Efferocytosis in Retinoblastoma
1446
Figure 11. (HE, ×400) Showing vesicles (efferosome) in dif-
ferent shapes and sizes noted in the RPE.
3. Discussion
Efferocytosis is derived from the Latin word “effere” for
“to bury”, and it is the process by which the dead cells
are removed by macrophage phagocytic cells [3-5]. Dur-
ing efferocytosis, the cell membranes of phagocytic cell
engulf the apoptotic cells forming a large fluid filled
vesicle containing the dead cells [3-6]. The ingested vesi-
cle is called efferosome and this process is similar to
macropinocytosis [3,4]. Documentation of efferocytosis
in retinal pigment epithelial cells in retinob lastoma speci-
men of human eye was shown for the first time in the
scientific literature. Apoptosis or programmed cell death
is orderly and genetically controlled form of cell death
which can be seen in the tumour or when chemotherapy
induces such change in the tumour mass [5,6]. In a mor-
phological logic, it differs from necrosis in which cellular
shrinkage and chromatin condensation occur, followed
by fragmentation of nuclear components and apoptotic
vesicle formation which are cleared by phagocytosis
without damaging the neighboring tissues [5,6,8]. We
had seen that in our case where nuclear fragmentation
and apoptotic vesicle arrangement and the macrophages
in the process engulfed the vesicular bodies, some of the
vesicles were also seen in the RPE where they were en-
gulfed by the macrophages and thus effective efferocyto-
sis was recognized. These have major pharmacodynamic
applications for the anticancer drugs. The first step of
any anticancer drug is the interaction of cellular target [5-
9]. As we have seen in our case, there were two groups
of cells in the tumour mass and the portion where it had
spread i.e. sclera. One group of cells was typical undif-
ferentiated retinoblastoma cells which were basophilic
nucleated cells with scanty cytoplasm and the other
group was the vesicular cells. So the targeted chemo-
therapy needs to focus on the vesicular apoptotic cells
which can have local effect and then they will be also
phagocytosed by the RPE cells. Thus, the effective drug
will be delivered in the tumour mass and then eliminated
out as efferosome during the process. In nutshell, cells
that undergo apoptosis form the second step where the
efficacy of anticancer drugs was mediated by those tar-
geted apoptotic vesicles. In larger study, the extent of
expression of various oncogenes such as P-53 [9], bcl-2,
bax, c-myc and others and exploring the endogenous
factors will benefit the understanding of cancer biology
of retinoblastoma. It is always a challenge for pharma-
cological research to explore apoptosis by modulating the
extrinsic and intrinsic regulators in a positive and nega-
tive direction in order to improve the efficacy of anti-
cancer treatment.
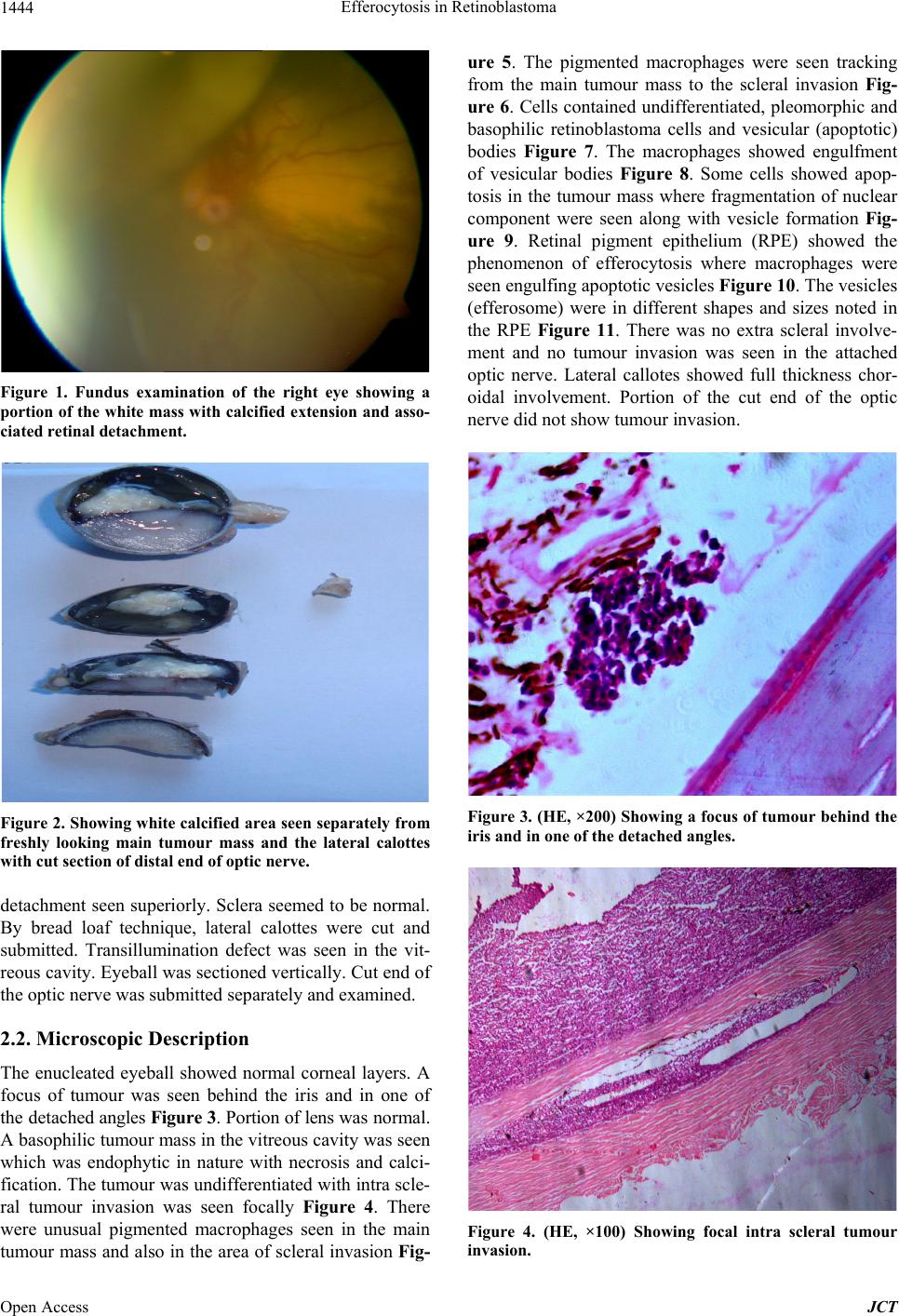
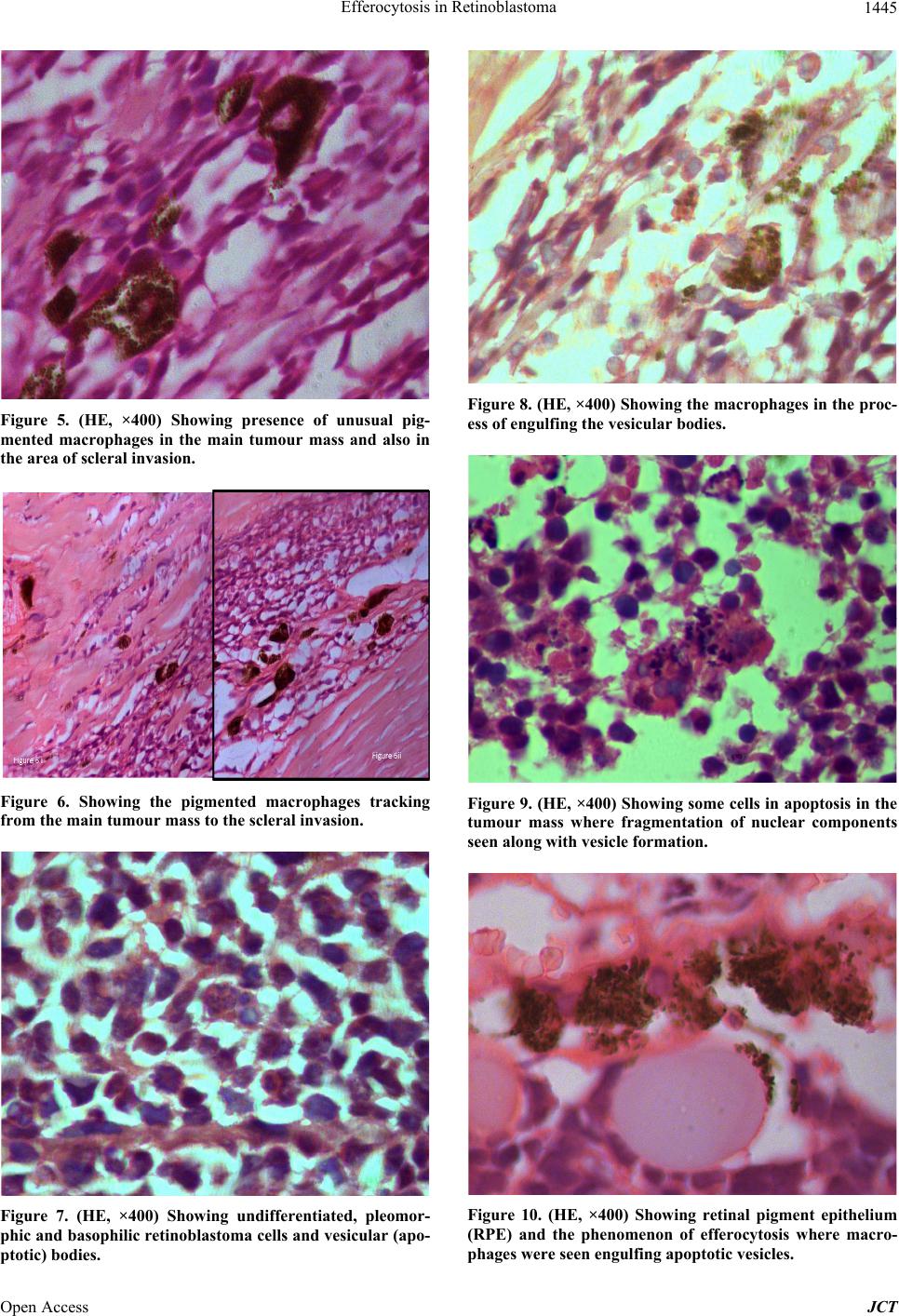
Our case was a 4-year-old boy with unilateral, undif-
ferentiated retinoblastoma. Clinical picture and gross
specimen showed two distinct zones of involvement. One
was calcified area and the other was a fresh active grey-
ish coloured mass with retinal detachment. We presumed
that patient might have small endophytic lesion earlier
which spontaneously regressed and later on, there was
recurrence. The biology of such mixed tumour with that
situation could also be explained even for the apoptotic
change. The patient had no history of previous chemo-
therapy. Tumour necrosis, calcification and obvious in-
tra-scleral spread might be due to the aggressive nature
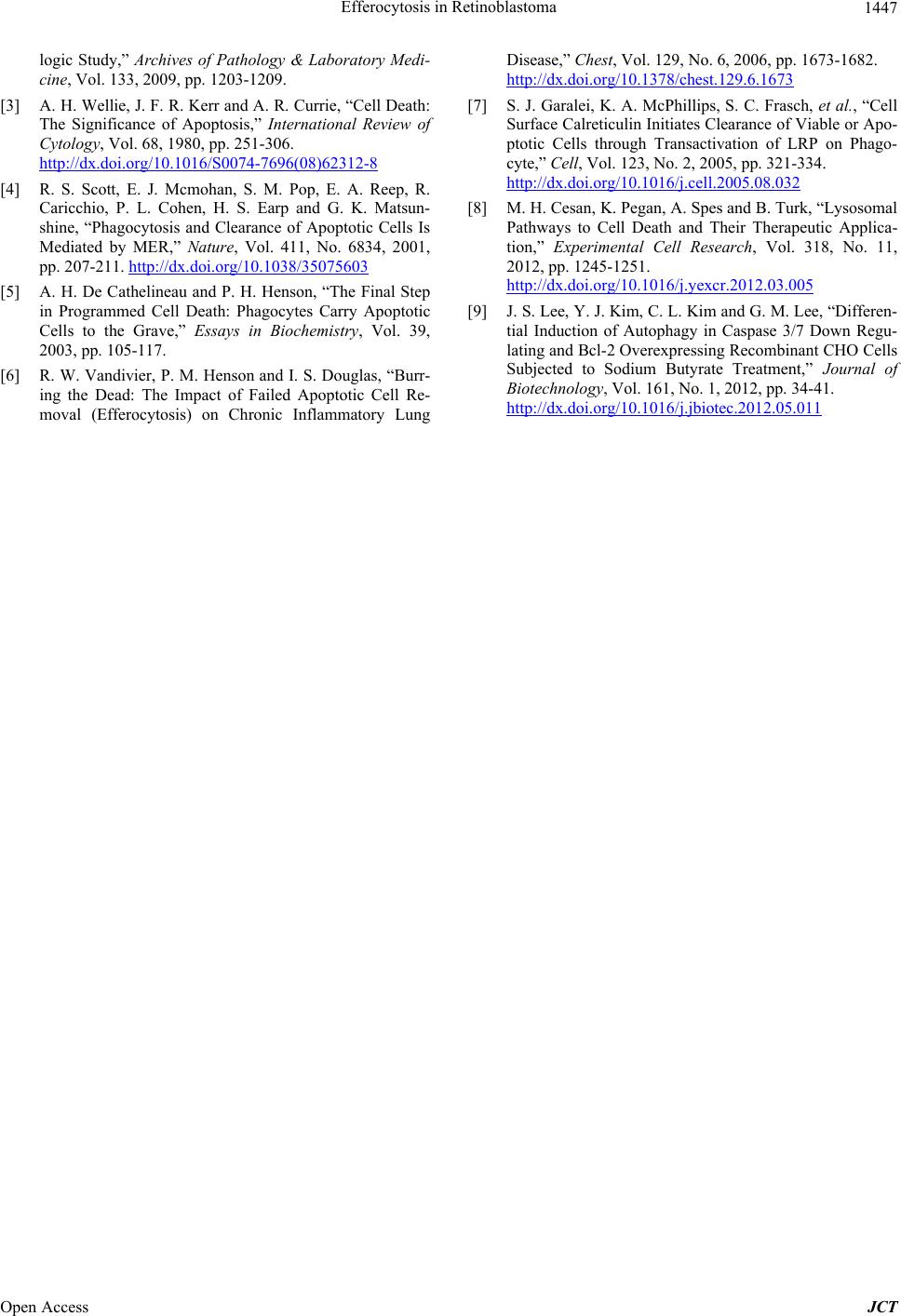
of recurrence. There was an interesting macrophagic
change seen in the sclera where the tumour was invaded.
Definite track of macrophagic migration was noted to the
sclera from the tumor mass. The pigmented macrophages
were larger from the normal pigmented cells seen in and
around that area of sclera and the tumour. Whether
macrophages traveled from the mass to the invaded tis-
sue before actual basophilic tumor cells migration or
macrophages really carried the tumour antibodies or pro-
teins to the distant areas in retinoblastoma will be the
subject of interest for the researcher in future.
4. Acknowledgements
The authors are indebted to: 1) Sri Kanchi Sankara
Health & Educational Foundation (SKSH&F); 2) Arjun
Mandal, Optometrist, Agartala, Tripura, India; 3) Mr.
Tarit Das, FM, Sri Sankaradeva Nethralaya, Guwahati,
Assam, India for their help and assistance.
REFERENCES
[1] C. L. Shields, A. Mashayekhi, H. Demirci, A. T. Mead-
ows and J. A. Shields, “Practical Approach to Manage-
ment of Retinoblastoma,” Archives of Ophthalmology,
Vol. 22, No. 5, 2004, pp. 729-735.
http://dx.doi.org/10.1001/archopht.122.5.729
[2] R. C. Eagle Jr., “High-Risk Features and Tumour Differ-
entiation in Retinoblastoma: A Retrospective Histopatho-
Open Access JCT