Intraoperative vs 24-Hour Administration of Cefamandole to Prevent Deep Sternal Wound Infection
and Endocarditis after Adult Cardiac Surgery
384
2. Methods
During a 16-month period, we retrospectively studied all
consecutive adults (>18 years of age) who underwent
cardiac surgery with cardiopulmonary bypass (CPB): pe-
riod 1: 01/01/2008 to 31/08/2008 and period 2: 01/09/
2008 to 30/04/2009. No included in this study were pa-
tients with ß-lactam allergy, acute endocarditis and/or
vascular surgery with CPB. Our institution is private with
more than 200 beds dedicated exclusively to medical and
surgical cardiovascular and thoracic pathologies and where
700 - 850 interventions are performed annually.
The following parameters were extracted from the lo-
cal database which is registred at the French National
Commission Informatics and Liberty: sex, age, body
mass index, cardiovascular risk factors (diabetes, current
smoker, hypercholesterolemia, hypertension), presence
of chronic obstructive pulmonary disease (COPD), chro-
nic renal insufficiency (creatinemia ≥200 µmol/L), pe-
ripheral vascular disease, type of cardiac surgery [coro-
nary artery bypass graft (CABG) ± valve replacement
(VR), VR and other], use of 1 or 2 internal thoracic arter-
ies, Euroscore I [5], duration of ICU length of stay, pro-
longed mechanical ventilation (≥48 hours), use of nonin-
vasive ventilation, red-cell transfusion, vasopressor use,
rate of acute renal insufficiency (defined as a 2-fold in-
crease of the preoperative creatinemia), dialysis required.
In our institution, anesthesiologists and intensivists are
responsible for antibiotic-prophylaxis prescription, intra-
operatively and post-operatively, respectively. Each pre-
scriber received the written local protocol recommenda-
tion before the switch to the shorter regimen in August
2008. This local protocol, validated by our local Noso-
comial Infection-Control Committee, recommends the
use of cefamandole as the first-line antibiotic in the ab-
sence of ß-lactam allergy. In the operating room, infusion
of 1.5 g of cefamandole within the 1 hour preceding the
incision is recommended. It is also specified that another
infusion 750 mg of cefamandole is mandatory when the
surgery lasts ≥120 minutes, with repeated infusions every
120 minutes, as needed. Lastly, for period 1, 750 mg of
cefamandole were infused every 6 hours during the first
24 postoperative hours during the intensive care unit
stay.
The Centers for Disease Control definitions were used
to for DSWI and endocarditis [6]. Occurrence of those
infections was recorded and validated independently by
our local Nosocomial Infection-Control Committee. For
each infection, we studied the date of its diagnosis, the
interval between surgery and infection, the pathogen(s)
involved, their susceptibilities to antibiotics and the de-
velopment of concomitant bacteriemia. All patients with
healing problems, suspected wound infection or sus-
pected postoperative endocarditis were systematically re-
addressed to their surgeon postoperatively.
There were no changes in measures to prevent infec-
tion between the study periods. Skin preparation was
performed as follow: the night before surgery, patients
took two showers with an antiseptic solution. The day of
surgery, 2 hours before surgery, patients took a third
shower with an antiseptic solution and hair was removed.
No specific outbreaks occurred during the study period.
The concerned database had been approved by the
French national commission for computerized files and
liberty. According to French law, its subsequent use for
epidemiologic work does not require additional regula-
tory or ethic commission approval.
Statistical Analysis
Continuous variables are presented as median with range
and categorical variables as n (%). Comparisons were
made using the chi-square or Fisher’s exact test (when
needed) to analyze differences in categorical variables.
The Student’s t-test or the Mann-Witney test was used,
as appropriate, for continuous variables. A p value < 0.05
was considered statistically significant. Statistical analy-
ses were performed using Statview version 5.1 software
(SAS Institute Inc., Cary, NC).
3. Results
During the study, 987 adults [499 (50.5%) during period
1 and 488 (49.5%) during period 2] had heart surgery
with CPB in our institution. Fifty-four patients were not
included, 29 from period 1 and 25 from period 2, because
of ß-lactam allergy, acute endocarditis and/or vascular
surgery with CPB. Thus, 933 patients were included in
the study: 470 during period 1 and 463 during period 2.
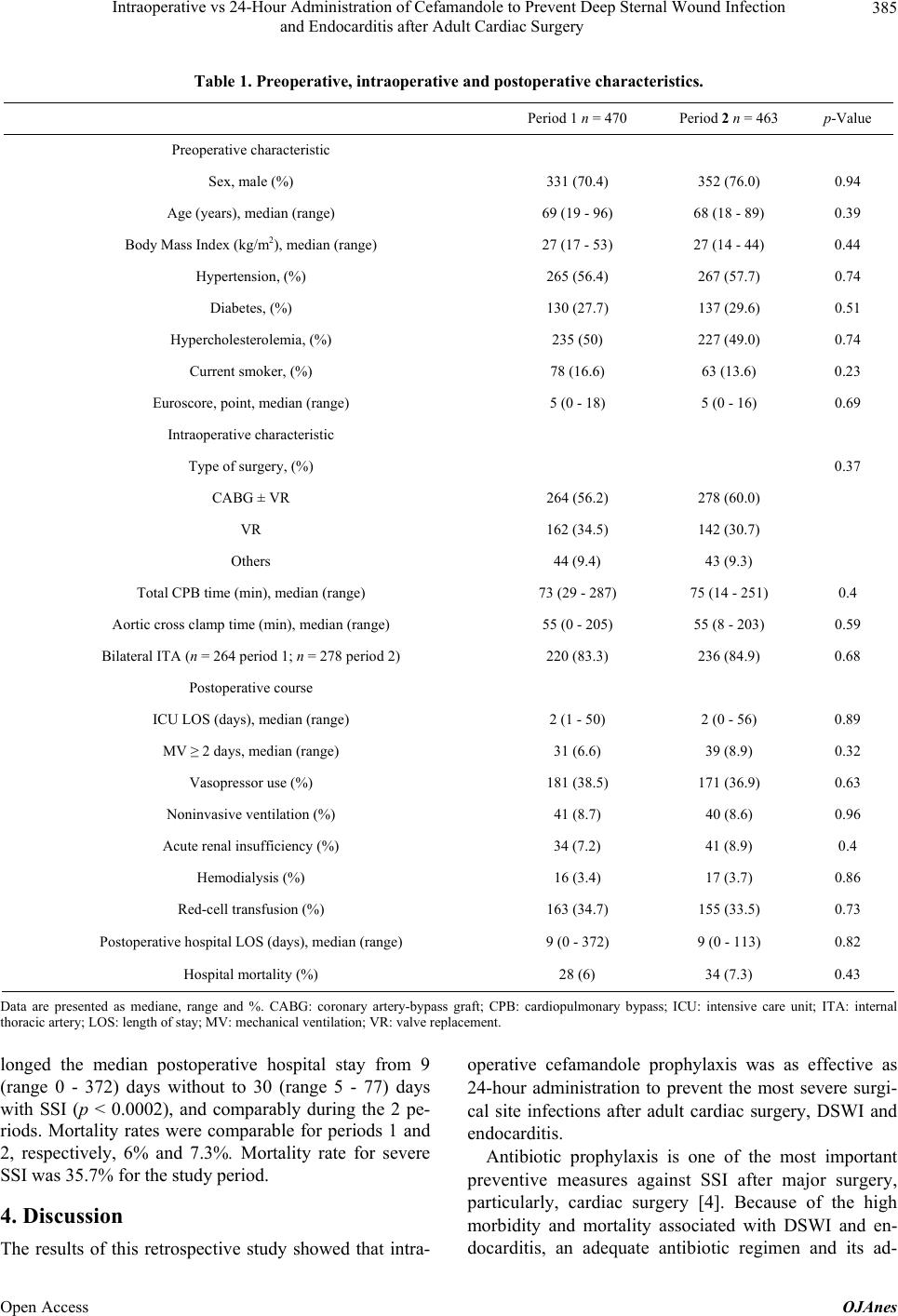
Detailed preoperative, intraoperative and postoperative
patient characteristics, categorized according to the anti-
biotic regimen used during those periods, are given in
Table 1. The 2 groups were homogeneous and compara-
ble for their demographic profiles and clinical character-
istics. The 3 surgeons’ activities were comparable during
the 2 periods (data not shown).
During the study, 14 (1.5%) SSI were diagnosed: 1.3%
(n = 6) during period 1 vs 1.7% (n = 8) during for period
2. SSI characteristics were comparable concerning the
median time to infection onset 28 days (range, 5 - 129
days) vs. 23 days (range, 4 - 112 days). Eleven (5 in pe-
riod 1 and 6 in period 2) bacteriemia were diagnosed
with SSI. Of 17 pathogens isolated, 12 (70.5%) were
Gram-positive cocci and 5 (20.9%) Gram-negative bacilli.
They were similarly distributed in the 2 periods.
Median postoperative hospital stay was comparable
during periods: 1 and 2, respectively: 9 (range 0 - 372) vs
9 (range 0 - 113) days. SSI occurrence significantly pro-
Open Access OJAnes