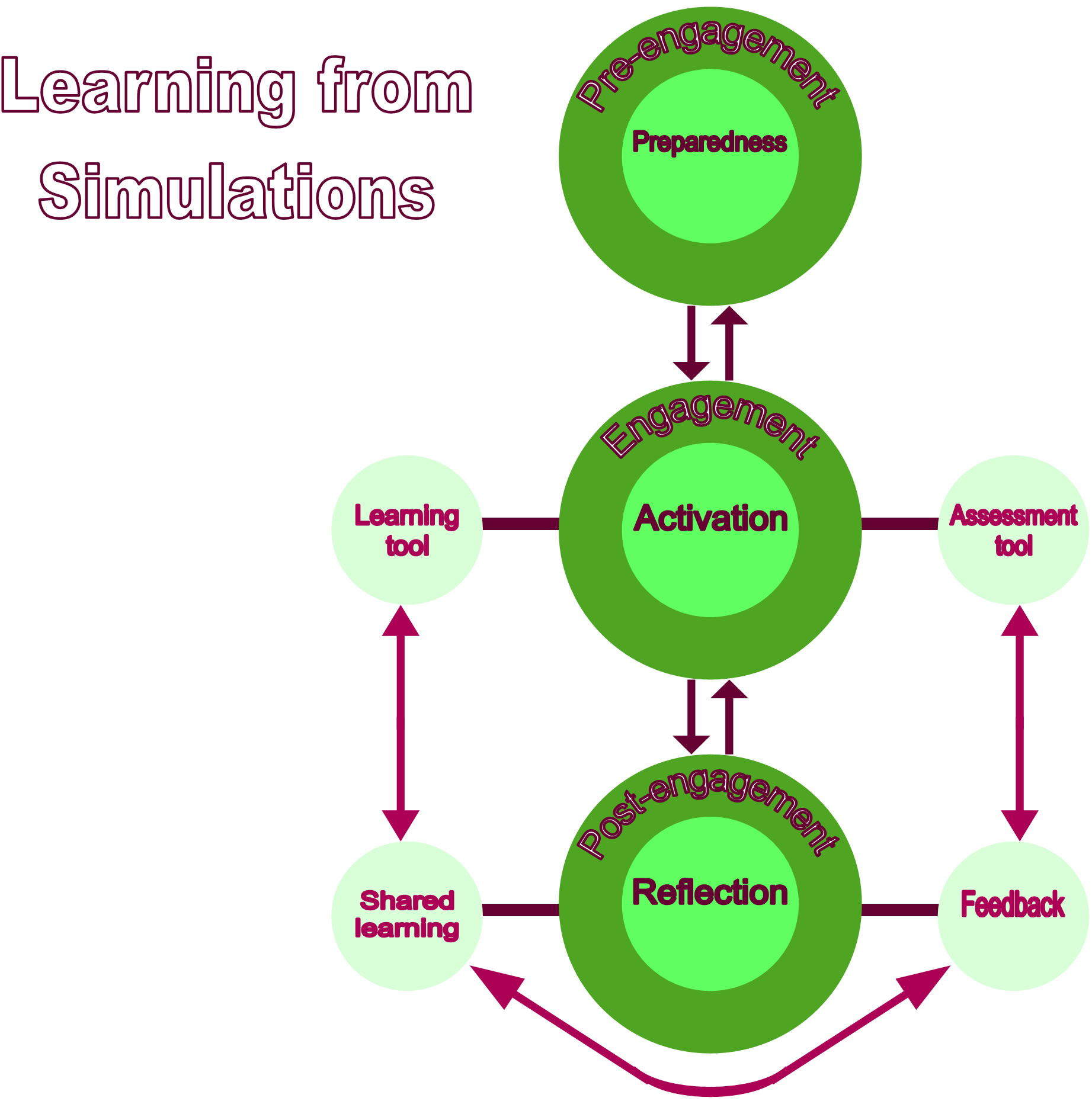
Figure 1. A model to enhance learning within simulations
develop this early model for practice. Through a consistent and insightful approach to teaching, dynamic learning will be assured within this very important aspect of engaging the learner within a process of meaningful decision-making.
4. SUMMARY
There is a clear rise in the significance of simulation as an important adjunct within nurse education to establish, develop and maintain clinical skills [1-3,11]. There is an obvious need to provide training opportunities that ensure patient safety, especially when learners are inexperienced and their procedural skills are at an early stage of development [18]. A structured approach through the application of a model for simulation teaching would ensure that all students receive the opportunity to apply their knowledge and skills in a real world setting, and to identify and address their individual learning needs before carrying out procedures on real patients. One of the major hurdles facing nurse education is to expand the fidelity within the simulation to evoke substantial aspects of the real world in a fully interactive manner [14], an educational model to underpin this process can only be a strength.
REFERENCES
- Nursing Midwifery Council (2007) Supporting direct care through simulated practice learning in the pre-registration nurse programmes. http://www.nmc-uk.org
- Nursing and Midwifery Council and the Council of Deans (UK) (2007) Simulation and practice learning project: Outcome of a pilot study to test principles of auditing simulated practice learning environments in the preregistration nursing programme. Final Report December 2007, NMC, London.
- NHS West Midlands (2007) Investing for Health. www.ifh.westmidlands.nhs.uk
- Sharif, F. and Masoumi, S. (2005) A qualitative study of nursing student experiences of clinical practice. BMC nursing, 4, 6-10. doi:10.1186/1472-6955-4-6
- Wellard, S., Woolf, R. and Gleeson, L. (2007) Exploring the use of clinical laboratories in undergraduate nursing programmes in regional Australia. International Journal of Nursing Education Scholarship, 4, 1-11.
- Scott, C. (2001) Back to basics. Nursing Management, 8, 16-19.
- Santucci, J. (2004) Facilitating the transition into nursing practice: Concepts and strategies for mentoring new graduates. Journal of Nurses Staff Development, 20, 274- 284. doi:10.1097/00124645-200411000-00007
- Remmen, R., Scherpbier, A., van der Vleuten, C., Denekens, J., Derese, A. and Hermann, I. (2001) Effectiveness of basic clinical skills training programmes: A crosssectional comparison of four medical schools. Medical Education, 35, 121-128. doi:10.1046/j.1365-2923.2001.00835.x
- Gaba, D.M. (2004) The future vision of simulation in health care. Quality and Safety in Health Care, 13, 2-10. doi:10.1136/qshc.2004.009878
- Issenberg, S. B., McGaghie, W. C., Petrusa, E. R., Gordon, D. L. and Scalese, R. J. (2005) Features and uses of highfidelity medical simulations that lead to effective learning: A BEME systematic review. Medical Teacher, 27, 10-28. doi:10.1080/01421590500046924
- Department of Health (2011) A framework for technology enhanced learning. DH Publications, London. http://www.dh.gov.uk/publications
- Inter-Professional Education Collaborative Expert Panel (2011) Core competencies for inter-professional collaborative practice. Report of an expert panel, Washington DC.
- Hull, L., Arora, S., Kassab, E., Kneebone, R.L. and Sevdalis, N. (2011) Observational teamwork assessment for surgery (OTAS): Content validation and tool refinement. Journal of the American College of Surgeons, 212, 234-243. doi:10.1016/j.jamcollsurg.2010.11.001
- Campbell, S.H and Daley, K.M (2013) Simulation scenarios for nursing educators: Making it real. 2nd Edition, Springer Publishing Company, New York.
- Quinn, F.M. (2000) Principles and practice of nurse education. Stanley Thornes Publishers, Gloucester.
- West Midlands Regional Strategic Health Authority (WMSHA) (2009) Scoping the future of clinical skills and simulation. Final Report, WMSHA, Birmingham.
- Waldner, M.H. and Olson, J.K. (2007) Taking the patient to the classroom: Applying theoretical frameworks to simulation in nursing education. International Journal of Nursing Education, 4, 1-14.
- Benner, P. (1984) From novice to expert: Excellence and power in clinical nursing practice. Addison-Wesley Publishing Co., Menlo Park.
- Kolb, D. (1984) Experiential learning: Experience as the source of learning and development. Prentice-Hall, Englewood Cliffs.
- Sewchuk, D. (2005) Experiential learning: A theoretical framework for perioperative education. AORN Journal, 81, 1311-1318. doi:10.1016/S0001-2092(06)60396-7
- Parker, B.C. and Myrick, F. (2009) A critical examination of high-fidelity human patient simulation within the context of nursing pedagogy. Nurse Education Today, 29, 322-329. doi:10.1016/j.nedt.2008.10.012
- Dabbagh, N. and Bannan-Ritland, B. (2005) Online learning: Concepts, strategies, and applications. Pearson Education, Upper Saddle River.
- Tomei, L.A. (2005) Taxonomy for the education domain. Information Science, Hershey.
- Bullock, I., Davis, M., Lockey, A. and Mackway-Jones, K. (2008) Pocket guide to teaching for medical instructors. BMJ Publishing, London.
- Bauersfeld, H. (1995) The structuring of the structures: Development and function of mathematizing as a social practice. In: Steffe, L.P. and Gale, J., Eds., Constructivism in Education, Lawrence Erlbaum Associates Publishers, Hillsdale.
- Gamoran, A., Secada, W.G. and Marrett, C.B. (1998) The organizational context of teaching. Educational Evaluation and Policy Analysis, 20, 229-252.
- Davis, M. and Forrest, K. (2008) How to teach continuing medical education. Wiley-Blackwell, Oxford.
- Day-black, C. and Watties-Daniels, A.D. (2006) Cutting edge technology to enhance nursing classroom instruction at Coppin State University. ABNF Journal, 17, 103-106.
- Skiba, D.J. (2007) Nursing education 2.0: Second life. Nursing Education Perspectives, 28, 156-157.
- Vygotsky, L.S. (1978). Mind in society: The development of higher mental processes. Harvard University Press, Cambridge.
- Van Meter, P. and Stevens, R.J. (2000) The role of theory in the study of peer collaboration. The journal of Experimental Education, 69, 13-27. doi:10.1080/00220970009600652
- Greeno, J. G., Collins, A. M. and Resnick, L. B. (1996). Cognition and learning. In: Berliner, D. and Calfee, R., Eds., Handbook of Educational Psychology, MacMillian, New York, 15-41.
- Duffy, T.M. and Jonassen, D. (1992) Constructivism and the technology of instruction: A conversation. Lawrence Erlbaum Associates, Hillsdale.
- Steinaker, N. and Bell, R. (1979) The experiential taxonomy: A new approach to teaching and learning. Academic Press, London.
- Fink, L.D. (2003) Creating significant learning experiences: An integrated approach to designing college courses. Jossey-Bass, San Francisco.
- Humphreys, M. (2002) Using simulations in resuscitation teaching. Resuscitation, 1, 7-10.
- Morgan, R. (2006) Using clinical skills laboratories to promote theory practice integration during first practice placement—An Irish perspective. Journal of Clinical Nursing, 15, 155-165. doi:10.1111/j.1365-2702.2006.01237.x
- Lasater, K. (2007) High-fidelity simulation and the development of clinical judgement: Students’ experiences. Journal of Nursing Education, 46, 269-275.
- Smith, S.J. and Roehrs, C.J. (2009) High-fidelity simulation: Factors correlated with nursing student satisfaction and self-confidence. Nursing Education Perspectives, 30, 74-78.
- Scherer, Y.K., Bruce, S.A. and Runkawatt, V. (2007) A comparison of clinical simulation and case study presentation on nurse practitioner students’ knowledge and confidence in managing a cardiac event. International Journal of Nursing Education Scholarship, 4, Article 22.
- Jeffries, P.R. (2005) A framework for designing, implementing, and evaluating simulations used as teaching strategies in nursing. Nurse Education Perspectives, 26, 96-103.
- Dunkin, M.J. and Biddle, B.J. (1974). The study of teaching. Holt, Rinehart and Winston, Inc., New York.
- Jeffries, P.R. (2008) Getting in S.T.E.P. with simulations: Simulations take educator preparation. Nurse Education Perspectives, 29, 70-73.
- Humphreys, M. (2004) Facilitating adult learning. Chapter 1. In: Resuscitation Council (UK), Eds., Advanced Life Support Instructor Manual: Resuscitation Council (UK), BMJ Publishing, London, pp. 48-54.
- Ahmad, F. (2008) Presage, context, process and product: Influencing variables in literature instruction in an ESL Context. GEMA Online Journal of Language Studies, 8, 1-21.
- Amitai, Z., Small, S.D. and Wolpe, P.R. (2000) Patient safety and simulation-based medical education. Medical Teacher, 22, 489-495. doi:10.1080/01421590050110777
- Fritz, P.Z., Gray, T. and Flanagan, B. (2007) Review of mannequin-based high-fidelity simulation in emergency medicine. Emergency Medicine Australia, 20, 1-9. doi:10.1111/j.1742-6723.2007.01022.x
- Campbell, S.H. and Daley, K. (2009) Simulation scenarios for nursing education: Making it real. Springer Publishing, New York.
- Kneebone, R.L., Kidd, J., Nestel, D., Barnet, A., Lo, B., King, R., Yang, G.Z. and Brown, R. (2005) Blurring the boundaries scenario based simulation in a clinical setting. Medical Education, 39, 580-587. doi:10.1111/j.1365-2929.2005.02110.x
- Janes, B. and Cooper, J. (1996) Simulations in nursing education. Australian Journal of Advanced Nursing, 13, 35-38.
- Maslow, A. and Lowery, R. (Ed.) (1998). Toward a psychology of being. 3rd Edition, Wiley & Sons, Hoboken.
- Thiagaraja, S. (1998) The myths and realities of simulations in performance technology. Educational Technology, 35, 35-41.
- Carlson, L., Crawford, N. and Contrades, S. (2005) Nursing student novice to expert: Benner’s research applied to education. Journal of Nursing Education, 28, 188-190.
- Seropian, M.A., Brown, K., Gavilanes, J.S. and Driggers, B. (2004) Simulation: Not just a manikin. Journal of Nursing Education, 43, 164-169.
- Mezirow, J. (2000) Learning as transformation: Critical perspectives on a theory in progress. Jossey Bass, San Francisco.