 Open Journal of Depression 2013. Vol.2, No.4, 64-71 Published Online November 2013 in SciRes (http://www.scirp.org/journal/ojd) http://dx.doi.org/10.4236/ojd.2013.24012 Open Access 64 Mood-Related Negative Bias in Response to Affective Stimuli in Patients with Major Depression Rottraut Ille1,2*, Peter Hofmann2, Christoph Ebner2, Hans-Peter Kapfhammer2, Anne Schienle1 1Institute of Psychology, Karl-Franzens-University of Graz, Graz, Austria 2University Hospital of Psychiatry, Medical University of Graz, Graz, Austria Email: *rottraut.ille@uni-graz.at Received July 25th, 2013; revised August 30th, 2013; accepted September 8th, 2013 Copyright © 2013 Rottraut Ille et al. This is an open access article distributed under the Creative Commons At- tribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background: The study focuses on the type and degree of impairment in the processing of affective faces and scenes in patients afflicted with major depression (MD). We investigated effects of emotional traits, gender, depression severity, and cognitive performance. Method: Thirty MD patients (15 men, 15 women) and 30 healthy controls were presented with pictures of emotional facial expressions and affective scenes. They were asked to estimate the intensity and allocation of the emotions expressed by the faces as well as the elicited emotions by the scenes. Results: MD patients showed a broad impairment of emotion recogni- tion. Patients’ responses to happy faces suggested a negativity bias, which also became evident in the perception of emotional scenes. The negativity bias was stronger in male than female patients. Depression severity was negatively related to experience of happiness. Patient’s lower cognitive performance was associated with allocation accuracy of angry and disgusted faces. Conclusions: Our findings show accor- dance with the mood-congruency hypothesis. Depression treatment should put increased focus to the as- sociation between negative mood bias and social functioning. Keywords: Emotion Recognition; Emotion Experience; Impairment; Negativity Bias; Cognitive Performance; Severity of Depression Introduction Major Depression (MD) is characterized by low mood ac- companied by lowered self-esteem, and by loss of interest or pleasure in normally enjoyable activities (APA, 2000). With in- creasing severity of illness MD is associated with impaired so- cial functioning. The afflicted patients have a reduced social competence, emit fewer interpersonal behaviors and are less skillful in solving interpersonal problems (Persad & Polivy, 1993). Furthermore, several studies could verify biased proc- essing of emotional information (Bylsma et al., 2008; Persad & Polivy, 1993). Depressive disorder involves several types of emotional ab- normalities, most notably increased propensity to negative af- fect and reduced capacity to experience pleasure (Drevets, 2001). In order to explain how MD alters emotional reactivity three alternative approaches have been put forward (Bylsma et al., 2008): MD may alter emotional reactivity by increased negative reactivity, by reduced positive reactivity or by “emo- tion context insensitivity” (ECI; reduced positive and negative reactivity; Rottenberg et al., 2005). The pronounced tendency to experience negative emotions and the reduced tendency to experience positive emotions by patients with depression have been explained by the mood con- gruency hypothesis (Bower, 1981). It suggests that depressed mood may enhance the processing of mood congruent material and impair the processing of mood incongruent material. But several studies on depression (e.g., Persad & Polivy, 1993; Mikhailova et al., 1996) found no evidence for mood congru- ency effects. The ECI model states that individuals with depression will exhibit decreased reactivity to all emotion cues, regardless of valence (Rottenberg, 2005; Rottenberg et al., 2005; Rottenberg, 2007). For this reason, individuals with MD should display lowered responses to both positive and negative stimuli, in- cluding sadness. Data of a meta-analysis by Bylsma et al. (2008) confirmed the ECI hypothesis, suggesting an overall reduced emotional reactivity in MD, with the reduction larger for posi- tive stimuli. Results were comparable for self-reported experi- ence, expressive behavior, and peripheral physiology. Rotten- berg et al. (2005) found most pronounced attenuation in emo- tion experience reports. Furthermore, MD patients with the most pronounced ECI showed the most severe symptoms, the longest episodes of depression, and the poorest overall psycho- social functioning. Depression is also associated with abnormalities in the iden- tification of emotional facial expressions (Surguladze et al., 2004). Affective facial expressions are salient features in social interactions (Persad & Polivy, 1993). Therefore, the ability to accurately identify others’ emotional facial expressions is of considerable importance. According to previous data MD is characterized by a reduced ability to correctly identify affective facial expressions. *Corresponding author.  R. ILLE ET AL. Open Access 65 There are some inconsistencies, if deficits in facial expres- sion decoding are emotion-specific or more general. Findings from Mikhailova et al. (1996) attested poor recognition of hap- piness and sadness in patients with depression. Mendlewicz et al. (2005) reported a lower decoding accuracy of depressed patients only for angry facial expressions, while for happy, disgusted, sad, and fearful expressions they did not differ from healthy controls. Several authors also found an enhanced ten- dency of depressed patients to judge facial expressions as dis- playing negative affect (“negativity bias”; Hale, 1998; Mik- hailova et al., 1996; Milders et al., 2010). It could also be shown that severity of depressive symp- toms plays a role in recognition accuracy of facial expressions. Hale (1998) reported a positive relationship between judgments of negative emotions in facial expressions and depression se- verity. Results by Leppänen et al. (2004) revealed a correlation between depression symptom score and sadness bias in neutral faces. As most studies tested recognition performance in depression only for several emotions, it is not clear, whether this disorder is associated with a general deficit in affecting identification or with impairments in the recognition of specific emotions. Fur- thermore, it remains unresolved, whether this deficit can be seen as a mood-congruent interpretation bias (e.g., towards sadness) or as an overall deficient decoding of emotional facial expressions. To summarize, results concerning decoding performance in MD are inconsistent. This may be a consequence of different intensities of facial expressions presented. Furthermore, MD patients must be seen as a heterogeneous population, with co- morbidity of several mental disorders like anxiety disorders, posttraumatic stress disorder or addiction. As a consequence, patients’ emotional reactivity may be different. Finally, depressive symptoms differ between genders (Angst et al., 2002; Kockler & Heun, 2002; Scheibe et al., 2003). Ag- gression and especially anger attacks are more prevalent in males compared to females (Winkler et al., 2005), while fe- males report more anxiety (Scheibe et al., 2003). This may result in a gender-specific difference of emotion experience and perception of emotions in others. Furthermore, several authors have reported that in healthy subjects females show greater identification accuracy of affective facial expressions compared to men (e.g., Cellerino et al., 2004; Kring & Gordon, 1998). It would be of interest if women suffering from depression can benefit from this advantage. To our knowledge, no previous studies have investigated emotion experience and allocation accuracy of emotional facial expressions simultaneously in patients afflicted with MD. Es- timation of affective scenes may provide information about patients’ mood state. The present study focuses on the type and degree of impair- ment in the processing of affective faces and scenes in patients with depressive disorder. We investigated effects of emo- tional traits, gender, depression severity, and cognitive per- formance. Methods Participants We studied 30 patients with the diagnosis Major Depression (criteria according to DSM-IV), 15 men and 15 women (M = 48.1 years, SD = 10.5), who were inpatients at the University Hospital of Graz (Austria). Socio-economic status was based on the highest educational level completed. Mean years of educa- tion were 11.1 years (SD = 3.3). Pharmacologic therapy was applied to all patients (antidepressants: 23 patients, antidepres- sants and antipsychotics: 7 patients). We further tested 30 men- tally healthy subjects, 15 men and 15 women, matched for age and socio-economic status. They had been recruited by adver- tisements in a local newspaper. The control group underwent a standardized clinical interview (Mini-Dips; Margraf, 1994) to exclude the presence of mental disorders. Mean age of the con- trols was 45.4 years (SD = 9.8). Mean education level was 11.9 years (SD = 3.6). Groups did not differ in age (t (58) = 1.04, p = .300) and years of education (t (58) = .90, p = .370). Questionnaires Cognitive performance was assessed using the Test for Early Detection of Dementia (TFDD; Ihl et al., 2000). This scale ranges between 0 and 50 points and allows the detection of early signs of cognitive impairment. A score lower than 35 points indicates a tentative dementia diagnosis (exclusion crite- rion). The Cronbach’s alpha is .88. Habitual emotional reactivity was assessed by several self- report inventories: The Beck Depression Inventory (BDI; German version: Haut- zinger et al., 1994) assesses depressive symptomatology. Cron- bach’s alpha is .88. The Questionnaire for the Assessment of Disgust Proneness (QADS; Schienle et al., 2002a) measures disgust propensity and describes 37 situations, which have to be judged on 5-point scales with regard to the experienced disgust (0 = “not disgust- ing”; 4 = “very disgusting”; e.g., “You are just about to drink a glass of milk as you notice that it is spoiled”). The Cronbach’s alpha of the total scale is .90. The disgust sensitivity scale of the Disgust Propensity and Sensitivity Scale-Revised (DPSS-R; Van Overveld et al., 2006) assesses a person’s tendency to evaluate disgust experiences as negative (e.g., “It embarrasses me when I feel disgusted”). Pos- sible mean sores range from 1 (“never”) to 5 (“always”). The Cronbach’s alpha of the sensitivity scale is .77. The Trait scale of the State-Trait Anxiety Inventory (STAI; Laux et al., 1981) measures the frequency of anxious feel- ings on a 4-point scale. The Cronbach’s alpha of the scale is .88. The Trait scales of the State-Trait-Anger Inventory (STAXI; Schwenkmezger et al., 1992) assess trait anger as well as anger expression. All items are rated on 4-point scales. Internal con- sistence of the STAXI is .90. Stimuli for the Picture Perception Tasks All participants viewed emotional scenes and facial expres- sions on a computer screen (notebook, 15 inches). The partici- pants sat at about 50 cm from the screen. Before starting the experiment participants were asked for their understanding of basic emotions by a short verbal description. Forty-two pictures with emotional facial expressions depict- ing happiness (6), fear (6), sadness (6), anger (6), disgust (6), and surprise (6) from the Karolinska-Set (Lundquist et al., 1998) were presented. Half of the posers were female, half were male. Participants were asked to view the faces as long as necessary for getting an impression of the emotion displayed. Maximum presentation time for each picture was 10 seconds.  R. ILLE ET AL. Open Access 66 Twenty-four emotion-relevant scenes for the induction of happiness (6), fear (6), and disgust (6) were presented. Most scenes were taken from the International Affective Picture Sys- tem (IAPS; Lang et al., 2001). Disgust-inducing pictures were developed by Schienle et al. (2002b) and included scenes with animals (maggots, bluebottles, and slugs), a dirty toilet, carrion and an eczematous face. The fear-inducing pictures showed threatening situations either through attacks of animals (“dog with its teeth bared”, IAPS 1300; “white shark”, developed by the authors) or human attacks (“man threatening a woman with a knife”, IAPS 6350; “men with pistol”, IAPS 6230; “war scene”, IAPS 6940; “masked robber”, IAPS 6370). Happy pic- tures included animals (“baby seal”, IAPS 1440; “young rab- bits”, IAPS 1750; “playing dolphins”, IAPS 1920) and food (“roast chicken”, IAPS 7230; “gateau”, IAPS 7282; “ice cream”, IAPS 7330). The stimulus material had been matched for item difficulty, complexity, brightness and colour. Since the IAPS does not include pictures which reliably induce anger, sadness and surprise these categories were omitted. It is known that IAPS scenes which should induce sadness or anger usually produce mixed emotions (e.g., 50% anger, 50% sadness). Maximum presentation time for each picture was 10 seconds. Then, the subject was asked to rate the pictures on a 9-point scale within 10 seconds. For each facial expression subjects rated how intense the depicted person experienced the six basic emotions (e.g., “Please indicate how intense the depicted per- son experienced disgust”: 1 = very little; 9 = very intense). For the scenes, subjects rated how intense the six basic emotions were induced by a particular picture (e.g., “Please indicate how intense you experienced disgust while viewing the picture”: 1 = very little, 9 = very intense). Asking the participants to rate emotion intensities of facial expressions and scenes for all basic emotions (graded choice) allowed the analysis of quantitative (intensity) as well as quali- tative (classification accuracy) emotion processing deficits. To avoid position effects, the order of the two-picture-per- caption-tasks (recognition vs. experience), order of pictures, and order of basic emotions to rate was randomised. Statistical Analysis All statistical analyses were carried out using SPSS Statistics 19.0 for Windows. Descriptive statistics were performed using Student’s t-tests, and for group comparisons ANOVAS were calculated. We computed mean intensity ratings of all six basic emotions for affective facial expressions. For estimation of af- fective faces repeated measures analyses of variance were car- ried out for each emotion category separately (2 × 6 ANOVAs), with group and rater’s sex as between-subjects factors. For pairwise comparisons of significant interactions Student t-tests were used. F-values were Greenhouse-Geisser-adjusted if nec- essary. All ε were > .50. Classification accuracy of target emo- tions was calculated as difference between rated target emotion intensity (e.g., rated disgust intensity for disgusted facial ex- pression) and mean intensity of all non-target emotions (fear, anger, sadness, happiness, and surprise). Effect sizes were cal- culated by Cohen’s d. Results Group Comparisons for the Questionnaires MD patients scored higher for depressive symptoms (BDI; t (58) = 13.68, p < .001), trait anxiety (STAI; t (58) = 11.21, p < .001), anger expression (STAXI; trait anger: F (1, 58) = 18.26, p < .001; “Anger in”: F (1, 58) = 75.37, p < .001), disgust pro- pensity (QADS; t (58) = 5.16, p < .001), and disgust sensi- tivity (DPSS-R; t (58) = 4.16, p < .001). Patients also showed lower cognitive performance (TFDD) than controls (t (58) = 5.52, p < .001) (Table 1). We found a sex x group interaction for trait anger (F (1, 58) = 2.83, p = .045). Males with depres- sion reported higher trait anger (M = 24.27, SD = 3.73) com- pared to females with MD (M = 20.21, SD = 5.40; t (28) = 2.37, p = .025). Group Comparisons for the Picture Perception Tasks Facial Expressions 1) Perceived intensities of target emotions (Table 2): Ana- lyzing the intensity ratings of the six target emotions (anger, disgust, sadness, fear, happiness, and surprise; e.g., disgust intensity in faces depicting disgust) we revealed a significant interaction for emotion x group (F (5, 280) = 2.53, p = .042). Patients reported lower intensities than controls for surprised (t (58) = 2.45, p = .017; d = .58) and for angry faces (t (58) = 2.12, p = .038; d = .78). Table 1. Means (Standard Deviations) of questionnaires in MD patients and con- trols. MD patients Controls p (n = 30) (n = 30) TFDD 41.41 (3.97) 45.97 (2.03) <.001 BDI 28.42 (8.66) 3.07 (4.95) <.001 Mean QADS 2.88 (.70) 2.02 (.59) <.001 DPSS-R 23.17 (7.23) 16.10 (5.88) <.001 STAI 57.68 (7.54) 32.03 (9.67) <.001 STAXI Trait Anger 21.81 (4.96) 16.67 (4.04) <.001 Anger-In 21.46 (4.74) 12.37 (3.02) <.001 Anger-Out 12.58 (3.43) 11.37 (2.66) .143 Anger Control 23.08 (4.39) 24.03 (5.01) .454 Note: TFDD (Test for Early Detection of Dementia); BDI (The Beck Depression Inventory); QADS (The Questionnaire for the Assessment of Disgust Proneness); DPSS-R (Disgust Propensity and Sensitivity Scale-Revised); STAI (State-Trait Anxiety Inventory); STAXI (State-Trait-Anger Inventory). Table 2. Means and standard deviations (SD) for target emotion intensities of facial expressions and scenes. Faces Scenes MD Patients Controls MD Patients Controls Fear 6.47 (1.34)5.85 (1.95) 7.67 (1.50) 5.97 (2.43) Disgust 6.59 (1.83)6.61 (2.15) 6.91 (1.58) 5.67 (1.59) Happiness 7.32 (1.69)7.91 (1.04) 6.52 (2.01) 6.59 (1.84) Anger 6.93 (1.49)7.65 (1.09) Sadness 6.39 (1.61)6.59 (1.35) Surprise 7.42 (1.05)7.96 (.79)  R. ILLE ET AL. Open Access 67 2) Classification accuracy of target emotions (Figure 1): For assessing participants’ classification accuracy of facial expres- sions we calculated the difference between the target emotion intensity and the mean of all non-target intensity ratings. Analyses revealed a significant main effect for group (F (1, 50) = 16.24, p < .001) and for sex (F (1, 50) = 15.21, p < .001). Patients displayed lower allocation accuracy of affective faces compared to controls, and males showed lower classification accuracy compared to females. Furthermore, we found a sig- nificant emotion x group interaction (F (5, 280) = 3.31, p = .006). Patients showed lower allocation accuracy than con- trols for all emotions with exception of fear: surprise (t (58) = 3.48, p = .001, d = .90), anger (t (58) = 3.36, p = .001, d = .86), happiness (t (58) = 3.32, p = .002, d = .86), sadness (t (58) = 2.91, p = .005, d = .75), and disgust (t (58) = 2.40, p = .020, d = .62). Patients assessed all negative non-target emotions in surprised faces more intense than controls (F (5, 280) = 4.69, p< .001; anger: t (58) = 2.79, p = .007; sadness: t (58) = 2.44, p = .018; fear: t (58) = 2.39, p = .020; disgust (t (58) = 2.24, p = .029). In sad faces patients also estimated all negative non-target emotions more intense than controls (F (5, 280) = 4.71, p = .002; anger: t (58) = 3.24, p = .002; fear: t (58) = 3.18, p = .002; disgust (t (58) = 2.34, p = .023). In fearful faces pa- tients rated more anger than controls (F (5, 280) = 4.87, P < .001; (t(58) = 2.64, P =.011). Moreover, compared to con- trols, patients rated higher intensities of disgust for angry faces (patients: M = 2.03, SD = 2.40; controls: M = 3.63, SD = 2.48; t (58) = 2.53, p = .014). Also for happy faces patients reported higher intensities for all negative emotions (F (5, 280) = 5.13, p =.011; fear: t (58) = 3.14, p = .003; disgust: t (58) = 3.13, p = .003; anger: t (58) = 2.68, p = .010; sadness: t (58) = 2.90, p = .005). Furthermore, we found an emotion x group x sex in- teraction for intensity ratings of happy faces (F (5, 280) = 3.34, p = .047). Compared to females, male MD patients estimated all negative emotions more intense (anger: t (28) = 2.18, p = .038; sadness: t (28) = 2.27, p = .035; fear: t (28) = 2.45, p = .021; disgust: (t (28) = 2.24, p = .035). Furthermore, male DisgustAngerFearSadness HappinessSurprise 0 1 2 3 4 5 6 7 p = 0.020 p = 0.001 p = 0.264 p = 0.005 p = 0.002 p = 0.001 MD Control Figure 1. Group comparison of the mean scores (standard errors) for classifica- tion accuracy of affective faces. patients rated happy faces less happy (t (28) = 2.49, p = .021) than females. The controls’ happiness ratings did not differ between males and females (all p > .106). 3) Perception of neutral faces (Figure 2): We found a sig- nificant effect for group (F (1, 56) = 15.21, p < .001) and for sex (F (1, 56) = 7.47, p = .008). Patients rated neutral faces more intense than controls, and males rated neutral faces more intense compared to females. Affective Scenes 1) Intensity of target emotions (Table 2): Intensity analyses for the three target emotions (happiness, fear, disgust) showed a significant main effect for group (F (1, 58) = 10.86, p = .002), and an emotion x group interaction (F (2, 110) = 5.99, p = .003). Compared to controls MD patients reported higher intensities for the scenes eliciting fear (t (58) = 3.22, p = .002; d = .84) and disgust (t (58) = 3.00, p = .004; d = .78). Furthermore, we found a significant emotion x group interaction for happiness experience (F (5, 280) = 4.97, p = .012). Patients experienced happy scenes sadder than controls (t (58) = 2.09, p = .048). 2) Experience of neutral scenes (Figure 3): Ratings of the neutral scenes displayed a main effect for group (F (1, 58) = 26.52, p < .001). Patients rated neutral scenes more intense than controls. Correlative Analyses MD patients showed a significant negative correlation be- tween severity of depressive symptoms (BDI score) and ex- perience of happiness in happiness-inducing (r = −.47, p = .019) as well as neutral scenes (r = −.55, p = .005). Severity of de- pressive symptoms was also correlated to experience of sadness in fearful (r = .42, p = .039) and neutral (r = .43, p = .031) scenes (Figure 4). But we found no association between de- pression severity and cognitive performance (r = −.13, p = .522). Patients’ cognitive performance was associated with allocation accuracy of anger (r = .55, p = .002) and disgust (r = .49, DisgustAngerFearSadness HappinessSurprise 0 1 2 3 4 5 6 7 p = 0.002 p = 0.001p = 0.001 p = 0.028 p = 0.058 p = 0.002 MD Control Figure 2. Group comparison of the mean scores (standard errors) for intensity ratings of neutral faces.  R. ILLE ET AL. Open Access 68 p = .007). But there was no relationship between cognitive per- formance and recognition accuracy in controls (all p > .290). “Anger in” score of patients was negatively related to experi- ence of happiness (r = −.42, p = .032). Patients’ disgust pro- pensity (mean QADS) was correlated with disgust ratings of fearful faces (r = .53, p = .002), angry faces (r = .47, p = .010), and sad faces (r = .38, p = .041) (Figure 5) as well as with dis- gust perception in fear-inducing (r = .49, p = .007) and disgust- ing (r = .64, p < .001) scenes (Figure 6). In controls we found a positive relationship between disgust propensity and intensity rating of disgusting scenes (r = .64, p < .001). Discussion Our results point to a general discrimination impairment of negative facial emotions in MD patients. This is contrary to several previous studies that report emotion-specific deficits in this mental disorder (e.g., Mendlewicz et al., 2005). Patients showed lower classification accuracy than controls for all nega- tive facial emotions with exception of fear. Fearful faces were poorly recognized also in healthy controls, indicating high task difficulty. The patients’ lower allocation accuracy was due to higher intensity ratings of all negative non-target emotions. But patients rated negative non-target emotions more intense also in happy faces, showing a negativity bias that cannot be explained by task difficulty. Happiness usually yields greatest accuracy, while negative emotions, especially fear, are less easily discriminable (Du & Martinez, 2013; Ekman & Friesen, 1976; Johnston et al., 2001). Our data are consistent with Surguladze et al., (2004) who reported a response bias in patients with depressive disorder judging happy faces as less happy compared to healthy volunteers. DisgustAngerFearSadness HappinessSurprise 0 1 2 3 4 5 6 7 p < 0.001 p < 0.001p < 0.001p < 0.001 p = 0.063 p < 0.001 MD Control Figure 3. Group comparison of the mean scores (standard errors) for intensity ratings of neutral scenes. Happiness in happy−inducing scenes Depression severity 10 15 20 25 30 35 40 45 123456789 r = −0.467 p = 0.019 Happiness in neutral scenes 123456789 r = −0.547 p = 0.005 Sadness in fear−inducing scenes Depression severity 10 15 20 25 30 35 40 45 123456789 r = 0.415 p = 0.039 Sadness in neutral scenes 123456789 r = 0.433 p = 0.031 Figure 4. MD patients: Correlations between depression severity (BDI score) and happiness ratings in happy-inducing and neutral scenes (above) respectively sadness ratings in fear-inducing and neutral scenes (below). 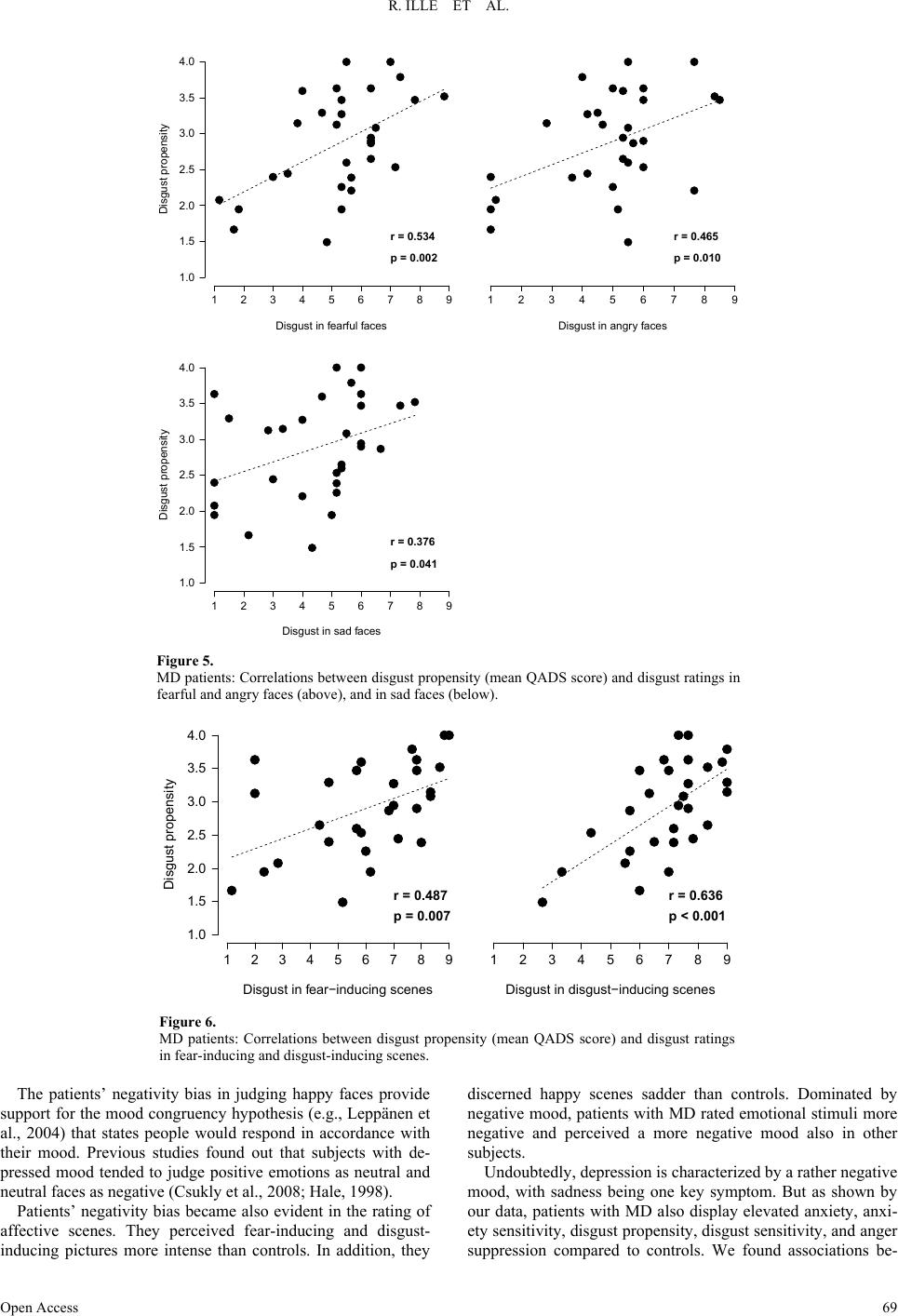 R. ILLE ET AL. Open Access 69 Disgust in fearful faces Disgust propensity 1.0 1.5 2.0 2.5 3.0 3.5 4.0 123456789 r = 0.534 p = 0.002 Disgust in angry faces 12345678 r = 0.465 p = 0.010 Disgust in sad faces Disgust propensity 1.0 1.5 2.0 2.5 3.0 3.5 4.0 123456789 r = 0.376 p = 0.041 Figure 5. MD patients: Correlations between disgust propensity (mean QADS score) and disgust ratings in fearful and angry faces (above), and in sad faces (below). Disgust in fear−inducing scenes Disgust propensity 1.0 1.5 2.0 2.5 3.0 3.5 4.0 123456789 r = 0.487 p = 0.007 Disgust in disgust−inducing scenes 123456789 r = 0.636 p < 0.001 Figure 6. MD patients: Correlations between disgust propensity (mean QADS score) and disgust ratings in fear-inducing and disgust-inducing scenes. The patients’ negativity bias in judging happy faces provide support for the mood congruency hypothesis (e.g., Leppänen et al., 2004) that states people would respond in accordance with their mood. Previous studies found out that subjects with de- pressed mood tended to judge positive emotions as neutral and neutral faces as negative (Csukly et al., 2008; Hale, 1998). Patients’ negativity bias became also evident in the rating of affective scenes. They perceived fear-inducing and disgust- inducing pictures more intense than controls. In addition, they discerned happy scenes sadder than controls. Dominated by negative mood, patients with MD rated emotional stimuli more negative and perceived a more negative mood also in other subjects. Undoubtedly, depression is characterized by a rather negative mood, with sadness being one key symptom. But as shown by our data, patients with MD also display elevated anxiety, anxi- ety sensitivity, disgust propensity, disgust sensitivity, and anger suppression compared to controls. We found associations be-  R. ILLE ET AL. Open Access 70 tween patients’ disgust propensity and disgust ratings of fearful, angry and sad faces pointing to a disgust bias in patients with elevated disgust proneness. Moreover, anger suppression was negatively related to patients’ happiness experience. These findings also coincide with the mood congruency effect. Our emotion recognition data are in accordance with Asthana et al. (1998) who found a general impairment of emotion de- coding performance in patients with MD. Comparable to our patient sample, patients in this study met the diagnostic criteria of DSM-IV for major depressive disorder that is associated with a general cognitive disorder. Patients of our study dis- played reduced cognitive performance compared to controls. Furthermore, we found a relationship between patients’ cogni- tive performance and identification accuracy of angry and dis- gusted facial expressions. These facial emotions are similar- looking and therefore are particularly difficult to discriminate. Patients rated higher intensities of disgust for angry faces than controls. Furthermore, severity of depressive symptoms was nega- tively correlated to experience of happiness in pleasure-induc- ing and neutral scenes. Depression severity was also positively associated to experience of sadness in fearful and neutral scenes. However, the degree of depressive symptoms had no effect on decoding accuracy of affective faces. Previous findings are contradictory. Milders et al. (2010) found no association be- tween accuracy performance of sad faces and BDI ratings. However, Hale (1998) reported a positive relationship between the judgment of negative emotions in the facial expressions and depression severity. We also found no association between depression severity and cognitive performance. It is possible that cognitive inter- ference is associated with major depression but does not sig- nificantly vary with its symptom severity. Patients’ elevated negative perception of emotion-inducing scenes and emotional facial expressions as well as their higher intensity ratings of neutral stimuli are contrary to suggestions of the ECI hypothesis. Rottenberg (2005) found that patients with the most pronounced ECI showed the most severe depression. Gender-specific differences of depressive symptoms, with males showing more anger compared to females (e.g., Rutz et al., 1997) were confirmed by our data. Males with MD reported higher trait anger, and they also rated happy faces more nega- tive than female patients. Although males and females with MD did not differ in depression score, this difference in judgment of happy faces may be the consequence of a more negative mood state in males suffering from depression. Items of depression inventories like the BDI do not sufficiently consider male de- pression symptoms like anger. We also could replicate the findings of previous studies that pointed a female advantage in decoding affective faces (e.g., Cellerino et al., 2004). Women in both groups displayed a better decoding of facial expressions than males. Therefore, compared to men, women with MD had an advantage by a less negative mood state and a more correct estimate of other subjects’ feelings. Results indicate that in depression treatment increased focus should put to the association between negative mood bias and social functioning. Especially in male depression this aspect may be underestimated. As a limitation of our study it must be stated that all patients were treated with antidepressants and/or antipsychotics. Tranter et al. (2009) could show that treatment of depressed patients with antidepressants resulted in improved recognition accuracy of disgusted, happy, and surprised facial expressions, being strongest for disgust. But it remains unclear, if this effect is directly associated with antidepressant treatment or a result of mood improvement. Therefore, antidepressant treatment could have resulted in a shift of our patients’ emotion decoding and experience. In conclusion, the present findings indicate that MD is char- acterized by a broad impairment of emotion recognition, con- cerning all negative facial emotions with exception of fear. Further on, patients’ responses to happy faces suggest a nega- tivity bias in perceiving other peoples’ facial expressions, which also became evident in the perception of emotional scenes. The negativity bias was stronger in male than female patients. Depression severity was negatively related to experi- ence of happiness, and positively associated to a sadness-bias in fear-eliciting and neutral scenes. Compared to controls MD patients showed a lower cognitive performance, which was associated with identification accuracy of angry and disgusted facial expressions. However, we found no association between depression severity and decoding accuracy of facial emotions and to patients’ cognitive performance. Thus, our findings on negativity bias show accordance with the mood-congruency hypothesis, suggesting facilitated processing of negative emo- tional cues and deficient processing of positive emotional stim- uli. By contrast, our outcomes are contrary to suggestions of the ECI hypothesis, supposing decreased reactivity to all emotion cues in individuals with depression, regardless of valence. Re- sults indicate that in depression treatment increased focus should put to the association between negative mood bias and social functioning. REFERENCES American Psychiatric Association (APA) (2000). Diagnostic and statis- tical manual of mental disorders (4th ed.).Washington DC: Author. Angst, J., Gamma, A., Gastpar, M., Lepine, J. P., Mendlewicz, J., & Tylee, A. (2002). Gender differences in depression. Epidemiological findings from the European DEPRES I and II studies. European Ar- chives of Psychiatry and Clinical Neuroscience, 25 2, 20-29. Asthana, H. S., Mandal, M. K., Khurana, H., & Haque-Nizamie, S. (1998). Visuospatial and affect recognition deficit in depression. Journal of Affective Disorders, 48, 57-62. http://dx.doi.org/10.1016/S0165-0327(97)00140-7 Bower, G. H. (1981). Mood and memory. American Psychologist, 36, 129-148. http://dx.doi.org/10.1037/0003-066X.36.2.129 Bylsma, L. M., Morris, B. H., & Rottenberg, J. (2008). A meta-analysis of emotional reactivity in major depressive disorder. Clinical Psy- chology Review, 28, 676-691. http://dx.doi.org/10.1016/j.cpr.2007.10.001 Cellerino, A., Borghetti, D., & Sartucci, F. (2004). Sex differences in face gender recognition in humans. Brain Research Bulletin, 63, 443- 449. http://dx.doi.org/10.1016/j.brainresbull.2004.03.010 Csukly, G., Czobor, P., Simon, L., & Takács, B. (2008). Basic emotions and psychological distress: Association between recognition of facial expressions and symptom checklist-90 subscales. Comprehensive Psy- chiatry, 49, 177-183. http://dx.doi.org/10.1016/j.comppsych.2007.09.001 Drevets, W. C. (2001). Neuroimaging and neuropathological studies of depression: Implications for the cognitive-emotional features of mood disorders. Current Opinion in Neurobiology, 11, 240-249. http://dx.doi.org/10.1016/S0959-4388(00)00203-8 Du, S., & Martinez, A. M. (2013). Wait, are you sad or angry? Large exposure time differences required for the categorization of facial expressions of emotion. Journal of Vision, 13, 1-14. http://dx.doi.org/10.1167/13.4.13 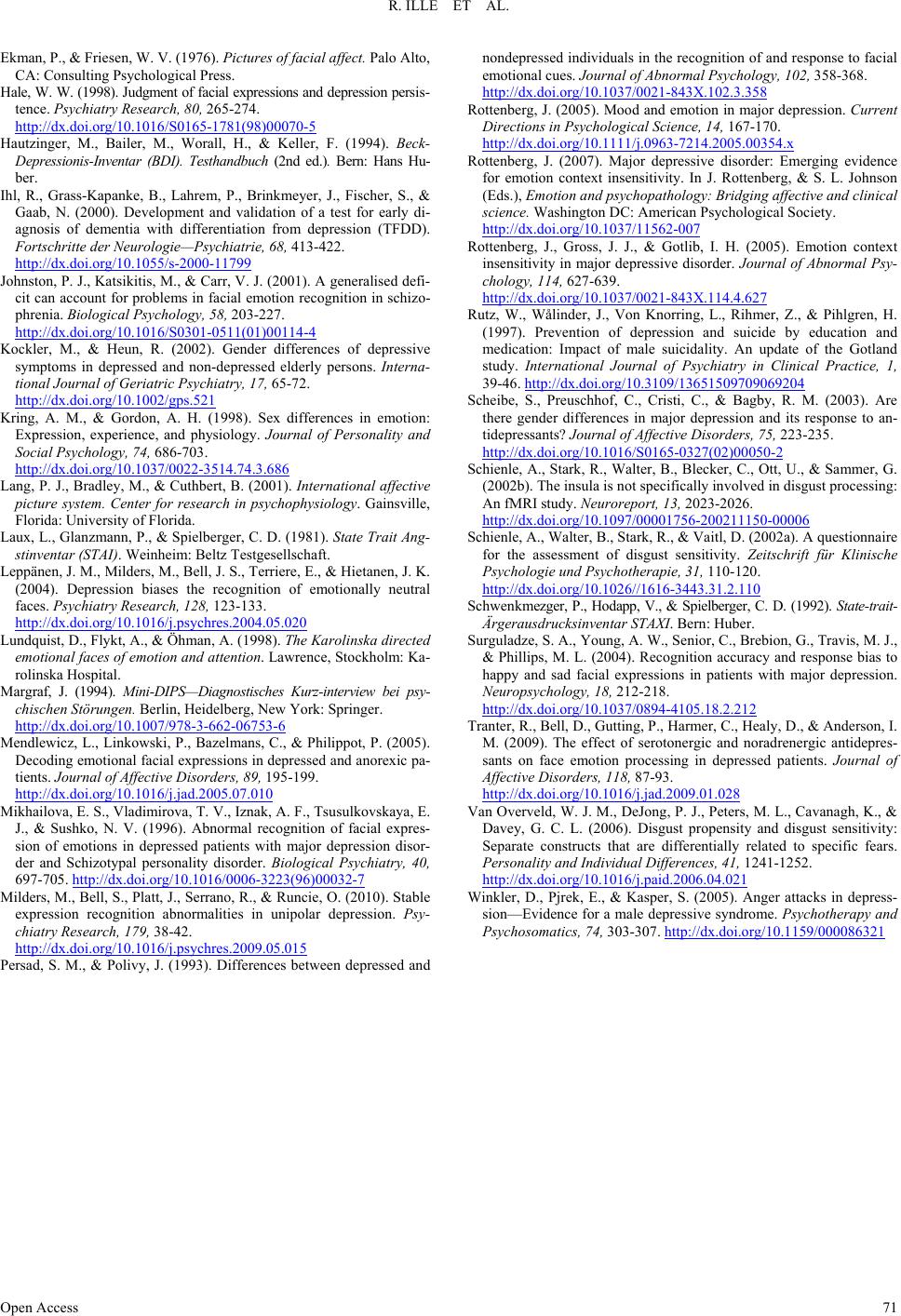 R. ILLE ET AL. Open Access 71 Ekman, P., & Friesen, W. V. (1976). Pictures of facial affect. Palo Alto, CA: Consulting Psychological Press. Hale, W. W. (1998). Judgment of facial expressions and depression persis- tence. Psychiatry Research, 80, 265-274. http://dx.doi.org/10.1016/S0165-1781(98)00070-5 Hautzinger, M., Bailer, M., Worall, H., & Keller, F. (1994). Beck- Depressionis-Inventar (BDI). Testhandbuch (2nd ed.). Bern: Hans Hu- ber. Ihl, R., Grass-Kapanke, B., Lahrem, P., Brinkmeyer, J., Fischer, S., & Gaab, N. (2000). Development and validation of a test for early di- agnosis of dementia with differentiation from depression (TFDD). Fortschritte der Neurologie—P sychiatrie, 68, 413-422. http://dx.doi.org/10.1055/s-2000-11799 Johnston, P. J., Katsikitis, M., & Carr, V. J. (2001). A generalised defi- cit can account for problems in facial emotion recognition in schizo- phrenia. Biological Psychology, 58, 203-227. http://dx.doi.org/10.1016/S0301-0511(01)00114-4 Kockler, M., & Heun, R. (2002). Gender differences of depressive symptoms in depressed and non-depressed elderly persons. Interna- tional Journal of Geriatric Psychiatry, 17 , 65-72. http://dx.doi.org/10.1002/gps.521 Kring, A. M., & Gordon, A. H. (1998). Sex differences in emotion: Expression, experience, and physiology. Journal of Personality and Social Psychology, 74, 686-703. http://dx.doi.org/10.1037/0022-3514.74.3.686 Lang, P. J., Bradley, M., & Cuthbert, B. (2001). International affective picture system. Center for research in psychophysiology. Gainsville, Florida: University of Florida. Laux, L., Glanzmann, P., & Spielberger, C. D. (1981). State Trait Ang- stinventar (STAI). Weinheim: Beltz Testgesellschaft. Leppänen, J. M., Milders, M., Bell, J. S., Terriere, E., & Hietanen, J. K. (2004). Depression biases the recognition of emotionally neutral faces. Psychiatry Research, 128, 123-133. http://dx.doi.org/10.1016/j.psychres.2004.05.020 Lundquist, D., Flykt, A., & Öhman, A. (1998). The Karolinska directed emotional faces of emotion and attention. Lawrence, Stockholm: Ka- rolinska Hospital. Margraf, J. (1994). Mini-DIPS—Diagnostisches Kurz-interview bei psy- chischen Störungen. Berlin, Heidelberg, New York: Springer. http://dx.doi.org/10.1007/978-3-662-06753-6 Mendlewicz, L., Linkowski, P., Bazelmans, C., & Philippot, P. (2005). Decoding emotional facial expressions in depressed and anorexic pa- tients. Journal of Affective Disorders, 89, 195-199. http://dx.doi.org/10.1016/j.jad.2005.07.010 Mikhailova, E. S., Vladimirova, T. V., Iznak, A. F., Tsusulkovskaya, E. J., & Sushko, N. V. (1996). Abnormal recognition of facial expres- sion of emotions in depressed patients with major depression disor- der and Schizotypal personality disorder. Biological Psychiatry, 40, 697-705. http://dx.doi.org/10.1016/0006-3223(96)00032-7 Milders, M., Bell, S., Platt, J., Serrano, R., & Runcie, O. (2010). Stable expression recognition abnormalities in unipolar depression. Psy- chiatry Research, 179, 38-42. http://dx.doi.org/10.1016/j.psychres.2009.05.015 Persad, S. M., & Polivy, J. (1993). Differences between depressed and nondepressed individuals in the recognition of and response to facial emotional cues. Journal of Abnormal Psychology, 102, 358-368. http://dx.doi.org/10.1037/0021-843X.102.3.358 Rottenberg, J. (2005). Mood and emotion in major depression. Current Directions in Psychological Science, 14, 167-170. http://dx.doi.org/10.1111/j.0963-7214.2005.00354.x Rottenberg, J. (2007). Major depressive disorder: Emerging evidence for emotion context insensitivity. In J. Rottenberg, & S. L. Johnson (Eds.), Emotion and psychopathology: Bridging affective and clinical science. Washington DC: American Psychological Society. http://dx.doi.org/10.1037/11562-007 Rottenberg, J., Gross, J. J., & Gotlib, I. H. (2005). Emotion context insensitivity in major depressive disorder. Journal of Abnormal Psy- chology, 114, 627-639. http://dx.doi.org/10.1037/0021-843X.114.4.627 Rutz, W., Wålinder, J., Von Knorring, L., Rihmer, Z., & Pihlgren, H. (1997). Prevention of depression and suicide by education and medication: Impact of male suicidality. An update of the Gotland study. International Journal of Psychiatry in Clinical Practice, 1, 39-46. http://dx.doi.org/10.3109/13651509709069204 Scheibe, S., Preuschhof, C., Cristi, C., & Bagby, R. M. (2003). Are there gender differences in major depression and its response to an- tidepressants? Journal of Affective Disorders, 75, 223-235. http://dx.doi.org/10.1016/S0165-0327(02)00050-2 Schienle, A., Stark, R., Walter, B., Blecker, C., Ott, U., & Sammer, G. (2002b). The insula is not specifically involved in disgust processing: An fMRI study. Neuroreport, 13, 2023-2026. http://dx.doi.org/10.1097/00001756-200211150-00006 Schienle, A., Walter, B., Stark, R., & Vaitl, D. (2002a). A questionnaire for the assessment of disgust sensitivity. Zeitschrift für Klinische Psychologie und Psychotherapie, 31, 110-120. http://dx.doi.org/10.1026//1616-3443.31.2.110 Schwenkmezger, P., Hodapp, V., & Spielberger, C. D. (1992). State-trait- Ärgerausdrucksinventar STAXI. Bern: Huber. Surguladze, S. A., Young, A. W., Senior, C., Brebion, G., Travis, M. J., & Phillips, M. L. (2004). Recognition accuracy and response bias to happy and sad facial expressions in patients with major depression. Neuropsychology, 18, 212-218. http://dx.doi.org/10.1037/0894-4105.18.2.212 Tranter, R., Bell, D., Gutting, P., Harmer, C., Healy, D., & Anderson, I. M. (2009). The effect of serotonergic and noradrenergic antidepres- sants on face emotion processing in depressed patients. Journal of Affective Disorders, 118, 87-93. http://dx.doi.org/10.1016/j.jad.2009.01.028 Van Overveld, W. J. M., DeJong, P. J., Peters, M. L., Cavanagh, K., & Davey, G. C. L. (2006). Disgust propensity and disgust sensitivity: Separate constructs that are differentially related to specific fears. Personality and Individual D i fferences, 41, 1241-1252. http://dx.doi.org/10.1016/j.paid.2006.04.021 Winkler, D., Pjrek, E., & Kasper, S. (2005). Anger attacks in depress- sion—Evidence for a male depressive syndrome. Psychotherapy and Psychosomatics, 74, 303-307. http://dx.doi.org/10.1159/000086321
|