Evaluation of Conservative Treatment of Acute Fracture of the Odontoid Process of Axis with a Halo-Vest 299
5. Discussion
Surgical therapy is recommended for patients with a
fresh fracture of the odontoid process of the axis because
it allows for early discharge and successful rehabilitation.
However, surgery cannot always be conducted. If a pa-
tient has poor systemic conditions or does not desire sur-
gical therapy, and if there are problems with access to the
appropriate equipment, the only option is conservative
therapy. Therefore, the percentage of bone union in con-
servative therapy was evaluated in patients treated in our
hospital. The mean percentage of bone union of halo-
vest-fixed odontoid process fractures was 72.6% in
Anderson Type II patients [1,3-7]. Greene et al. [3]
showed that the percentage of bone union in 340 Ander-
son Type II patients treated with conservative therapy
was 79%. They also found that the percentage of bone
union of patients with a ≥6 mm fracture dislocation at the
time of injury was significantly different, consequently,
injury to the soft tissues was affected it. It was confirmed
that the percentage of bone union in Type III patients
was better than that of Type II patients [1,3,4,5,7] and the
mean percentage of bone union was 97.5% [1,3,4,5,7]
(Table 4). Therefore, an Anderson Type II patient with
≥6 mm fracture dislocation was considered to be a can-
didate for surgery in our hospital based on the results of
Greene et al. [3]. Patients in this study were Anderson
Type II with <6 mm and III fracture dislocations who
could not undergo surgery due to multiple trauma or did
not desire surgery. Bone union was observed in all of our
patients at 3 months after injury.
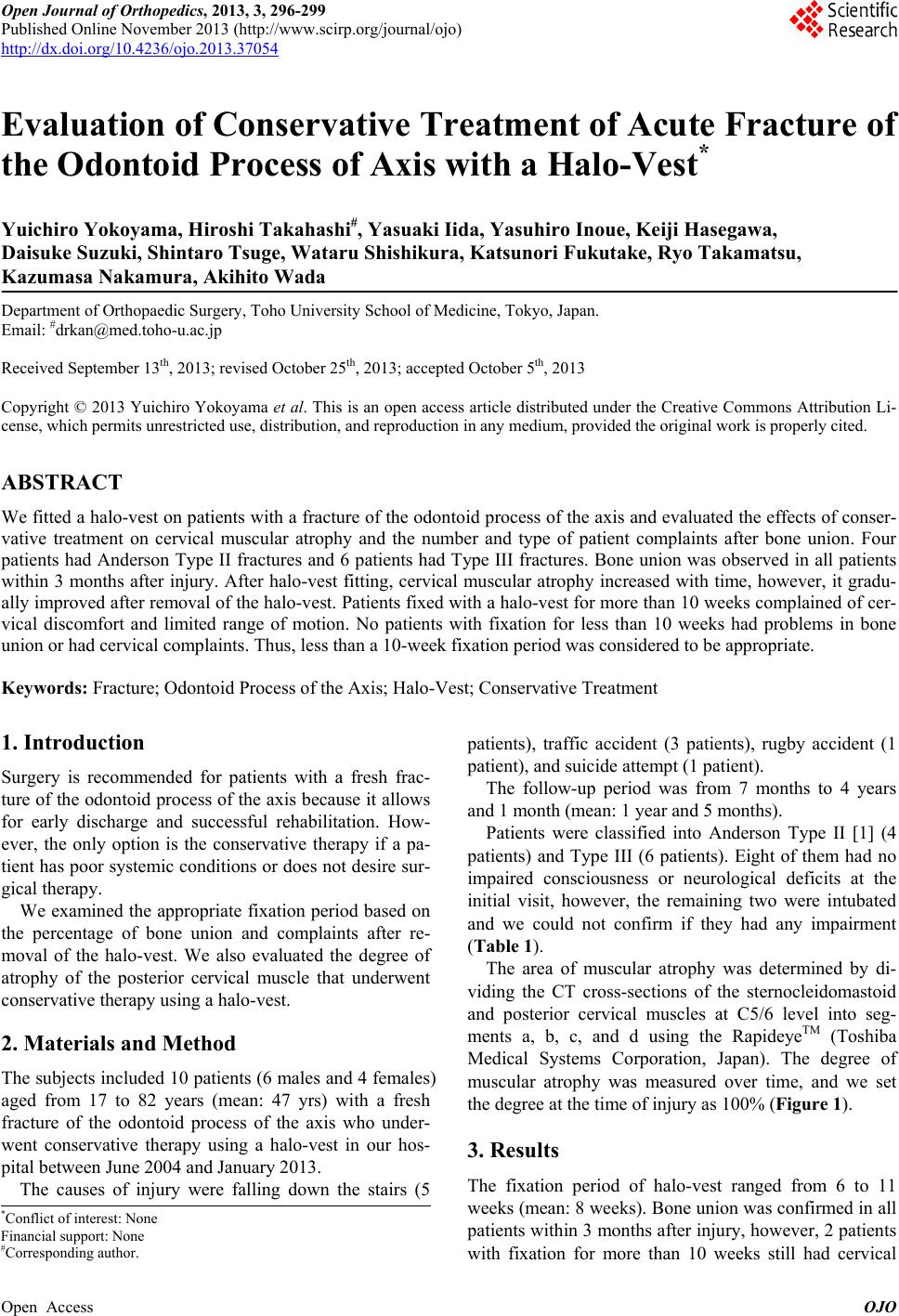
Muscular atrophy in the sternocleidomastoid and pos-
terior cervical muscles was evaluated based on the dura-
tion of the fixation period. Callus formation in radio-
graph and CT findings was detectable, however, it was
difficult to evaluate when the halo-vest was removed.
The longer the fixation is, the better the bone union ad-
vances. However, muscular atrophy occurs, possibly re-
sulting in cervical pain, stiff neck, cervical discomfort, or
limited range of motion in the cervical spine. Therefore,
muscular atrophy was measured over time. Ono et al. [8]
examined cervical muscular atrophy after halo-vest fit-
ting and showed that atrophy was observed in approxi-
mately 15% of the sternocleidomastoid muscles and in
22% of the posterior cervical muscles, and cervical dis-
comfort and limited range of motion were found when
atrophy was observed in more than 20% of the posterior
cervical muscles. Atrophy in the sternocleidomastoid and
posterior cervical muscles in this study was less than that
in Ono’s study because no patients were fixed with a
halo-vest for as long as 3 months. However, complaints,
including stiff neck and cervical discomfort in patients
with fixation for 10 weeks or more, were more frequent
than those in patients with cervical muscular atrophy for
less than 10 weeks.
Table 4. Bone union rates.
Fracture type Bone union
rates No. of cases
Odontoid process
fracture Anderson Type II 72.6% 386/531 cases
Type III 97.5 241/247
Based on these results, no patient with fixation for less
than 10 weeks had problems with bone union. Thus,
fixation with a halo-vest for less than 10 weeks is appro-
priate for a fresh fracture of the odontoid process of the
axis since cervical muscular atrophy and complaints as-
sociated with muscular atrophy are caused by long-term
fixation.
6. Conclusion
Halo-vest is useful for treatment of a fresh fracture of the
odontoid process in patients who cannot have surgery,
and the appropriate fixation period should be less than 10
weeks.
REFERENCES
[1] L. D. Anderson and R. T. D’Alonzo, “Fracture of the
Odontoid Process of the Axis,” The Journal of Bone &
Joint Surgery, Vol. 56, No. 8, 1974, pp. 1663-1674.
[2] A. M. Levine and C. C. Edwards, “The Management of
Traumatic Spondylolisthesis of the Axis,” The Journal of
Bone & Joint Surgery, Vol. 67, No. 2, 1985, pp. 217-226.
[3] K. A. Greene, C. A. Dickman, F. F. Marciano, J. B.
Drabier, M. N. Hadley and V. K. Sonntag, “Acute Axis
Fractures. Analysis of Management and Outcome in 340
Consecutive Cases,” Spine, Vol. 22, 1997, pp. 1843-1852.
http://dx.doi.org/10.1097/00007632-199708150-00009
[4] M. N. Hadley, C. Browner and V. K. Sonntag, “Axis
Fractures: A Comprehensive Review of Management and
Treatment in 107 Cases,” Neurosurgery, Vol. 17, 1985,
pp. 281-290.
http://dx.doi.org/10.1227/00006123-198508000-00006
[5] P. J. Lennarson, H. Mostafavi, V. C. Traynelis and B. C.
Walters, “Management of type Ⅱ Dens Fractures: A Case-
Control Study,” Spine, Vol. 25, No. 10, 2000, pp. 1234-
1237.
[6] E. A. Seybold and J. C. Bayley, “Functional Outcome of
Surgically and Conservatively Managed Dens Fractures,”
Spine, Vol. 23, No. 17, 1998, pp. 1837-1846.
http://dx.doi.org/10.1097/00007632-199809010-00006
[7] U. Vieweg and R. Schultheiss, “A Review of Halo Vest
Treatment of Upper Cervical Spine Injuries,” Archives of
Orthopaedic and Trauma Surgery, Vol. 125, 2001, pp.
50-55. http://dx.doi.org/10.1007/s004020000182
[8] A. Ono, M. Amano, Y. Okamura, T. Numazawa, K.
Ueyama, S. Nishizawa and S. Toh, “Muscle Atrophy after
Treatment with Halovest,” Spine, Vol. 30, 2005, pp. E8-
12.
Open Access OJO