Open Journal of Internal Medicine
Vol.1 No.2(2011), Article ID:7695,4 pages DOI:10.4236/ojim.2011.12007
Fatal septic shock caused by candida myocarditis associated with malignant lymphoma and Epstein-Barr virus mediated disorder
![]()
Department of Cardiology, Hospital Group Twente, Hengelo, The Netherlands.
Email: *samsaid@home.nl
Received 1 June 2011; revised 13 July 2011; accepted 21 July 2011.
Keywords: Septic Shock; Candida Myocarditis; Epstein-Barr Virus Mediated Lymphoproliferative Disorder; Malignant Lymphoma; Arrhythmia
ABSTRACT
A 60-year-old man with known epilepsy was admitted to our hospital due to hypotension, fever and arrhythmia. He was treated medically and myocardial infarction was ruled out. Treatment of septic shock was established according to the guidelines of the early goal-guided therapy including vasopressors, inotropic agents, mechanical ventilation, and hemofiltration in combination with empirical treatment with antimicrobial drugs and hydrocortisone. The patient’s condition deteriorated rapidly into multi-organ failure resulting in a fatal outcome. Ante-mortem blood cultures were sterile. Autopsy findings were compatible with Epstein-Barr virus mediated lymphoproliferative disorder, malignant lymphoma, disseminated candidiasis and candida myocarditis. Post-mortem blood and tissue cultures were positive for growth of candida glabrata and candida albicans, respectively. The postmortem examination documented Epstein-Barr virus mediated lymphoproliferative disorder and malignant small cell lymphoma associated with candida myocarditis. Prior to death, the patient did not receive antiviral or antifungal treatment. Fatal candida myocarditis associated with septic shock secondary to disseminated candidiasis in a 60-years old male patient with prior unknown immune compromised state caused by Epstein-Barr virus mediated lymphoproliferative disorder and malignant lymphoma is described.
1. INTRODUCTION
Myocarditis may have several etiologic agents. The most common are enteroviruses and adenoviruses. Myocarditis of any etiology usually presents with cardiac failure and ventricular arrhythmia. As a result, myocarditis is one of the most common causes of sudden death in patients without pre-existing structural heart disease [1].
Candida is a dimorphic fungus that exists as a commensal of warm-blooded animals including humans [2]. Due to the disturbance of the microflora, infection may occur in immuno-compromised individuals. The most commonly affected organs are the liver and spleen followed by the kidneys, brain, eyes and myocardium [3]. We describe a case of a 60-years old male patient with prior unrecognized immune compromised state caused by Epstein-Barr virus mediated lymphoproliferative disorder and malignant lymphoma who was presented with fatal candida myocarditis associated with septic shock secondary to disseminated candidiasis.
2. CASE REPORT
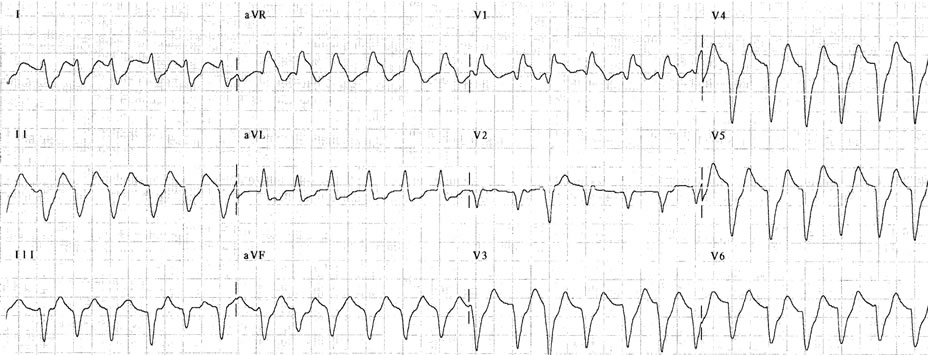
A 60-year-old man (weight of 100 kg and height of 185 cm) with known epilepsy was admitted to our hospital due to septic shock. His further medical history included gastric surgery after swallowing dental elements and a car accident few years earlier. The patient had a threedays history of general malaise, anorexia and shivering. On admission, the patient was tachypnoeic and sweaty with a blood pressure of 70/20 mmHg, a body temperature of 35.2˚C and an irregular pulse rate of 120 bpm. The patient was sedated, intubated and mechanically ventilated. The circulation was supported with inotropic agents, vasopressors and fluid regimens. Because of his septic shock the patient was initially treated according to the guidelines of the early goal-guided therapy [4]. Blood cultures were taken together with the initiation of an empiric treatment of a combination of antimicrobial therapy (ciprofloxacin and amoxicilline/clavulanic acid) and hydrocortison. Admission electrocardiograms (Figures 1(a) and (b)) showed atrial fibrillation with rapid ventricular response of 150/min, with wide QRS complex associated with alternating configuration of right and left bundle branch block patterns.
 (a)
(a)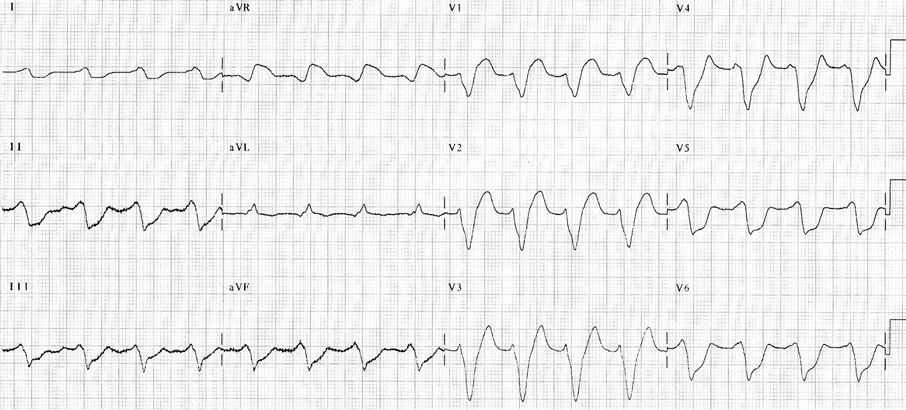 (b)
(b)
Figure 1. Admission electrocardiograms depicting atrial fibrillation with rapid ventricular rate and alternated configuration of left (a); and (b) right bundle branch block patterns.
Chemical (amiodaron) and electrical cardioversion were attempted due to atrial fibrillation but were unsuccessful to restore sinus rhythm. Emergency coronary angiography revealed no significant atherosclerotic coronary arterial disease. Chest X-ray illustrated cardiomegaly without infiltrative lesions or pleural effusion. Transesophageal echocardiography demonstrated mild pericardial effusion with diffuse left ventricular hypokinesia without valvular dysfunction nor cardiac tamponade. There were no vegetations. Laboratory investigation depicted biochemical signs of severe sepsis with elevated infection parameters of C-reactive protein (CRP) and leukocytosis, elevated troponine and CK levels. The liver and renal function tests were abnormal.
Ante-mortem serial blood cultures were negative for bacterial or fungal growth. Elevated serum lactate concentrations indicating global tissue hypoxia. Arterial blood gases revealed metabolic acidosis with a strongly negative base deficit.
Multi-slice computed tomography scan of thorax and abdomen showed enlarged mediastinal lymphe nodes, pleural effusion and para-aortal lymphadenopthy. Furthermore, diverticulosis and infiltrative lesions in the region of the gall bladder were found.
During the following hours, the condition of the patient deteriorated rapidly. Due to renal failure and sepsis, continuous high-volume veno-venous hemofiltration was carried out. Unfortunately the multi-organ failure developed in a non-resuscitationable state of septic shock. Three days after admission to the hospital the patient succumbed. Post-mortem examination was performed. Prior to death, the patient was not known with immunosuppressive conditions, illness or malignancy.
At post-mortem examination, the heart weighed 611 grams reflecting cardiomegaly without evidence of necrosis, fibrosis or infarction. The coronary arteries showed mild atherosclerotic changes with non-significant luminal narrowing. The cardiac valves did not show signs of valvulitis. Post-mortem blood culture showed growth of candida glabrata and tissue cultures (spleen and lungs) were positive for candida albicans.
Microscopic examination demonstrated fulminant myocarditis consisting of diffuse infiltration with lymphoid cells interposing the myocardial tissue (Figures 2(a)-(c)) and inflammatory reaction without granulomas.
 (a)
(a)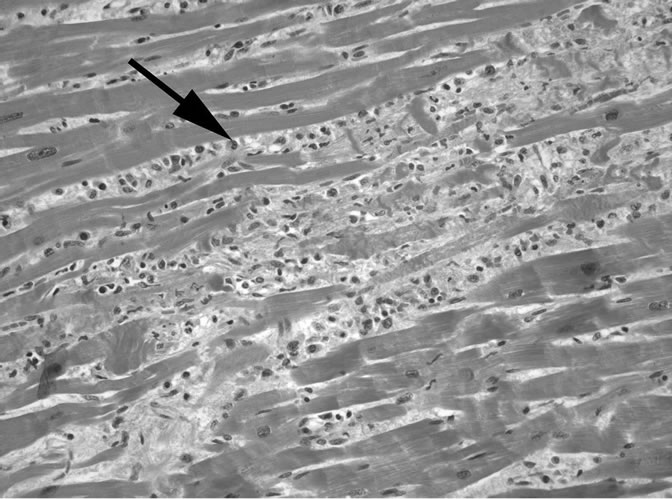 (b)
(b)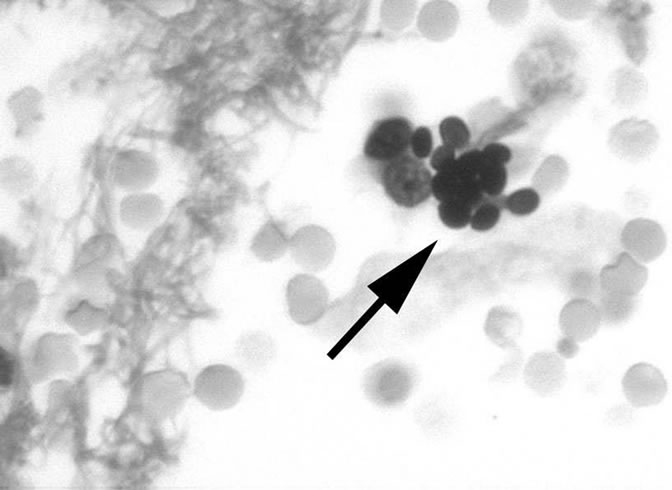 (c)
(c)
Figure 2. (a) Lymphocytes in myocardial tissue illustrated by positive Eber staining (20×) (arrows). (b) Standard HE staining (20×) of heart tissue allowing the demonstration of lymphocyte infiltration indicating myocarditis (arrow). (c) Pas-D staining (63×) showing the yeasts (arrow) in the myocardial tissue.
Special stains for fungi on cardiac sections were positive. Furthermore, generalized lymphadenopathy with Epstein-Barr virus (EBV)-mediated lymphoproliferative disorder was found (Figures 3(a)-(c)).
 (a)
(a)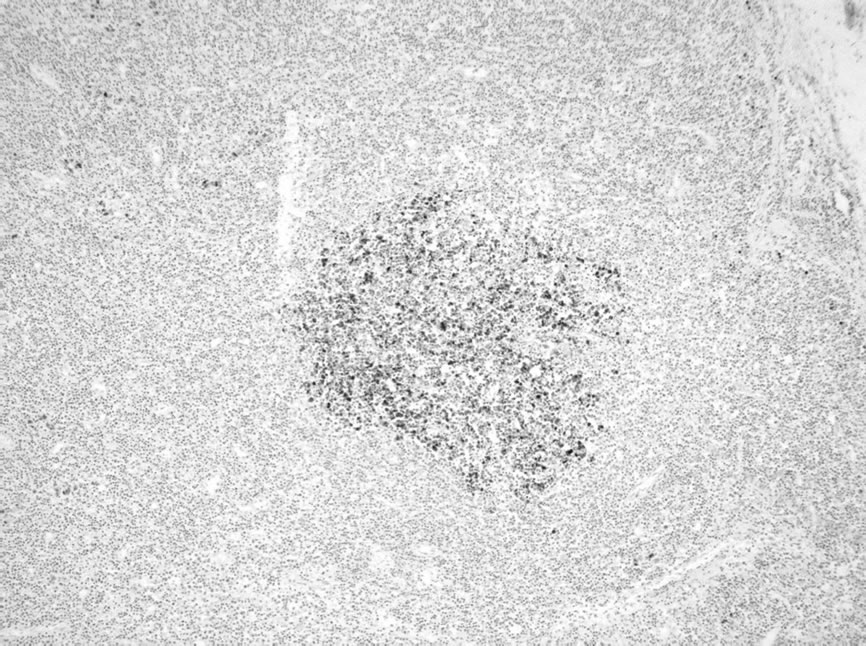 (b)
(b)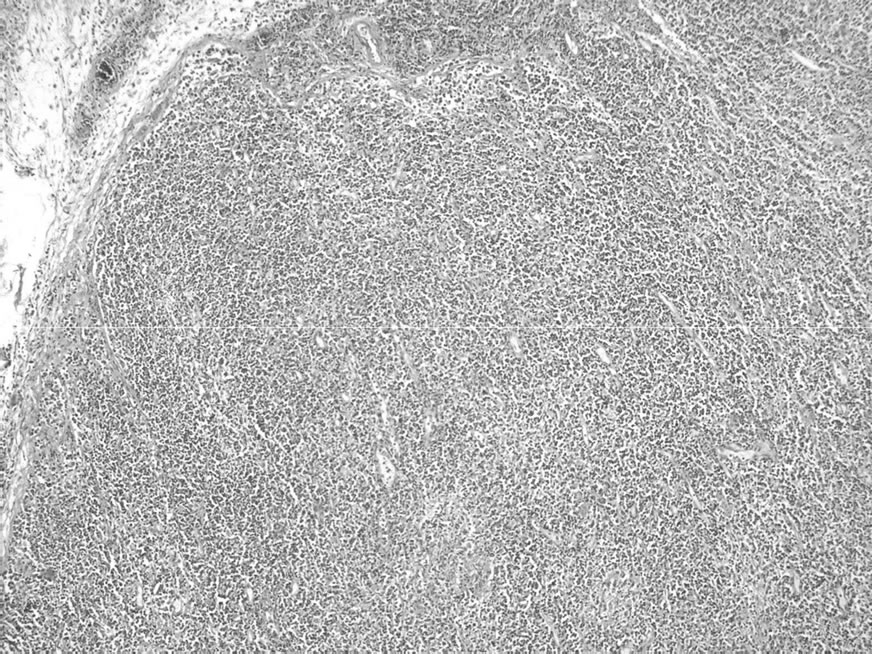 (c)
(c)
Figure 3. (a) Lymph node with Eber-positive cells (arrows) (40×); (b) HE staining (5×) of a lymph node illustrating the essentially normal lymphoid structure and architecture; (c) Eber-positive (5×) cells are shown in the lymph node (blue cluster of cells).
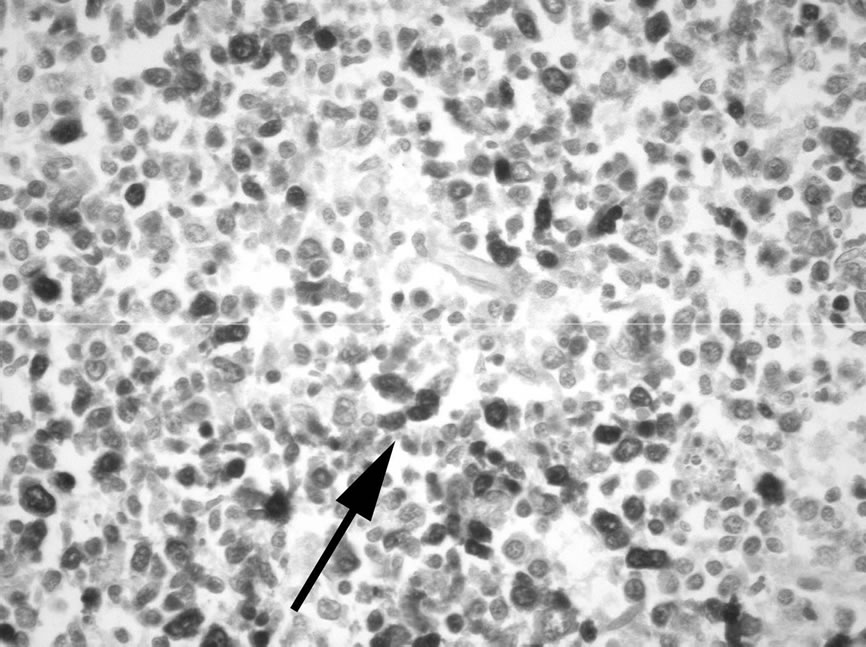
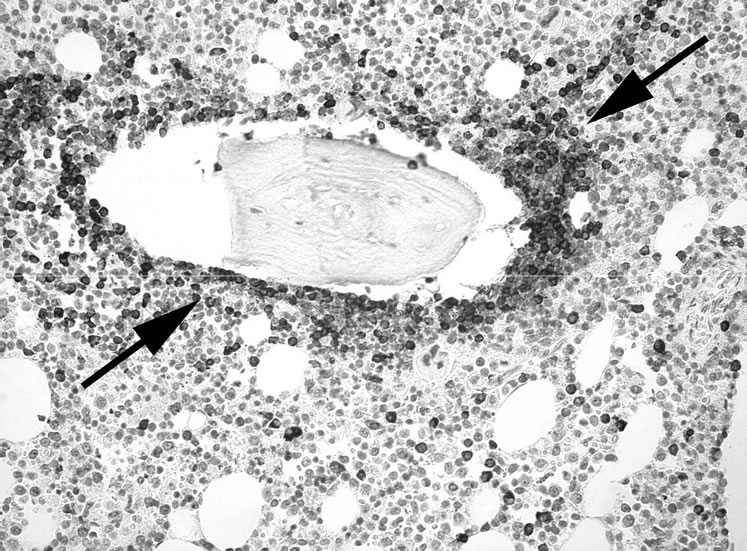
Bone marrow showed lymphoid foci localized intertrabecular and paratrabecular suggesting low-grade malignant small cell lymphoma (Figures 4(a)-(c)) which may have caused the immune compromised state giving rise to EBV-mediated lymphoproliferative reaction.
 (a)
(a)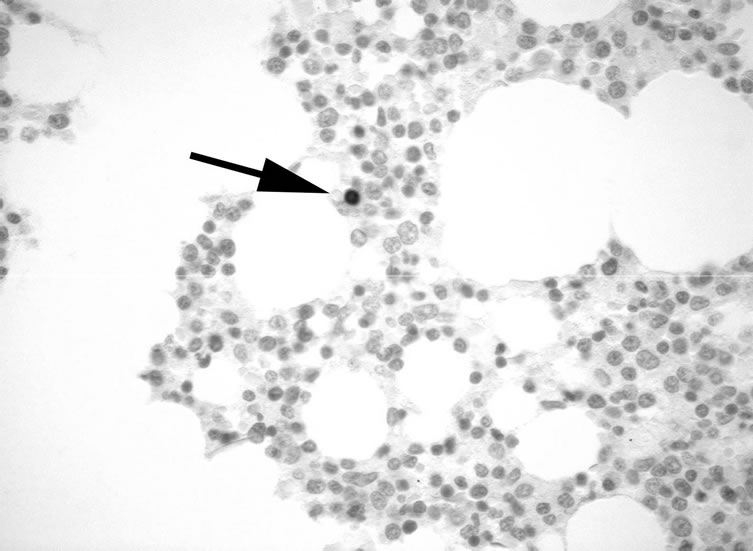 (b)
(b) (c)
(c)
Figure 4. (a) Bone marrow (20×) with paratrabecular groups of B-cells (CD79a-positive), indicating malignant lymphoma (arrows); (b) A single lymphocyte (arrow) in the bone marrow shows positive Eber staining (40×). Eber is a molecular biological staining method using in situ hybridization of Epstein Barr virus RNA; (c) Standard HE staining (20×) of bone marrow demonstrating infiltration of small lymphcytes (arrow). Compare this image with CD79a staining of bone marrow in (Figure 4(a)) in which the B-cells are specifically stained.
3. DISCUSSION
Candida is a dimorphic fungus that exists as a commensal of warm-blooded animals including humans [2]. Due to the disturbance of the microflora, infection may occur in immune compromised individuals. However the diagnosis of disseminated candida infection is difficult. The overall rate of positive blood cultures is around 20% [5]. In our patient, ante-mortem serial blood cultures remained negative as well.
Furthermore, candida infections have increased dramatically over the last two decades due to the wide spread use of broad-spectrum antibiotics, immunosuppressive treatment, and longer survival of immune compromised patients [2].
In the immune compromised hosts the inflammatory response may be minimal resulting in abscesses composed of candida organisms and necrotic tissue [3]. Different internal organs may be involved in disseminated candidiasis. The most commonly affected are the liver and spleen followed by the kidneys, brain, eyes and myocardium [3]. Acute infection of the heart (endocarditis, myocarditis and/or pericarditis) may occur secondary to various infectious conditions such as viral, bacterial and fungal agents [6]. The latter usually occurs in immune compromised patients. Predisposing factors for candida infection include central venous catheters, antibiotic use, underlying heart disease, open-heart surgery, prosthetic valves and intravenous heroin addiction [7,8]. Symptoms may resemble bacterial endocarditis such as fever, murmur, splenomegaly, congestive heart failure, petechiae, papules, pustules, nodules or ulcers [7]. Recently, a fatal case of bacterial myocarditis causing septic shock has been reported in a middle-aged cirrhotic patient [9]. Cardiac troponin is elevated in patients with acute myocarditis [6], as was the case in the current patient.
In a necropsy study of 168 cancer patients with candidiasis, 10% showed myocardial involvement. These 17 patients were among the 85 cases with disseminated candida infection. No signs or symptoms of cardiac dysfunction were detected in these cancer patients with cardiac candida infection contrasting the clinical and pathologic presentation of candida endocarditis [10].
In a post-mortem study of 50 patients with systemic candidiasis 31 were found to have myocardial involvement without valvulitis [11]. Myocardial involvement included abscesses in all 31 patients. Retrospectively in 22 patients ECG were obtained. Pronounced T-wave changes were found in 13 cases. A major new conduction disturbance was seen in 10 patients, supraventricular arrhythmias in 5, QRS alterations mimicking myocardial infarction in 3. Furthermore shock or hypotension was seen in 13 patients. In the remaining 19 patients with systemic candidiasis without myocardial focal invasion, 4 had minor T-wave changes and 1 had a supraventricular arrhythmia [11]. Our patient had atrial fibrillation with rapid ventricular response. The admission ECG demonstrated alternating left and right bundle branch block patterns.
It has recently been reported that cardiac microabscesses as a result of candida sepsis mimicked left ventricular non-compaction in a middle-aged man with hypopharyngeal carcinoma who died 3 weeks after receiving chemotherapy [12].
Our presented case had an acute and dramatic course with post-mortem diagnosed Epstein-Barr virus (EBV)- mediated lymphoproliferative disorder, low-grade small cell malignant lymphoma, septic shock, candida myocarditis and atrial fibrillation with intraventricular conduction disturbances.Early goal-guided therapy for septic shock was initiate [4]. Empirical antimicrobial treatment with a combination of amoxicilline/clavulanic acid and ciprofloxacine was started. The patient received no antiviral or antifungal treatment as the diagnosis was discovered and documented by post-mortem examination. Mortality of candida infection of the heart has been reported to be approximately 72% [7]. Candida infection of the heart should be considered as an etiologic factor in fatal myocarditis, pre-mortem effort should be made to diagnose such condition, as treatment with newer antifungal drugs, such as echinocandins, caspofungin, voriconazole and lipid preparations of amphotericin B may positively influence the outcome [7,13]. Reduction of mortality has been shown by the conventional sequential treatment of candida infection of the heart composed of amphotericin B for a period of at least 6-8 weeks followed by fluconazole [7].
4. CONCLUSIONS
It is concluded from this case presentation that antemortem undiagnosed malignant lymphoma may have mediated EBV lymphoproliferative condition causing immune suppressive state and consequently giving rise to disseminated candidiasis affecting different organs associated with multi-organ dysfunction. This resulted in severe septic shock, candida myocarditis and multi-organ failure leading to death. The diagnosis was fully established post-mortem. In patients presented with fever, hypotension and arrhythmias, candidiasis should be suspected.
5. ACKNOWLEDGEMENTS
The authors appreciate the assistance of Mr. R.H.A. Rieksen, Laboratory for Pathology Oost Nederland, Enschede for his excellent image production and Mrs. A. Geerdink and Mr. D. Maas, librarians of Hospital Group Twente for their assistance during the preparation of the manuscript.
REFERENCES
- Mason, J.W., Trehan, S. and Renlund, D.G. (2007) Myocarditis. In: Hall, J.B., Schmidt, G.A. and Wood, L.D.H. Eds., Principles of Critical Care, Springer, London, 1313- 1334.
- Molero, G., Díez-Orejas, R., Navarro-García, F., Monteoliva, L., Pla, J., Gil, C., Sanchez-Perez, M. and Nombela, C. (1998) Candida albicans: Genetics, dimorphism and pathogenicity. International Microbiology, 1, 95-106.
- Bennett, J.E. (1990) Mycosis. In: Maddell, G.L., Douglas, R.G. and Bennett, J.E., Eds., Principles and Practice of Infectious Diseases, Churchill Livingstone Inc Publications, New York, 1942-1954.
- Rivers, E., Nguyen, B., Havstad, S., Ressler, J., Muzzin, A., Knoblich, B., Peterson, E. and Tomlanovich, M. (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. The New England Journal of Medicine, 345, 1368-1377. doi:10.1056/NEJMoa010307
- Abbas, A.A.H. and Tapp, H.E. (2005) Disseminated candida infection in children treated for cancer: A report of five cases and review of the literature. Haema, 8, 497- 503.
- Dennert, R., Crijns, H.J. and Heymans, S. (2008) Acute viral myocarditis. European Heart Journal, 29, 2073- 2082. doi:10.1093/eurheartj/ehn296
- Baddley, J.W., Benjamin, D.K., Patel, M., Miro, J., Athan, E., Barsic, B., Bouza, E., Clara, L., Elliott, T., Kanafani, Z., Klein, J., Lerakis, S., Levine, D., Spelman, D., Rubeinstein, E., Tornos, P., Morris, A.J., Pappas, P., Fowler Jr, V.G., Chu, V.H. and Cabell, C. (2008) Candida infective endocarditis. European Journal of Clinical Microbiology & Infectious Diseases, 27, 519-529. doi:10.1007/s10096-008-0466-x
- Ellis, M.E., Al-Abdely, H., Sandridge, A., Greer, W. and Ventura, W. (2001) Fungal endocarditis: Evidence in the world literature, 1965-1995. Clinical Infectious Diseases, 32, 50-62. doi:10.1086/317550
- Nieuwenhuijs, D.J.F. and Zandstra, D.F. (2008) Bacterial myocarditis as a cause of fatal septic shock. The Netherlands Journal of Critical Care, 12, 285-287.
- Ihde, D.C., Roberts, W.C., Marr, K.C., Brereton, H.D., McGuire, W.P., Levine A.S. and Young, R.C. (1978) Cardiac candidiasis in cancer patients. Cancer, 41, 2364- 2371. doi:10.1002/1097-0142(197806)41:6<2364::AID-CNCR2820410640>3.0.CO;2-W
- Franklin, W.G., Simon, A.B. and Sodeman, T.M. (1976) Candida myocarditis without valvulitis. American Journal of Cardiology, 38, 924-928. doi:10.1016/0002-9149(76)90805-5
- Stöllberger, C., Preiser, J. and Finsterer, J. (2004) Histological detection of intramyocardial abscesses in candida sepsis mimicking left ventricular non-compaction/hypertrabeculation on echocardiography. Mycoses, 47, 72- 75.
- Einarsdottir, H.M., Danielsen, R. and Gottfredsson, M. (2002) Successful treatment of Candida glabrata myocarditis with voriconazole. Scandinavian Journal of Infectious Diseases, 34, 778-780. doi:10.1080/00365540260348635