 World Journal of Cardiovascular Diseases, 2013, 3, 499-505 WJCD http://dx.doi.org/10.4236/wjcd.2013.38079 Published Online November 2013 (http://www.scirp.org/journal/wjcd/) Hyperhomoysteinemia as a risk factor for coronary heart diseases in chronic hepatitis C patients Ali Raza Kazmi1, Andleeb Hanif1,2, Muhammad Ismail1, Javaria Qazi2 1Institute of Biomedical and Genetic Engineering, Islamabad, Pakistan 2Department of Biotechnology, Quaid-i-Azam University, Islamabad, Pakistan Email: drsakazmi@gmail.com Received 20 August 2013; revised 28 September 2013; accepted 15 October 2013 Copyright © 2013 Ali Raza Kazmi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Hepatitis C virus is one of the major health problems worldwide. It affects mainly the liver but several ex- trahepatic manifestations are also accounted. Chronic hepatitis C patients are at an increased risk of devel- oping hepatic steatosis, which share many clinical fea- tures with the metabolic syndrome. Hepatic steatosis has also been associated with elevated levels of mark- ers of inflammation such as homocysteine, identified as hyperhomocysteinemia (HHC). HHC due to Me- thylenetetrahydrofolate Reductase (MTHFR) gene, in particular the C677T polymorphism, was recently as- sociated with coronary heart diseases (CHD) in chro- nic hepatitis C (CHC) patients. Homocysteine is an intermediate in methionine metabolism, which takes place mainly in the liver metabolism. Deficiencies of micronutrients (folate, vitamin B 6 and possibly vita- min B 12) along with mild hyperhomocysteinemia, perhaps, act synergistically with other classical risk factors to further increase the risk of CHD. Clinical data indicate that HHC is associated with an increa- sed incidence of CHD as well as with the severity of the disease in CHC patients. In conclusion, HHC might be a potential aetiological factor of CHD in CHC patients. The aim of this review is to investigate the progression of coronary heart diseases in chronic hepatitis C patients and correlate with levels of homo- cysteine in concurrence to genetic defects and nutri- ent deficiencies. However, future studies need to clari- fy the mechanistic role of HHC in CHD and CHC as a useful paradigm with most interesting therapeutic im- plications. Keywords: Hepatitis C Virus; Hyperhomocysteinemia (HHC); Coronary Heart Diseases (CHD); Chronic Hepatitis C (CHC) 1. INTRODUCTION Chronic infection with hepatitis C virus (HCV) is one of the leading causes of chronic liver disease; about 170 million people worldwide are estimated to be infected. Hepatitis C virus infection causes acute symptoms in only 15% of patients exposed to HCV infection while about 80% patients develop chronic infection [1]. Chro- nic hepatitis C results in formation of high levels of free radicals in the liver cells, which put serious oxidative stress depleting protective antioxidants and eventually kill the liver cells. A hepatitis screen is recommended for patients whereby the disease can be diagnosed by the presence of antibodies for hepatitis C or by the direct presence of the virus or viral products in the blood [2]. 2. ASSOCIATED RISKS: CHRONIC HEPATITIS C Hepatitis C virus (HCV) infection is a major cause of chronic liver disease. HCV infection frequently does not resolve, leading to chronic hepatitis with increasing risk of developing hepatic fibrosis, steatosis, liver cirrhosis, hepatocellular carcinoma, metabolic syndromes, arthro- sclerosis and extrahepatic diseases [3]. The combination of pegylated interferon (IFN)-a and ribavirin is the only treatment for chronic HCV infections with proven effi- cacy. Unfortunately, this therapeutic strategy results in a low sustained virologic response (SVR), defined as an ab- sence of detectable serum HCV-RNA at six months after completion of antiviral therapy; SVR is achieved in less than 50% of treated patients that have HCV genotype 1 and a high viral load [4]. There is evidence indicating that SVR is associated with long-term clearance of HCV infection and lower HCV-related complications [5,6]. However, IFN-a in combination with ribavirin is gene- rally not well tolerated, and the adverse side effects may OPEN ACCESS  A. R. Kazmi et al. / World Journal of Cardiovascular Diseases 3 (2013) 499-505 500 lead to interruption or cessation of therapy. The major adverse effects are anemia, fatigue, hair loss, depression, insomnia, vertigo, anorexia, nausea, nasal congestion, cough, dyspnea, pruritus, and growth delay [7]. 3. HEPATITIS C VIRUS AND CARDIAC RISK Chronic hepatitis C virus (CH-C) infection is associated with metabolic conditions such as insulin resistance and type 2 diabetes (T2DM) and may increase the risk of coronary heart diseases. Coronary artery disease is the most common heart disease with multifactorial etiology. Atherosclerosis being the principal cause has plagued human kind since ancient times. Its understanding has much evolved over centuries, traditionally being viewed as degenerative disease, is now considered a dynamic in- flammatory and fibroproliferative process, triggered by cytokines and growth factors [8-12]. In addition to other conventional atherogenic risk factors (Age, Sex, Smok- ing, Hypertension, Diabetes Mellitus and Dyslipidaemia), one of the most interesting development in the recent years has been the idea that infective agents may induce a pro-inflammatory state and have a crucial role in athe- rothrombosis [12-14]. 4. INADEQUATE VITAMINS AND HCV Patients with chronic HCV infection have significantly lowered plasma vitamin B1, B2, B6, C, and folic acid levels [15]. These patients were also observed to have significantly higher plasma homocysteine (a sulfur-con- taining amino acid, which is influenced by vitamin B2, 6, 12, and folic acid) concentrations and lower concentra- tions of folic acid and vitamin B12 [16]. The plasma ho- mocysteine levels were inversely correlated with the con- centrations of folic acid in HCV-infected patients. SVR patients have been observed to have lower plasma homo- cysteine levels than non-SVR patients [17]. Pre-treat- ment with IFN-a and ribavirin in chronic HCV-infected patients, serum vitamin B12 levels are positively corre- lated to end-of-treatment response [18]. Several infectious etiologies for coronary heart dis- eases (CHD) have been proposed in recent years on the basis of epidemiological associations, but there is no consensus regarding a causative role [19-21]. The asso- ciation between hepatitis C virus (HCV) infection and CHD is less clear. A small number of reported studies have shown conflicting results; some have reported no association between HCV infection and CHD [22-25], whereas others have reported an increased risk [26] or an increase in measures of subclinical atherosclerosis (e.g., carotid intima-media thickness) [26-28]. Many of the studies showing no association between HCV infection and CHD used a case-control design in which subjects with known CHD were compared with control subjects without CHD and the prevalence of HCV infection was compared between the 2 groups without adjustment for all Coronary artery diseases (CAD) risk factors. However, Persons with HCV infection are at an increased risk of developing hepatic steatosis, which shares many clinical features with the metabolic syndrome [29,30]. Hepatic steatosis has also been associated with elevated levels of markers of inflammation and endothelial dysfunction [31]. Hepatitis C virus increases the risk of coronary ar- tery disease, a large American study published in the Cli- nical Infectious Diseases [32]. These factors suggest a biologically plausible mechanism of increased risk of CHD in at least a subset of HCV-infected persons. The main rationale of this review is shown in Figure 1. 5. HOMOCYSTEINE METABOLISM Homocysteine (Hcy) belongs to a group of molecules known as cellular thiols. It is considered a “bad thiol” because its association with a variety of health conditions including cardiovascular disease, [33] end-stage renal di- sease, [34] neural tube defects, [35]. Recently, homo- cysteine has also been implicated in the pathogenesis of alcoholic liver injury [36]. The 5,10-methylenetetrahydrofolate reductase (MTHFR) is a key enzyme in the folate cycle and contributes to the metabolism of the amino-acid homocysteine. It irreversi- bly catalyzes the reduction of 5,10-methylene-tetrahy- drofolate to 5-methyltetrahydrofolate, the major circula- tory form of folate in the body and a carbon donor for conversion of homocysteine to methionine, precursor of S-adenosyl-L-methionine [37]. 6. HOMOCYSTEINE AND CHRONIC HEPATITIS C Homocysteine levels are also altered in chronic liver di- sease. Homocysteine is a sulphur containing amino acid belonging to the group of intracellular thiols. Numerous Figure 1. Rationale of study. Copyright © 2013 SciRes. OPEN ACCESS  A. R. Kazmi et al. / World Journal of Cardiovascular Diseases 3 (2013) 499-505 501 clinical and epidemiological studies have reported that elevated plasma homocysteine concentrations reflect im- paired cellular metabolism [38] and may be considered as an independent risk factor for atherosclerotic vascular disease and thromboembolism [39]. Experimental data in transgenic mice deficient in homocysteine metabolism enzymes have shown the presence of severe liver steato- sis with occasional steatohepatitis. In human beings, many studies have found a correlation between homocysteine and steatosis [40] Homocysteine is mainly synthesized and metabolized in the liver, since metabolism of majority of dietary me- thionine occurs in this organ, where about 85% of the whole body capacity for transmethylation resides. There- fore, genes involved in methionine and homocysteine metabolism are expressed in a specific pattern in the liver [41]. Homocysteine is formed as an intermediate in me- thionine metabolism; therefore, impaired liver function leads to altered methionine and homocysteine metabo- lism [42]. Plasma homocysteine levels were significantly elevated in HCV infected patients in both sexes com- pared with control values. These findings are in accor- dance with the results of many studies observed elevated plasma homocysteine levels in patients with liver cirrho- sis secondary to hepatitis C virus infection [38]. Some of the studies have attributed this condition to reduced ex- pression of genes involved in Hcy metabolism. The de- gree of reduced expression of these genes was related to the severity of liver disease [40]. Alterations in Hcy metabolism in human liver cirrho- sis can be ascribed in part to a marked reduction in the expression of the main genes involved in its metabolism, namely methionine synthase (MS) and betaine-homo- cysteine methyltransferase (BHMT), which convert ho- mocysteine back to methionine, and cystathionine-syn- thase (CBS), the first enzyme in the transsulfuration pathway[41]. The expression of these genes was always more compromised than that of HSA and was related to the severity of the disease, expressed as the Child-Pugh score. We observe reduced expression of Hcymetaboliz- ing genes, both in alcoholism and hepatitis C virus cir- rhosis. It has been suggested that impairment of Hcy metabolism in cirrhosis most possibly can be also related to decreased availability or utilization of vitamins B6, B12, or folates, [43]. 7. HYPERHOMOCYSTEINEMIA Elevated levels of homocysteine, Hyperhomocysteinemia (HHC), may result from defects in homocysteine-me- tabolizing genes; (such as MTHFR, Methylene tetrahy- drofolate Reductase gene) vitamin B6, B12, or folate de- ficiencies resulting from nutritional conditions; or chro- nic alcohol consumption [40]. The hyperhomocysteine- mia is known as atherogenic and thrombotic risk factor for cardiovascular disease. It might also be a risk factor for cirrhotic patients but the direct effect of Hcy on liver injury is not well known [44]. Hyperhomosysteinemia was correlated with elevated levels of ALT, ALP, TGs and cholesterol. This might be related to progression of liver injury. Some other studies have also reported a correlated elevation of plasma Hcy levels with ALT, ALP, TGs and cholesterol [45,46]. It is evident that homocysteine-induced endoplasmic reticu- lum stress leaves a dysregulated endogenous sterol re- sponse pathway, which leads to increased hepatic bio- synthesis and uptake of cholesterol and triglycerides [47]. 8. GENETIC DEFECTS IN HOMOCYSTEIN METABOLISM Elevations in plasma homocyst(e)ine are typically caused either by genetic defects in the enzymes involved in ho- mocysteine metabolism or by nutritional deficiencies in vitamin cofactors. Homocystinuria and severe hyperho- mocyst(e)inemia are caused by rare inborn errors of me- tabolism resulting in marked elevations of plasma and urine homocyst(e)ine concentrations. Cystathionine b- synthase deficiency is the most common genetic cause of severe hyperhomocyst(e)inemia. The homozygous form of this disease—congenital homocystinuria—can be as- sociated with plasma homocyst(e)ine concentrations of up to 400 mmol per liter during fasting [48]. The homo- zygous trait is rare (occurring in 1 in 200,000 births), and clinical manifestations include ectopialentis, skeletal de- formities, mental retardation, thromboembolism, and se- vere, premature atherosclerosis [49]. Atherothrombotic complications frequently develop in young adulthood in homozygotes and are often fatal, as first shown in a study by Carey and colleagues as early as 1968 [49]. Mudd and colleagues [50] have estimated that approximately 50 percent of untreated patients with homocystinuria will have a thromboembolic event before the age of 30 and that overall, the disease-related mortality is approxima- tely 20 percent. Heterozygotes typically have much less marked hy- perhomocyst(e)inemia, with plasma homocyst(e)ine con- centrations in the range of 20 to 40 mmol per liter, ap- proximately two to four times greater than the normal concentration of homocyst(e)ine in plasma [49,51-53]. A homozygous deficiency of N5, N10-methylenetetra hy- drofolatereductase, the enzyme involved in the vitamin B12-dependent remethylation of homocysteine to me- thionine, may also lead to severe hyperhomocyst(e)ine- mia [54]. Patients with this type of deficiency tend to have a worse prognosis than those with cystathionine b-synthase deficiency, in part because of the complete lack of effective therapy [55,56]. In addition, studies (Kang and colleagues) [57] have reported a thermolabile Copyright © 2013 SciRes. OPEN ACCESS  A. R. Kazmi et al. / World Journal of Cardiovascular Diseases 3 (2013) 499-505 502 variant of N5, N10-methylene-tetrahydrofolate reductase that is caused by a point mutation (MTHFR_C677T) in the coding region for the N 5, N 10-methylene-tetrahy- drofolate binding site, leading to the substitution of va- line for alanine [58]. 9. MTHFR: C→T POLYMORPHISM A single nucleotide polymorphism (SNP) in the MTHFR gene, which is located in the chromosome 1p36.3, has been identified. A C-to-T transition at the nucleotide 677 (C677T) in exon four results in an alanine to valine ex- change which affects the catalytic domain of the enzyme; as a consequence, a thermo-labile variant of MTHFR, called t-MTHFR, is synthesized, which possesses redu- ced enzyme activity [59]. One of the most common mutations, or polymor- phisms, that are associated with a mild increase in plasma homocysteine (hyperhomocysteinemia) is the 677C→T substitution (an alanine to valine change) in the enzyme methylenetetrahydrofolate reductase (MTHFR). The MTHFR is an enzyme of the folate metabolism that reduces 5,10-metilenetetraidrofolate (5,10-mTHFR) to 5-metiltetraidrofolate (5-mTHF), an important co-factor to homocysteine (Hcy) methylation. Mutations in MTHFR gene like C677T result in amino acids substitutions that lead to a decreased enzyme activity [60,61]. As a conse- quence of the MTHFR dysfunctions, an increased Hcy level in plasma has been expected which, in turn, produ- ces a cytotoxic effect [62]. 10. CONCLUSION Hepatitis C virus infection is a major cause of progres- sive liver damage whose long term sequelae includes cir- rhosis and primary hepatocellular carcinoma. HCV main- ly affects the liver, but several tissues outside the liver have been reported to be involved, resulting in a wide spectrum of extrahepatic manifestations. Despite having fewer risk factors for cardiovascular disease, the hepatitis C-infected individuals were more likely to have been diagnosed with coronary artery disease. Multiple pro- spective and case-control studies have shown that a moderately elevated plasma homocysteine concentration is an independent risk factor for atherothrombotic vascu- lar disease. Homocysteine concentrations are consistent- ly higher in patients with peripheral, cerebrovascular, and coronary artery disease than in those without such disea- ses. Homocyst(e)ine promotes atherothrombogenesis by a variety of mechanisms; however, it is not yet clear whether homocysteine itself or a related metabolite or cofactor is primarily responsible for the atherothrombo- genic effects of hyperhomocyst (e)inemia in vivo. How- ever, it is biologically plausible that hepatitis C may in- crease the risk of disease such as heart attack and stoke as hepatitis steatosis (fatty liver), a common complica- tion of hepatitis C infection, has been associated with in- creased levels of homocysteine and metabolic syndrome. Though, the reason(s) and mechanism(s) of this associa- tion need further study.” 11. ACKNOWLEDGEMENTS We are thankful to the head of Department of Biotechnology, Quaid-i- Azam University, Islamabad, Pakistan for support. REFERENCES [1] National Institutes of Health Consensus Development Conference Panel statement Management of hepatitis C. (1997) Hepatology, 26, 2S-10S. [2] Wilkins, T., Malcolm, J.K., Raina, D., Schade, R.R. Hepatitis, C: Diagnosis and treatment. (2010) American Family Physician, 81, 1351-1357. [3] Choi, J., Ou, J.H.J. (2006) Mechanisms of liver injury. III. Oxidative stress in the pathogenesis of hepatitis C virus. American Journal of Physiology—Gastrointestinal & Liver Physiology, 290, G847-G851. http://dx.doi.org/10.1152/ajpgi.00522.2005 [4] Ghany, M.G., Strader, D.B., Thomas, D.L., Seeff, L.B. (2009) Diagnosis, management, and treatment of hepatitis C: An update. Hepatology, 49, 1335-1374. http://dx.doi.org/10.1002/hep.22759 [5] Ghany, M.G., Nelson, D.R., Strader, D.B., Thomas, D.L., Seeff, L.B. (2011) An Update on Treatment of Genotype 1 Chronic Hepatitis C Virus Infection: 2011 Practice Gui- deline by the American Association for the Study of Liver Diseases. Hepatology, 54, 1433-1444. http://dx.doi.org/10.1002/hep.24641 [6] Pearlman, B.L., Traub, N. (2011) Sustained virologic response to antiviral therapy for chronic hepatitis C virus infection: A cure and so much more. Clinical Infectious Diseases, 52, 889-900. http://dx.doi.org/10.1093/cid/cir076 [7] Ko, W.S., Guo, C.H., Hsu, G.S.W., Chiou, Y.L., Yeh, M.S., Yaun, S.R. (2005) Effects of zinc supplementation on the treatment of chronic hepatitis C patients with in- terferon and ribavirin. Clinical Biochemistry, 38, 614-620. http://dx.doi.org/10.1016/j.clinbiochem.2005.04.003 [8] Anton, E., Becker, M.D., Becker A.E. et al. The athero- sclerosis from Egyptian mummies to immune mediated intraplaque inflammation. Dialogue in Cardiovascular Medicine, 2006, 11, 116. [9] Becker, A.E., Boer, O.J., Wal, A.C. The role of inflame- mation and infections in coronary artery disease. Annual Review of Medicine, 2001, 52, 289-297. http://dx.doi.org/10.1146/annurev.med.52.1.289 [10] Libby, P., Hanssson, G.K. et al involvement of immune system in human atherogenesis, current knowledge and unanswered questions. Laboratory Investigation, 1991, 64, 52-50. [11] Wal, A.C., Becker, A.E., Loos, C.M., et al. fibrous and lipid rich plaques. Plaques are part of interchangeable Copyright © 2013 SciRes. OPEN ACCESS 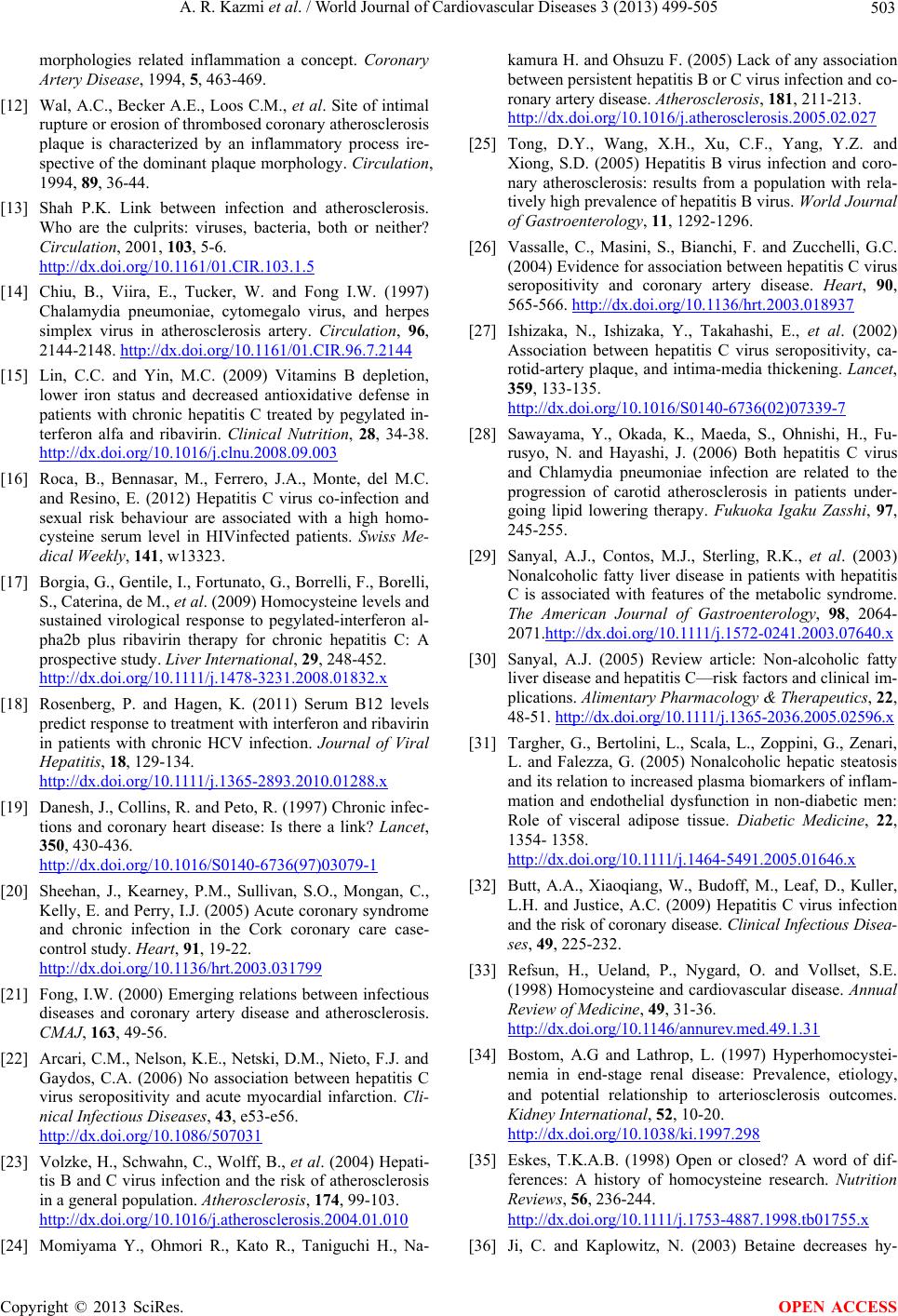 A. R. Kazmi et al. / World Journal of Cardiovascular Diseases 3 (2013) 499-505 503 morphologies related inflammation a concept. Coronary Artery Disease, 1994, 5, 463-469. [12] Wal, A.C., Becker A.E., Loos C.M., et al. Site of intimal rupture or erosion of thrombosed coronary atherosclerosis plaque is characterized by an inflammatory process ire- spective of the dominant plaque morphology. Circulation, 1994, 89, 36-44. [13] Shah P.K. Link between infection and atherosclerosis. Who are the culprits: viruses, bacteria, both or neither? Circulation, 2001, 103, 5-6. http://dx.doi.org/10.1161/01.CIR.103.1.5 [14] Chiu, B., Viira, E., Tucker, W. and Fong I.W. (1997) Chalamydia pneumoniae, cytomegalo virus, and herpes simplex virus in atherosclerosis artery. Circulation, 96, 2144-2148. http://dx.doi.org/10.1161/01.CIR.96.7.2144 [15] Lin, C.C. and Yin, M.C. (2009) Vitamins B depletion, lower iron status and decreased antioxidative defense in patients with chronic hepatitis C treated by pegylated in- terferon alfa and ribavirin. Clinical Nutrition, 28, 34-38. http://dx.doi.org/10.1016/j.clnu.2008.09.003 [16] Roca, B., Bennasar, M., Ferrero, J.A., Monte, del M.C. and Resino, E. (2012) Hepatitis C virus co-infection and sexual risk behaviour are associated with a high homo- cysteine serum level in HIVinfected patients. Swiss Me- dical Weekly, 141, w13323. [17] Borgia, G., Gentile, I., Fortunato, G., Borrelli, F., Borelli, S., Caterina, de M., et al. (2009) Homocysteine levels and sustained virological response to pegylated-interferon al- pha2b plus ribavirin therapy for chronic hepatitis C: A prospective study. Liver International, 29, 248-452. http: //dx.do i.org/10. 1111/j.1478-3231.2008.01832.x [18] Rosenberg, P. and Hagen, K. (2011) Serum B12 levels predict response to treatment with interferon and ribavirin in patients with chronic HCV infection. Journal of Viral Hepatitis, 18, 129-134. http:/ /dx.doi.o rg/ 10.1111 /j.1365-2893.2010.01288.x [19] Danesh, J., Collins, R. and Peto, R. (1997) Chronic infec- tions and coronary heart disease: Is there a link? Lancet, 350, 430-436. http://dx.doi.org/10.1016/S0140-6736(97)03079-1 [20] Sheehan, J., Kearney, P.M., Sullivan, S.O., Mongan, C., Kelly, E. and Perry, I.J. (2005) Acute coronary syndrome and chronic infection in the Cork coronary care case- control study. Heart, 91, 19-22. http://dx.doi.org/10.1136/hrt.2003.031799 [21] Fong, I.W. (2000) Emerging relations between infectious diseases and coronary artery disease and atherosclerosis. CMAJ, 163, 49-56. [22] Arcari, C.M., Nelson, K.E., Netski, D.M., Nieto, F.J. and Gaydos, C.A. (2006) No association between hepatitis C virus seropositivity and acute myocardial infarction. Cli- nical Infectious Diseases, 43, e53-e56. http://dx.doi.org/10.1086/507031 [23] Volzke, H., Schwahn, C., Wolff, B., et al. (2004) Hepati- tis B and C virus infection and the risk of atherosclerosis in a general population. Atherosclerosis, 174, 99-103. http://dx.doi.org/10.1016/j.atherosclerosis.2004.01.010 [24] Momiyama Y., Ohmori R., Kato R., Taniguchi H., Na- kamura H. and Ohsuzu F. (2005) Lack of any association between persistent hepatitis B or C virus infection and co- ronary artery disease. Atherosclerosis, 181, 211-213. http://dx.doi.org/10.1016/j.atherosclerosis.2005.02.027 [25] Tong, D.Y., Wang, X.H., Xu, C.F., Yang, Y.Z. and Xiong, S.D. (2005) Hepatitis B virus infection and coro- nary atherosclerosis: results from a population with rela- tively high prevalence of hepatitis B virus. World Journal of Gastroenterology, 11, 1292-1296. [26] Vassalle, C., Masini, S., Bianchi, F. and Zucchelli, G.C. (2004) Evidence for association between hepatitis C virus seropositivity and coronary artery disease. Heart, 90, 565-566. http://dx.doi.org/10.1136/hrt.2003.018937 [27] Ishizaka, N., Ishizaka, Y., Takahashi, E., et al. (2002) Association between hepatitis C virus seropositivity, ca- rotid-artery plaque, and intima-media thickening. Lancet, 359, 133-135. http://dx.doi.org/10.1016/S0140-6736(02)07339-7 [28] Sawayama, Y., Okada, K., Maeda, S., Ohnishi, H., Fu- rusyo, N. and Hayashi, J. (2006) Both hepatitis C virus and Chlamydia pneumoniae infection are related to the progression of carotid atherosclerosis in patients under- going lipid lowering therapy. Fukuoka Igaku Zasshi, 97, 245-255. [29] Sanyal, A.J., Contos, M.J., Sterling, R.K., et al. (2003) Nonalcoholic fatty liver disease in patients with hepatitis C is associated with features of the metabolic syndrome. The American Journal of Gastroenterology, 98, 2064- 2071.http://dx.doi.org/10.1111 /j.1572-0241.2003.07640.x [30] Sanyal, A.J. (2005) Review article: Non-alcoholic fatty liver disease and hepatitis C—risk factors and clinical im- plications. Alimentary Pharmacology & Therapeutics, 22, 48-51. http://dx.doi.org/10.1111/j.1365-2036.2005.02596.x [31] Targher, G., Bertolini, L., Scala, L., Zoppini, G., Zenari, L. and Falezza, G. (2005) Nonalcoholic hepatic steatosis and its relation to increased plasma biomarkers of inflam- mation and endothelial dysfunction in non-diabetic men: Role of visceral adipose tissue. Diabetic Medicine, 22, 1354- 1358. http:/ /dx.doi.o rg/ 10.1111 /j.1464-5491.2005.01646.x [32] Butt, A.A., Xiaoqiang, W., Budoff, M., Leaf, D., Kuller, L.H. and Justice, A.C. (2009) Hepatitis C virus infection and the risk of coronary disease. Clinical Infectious Disea- ses, 49, 225-232. [33] Refsun, H., Ueland, P., Nygard, O. and Vollset, S.E. (1998) Homocysteine and cardiovascular disease. Annual Review of Medicine, 49, 31-36. http://dx.doi.org/10.1146/annurev.med.49.1.31 [34] Bostom, A.G and Lathrop, L. (1997) Hyperhomocystei- nemia in end-stage renal disease: Prevalence, etiology, and potential relationship to arteriosclerosis outcomes. Kidney International, 52, 10-20. http://dx.doi.org/10.1038/ki.1997.298 [35] Eskes, T.K.A.B. (1998) Open or closed? A word of dif- ferences: A history of homocysteine research. Nutrition Reviews, 56, 236-244. http:/ /dx.doi.o rg/ 10.1111 /j.1753-4887.1998.tb01755.x [36] Ji, C. and Kaplowitz, N. (2003) Betaine decreases hy- Copyright © 2013 SciRes. OPEN ACCESS  A. R. Kazmi et al. / World Journal of Cardiovascular Diseases 3 (2013) 499-505 504 peryhomocysteinemia, endoplasmic reticulum stress, and liver injury in alcohol-fed mice. Gastroenterology, 124, 1488-1499. http://dx.doi.org/10.1016/S0016-5085(03)00276-2 [37] Miner, S.E., Evrovski, J. and Cole, D.E. (1997) Clinical chemistry and molecular biology of homocysteine me- tabolism: An update. Clinical Biochemistry, 30, 189-201. http://dx.doi.org/10.1016/S0009-9120(96)00172-5 [38] Taha, K., El-Shayeb, A., Shafeh, R., Deghady, A. and Eldin, S.Z. (2009) Clinical significance of plasma homo- cysteine concentration in chronic hepatitis C patients with liver cirrhosis. Alexandria Journal of Medicine, 45, 755- 760. [39] Roblin, X., Pofelski, J. and Zarski, J.P. (2007) Steatosis, chronic hepatitis virus C infection and homocysteine. Gastroentérologie Clinique et Biologique, 31, 415-720. http://dx.doi.org/10.1016/S0399-8320(07)89402-4 [40] García-Tevijano, E.R., Berasain, C., Rodríguez, J.A., Corrales, F.J., Arias, R., Martín-Duce, A., Caballería, J., Mato, J.M. and Avila, M.A. (2001) Hyperhomocysteine- mia in liver cirrhosis: Mechanisms and role in vascular and hepatic fibrosis. Hypertension, 38, 1217-1221. http://dx.doi.org/10.1161/hy1101.099499 [41] Finkelstein, J.D. (2003) Methionine metabolism in liver diseases. The American Journal of Clinical Nutrition, 77, 1094-1095. [42] Avila, M.A., Berasain, C. and Torres, L. (2000) Reduced mRNA abundance of the main enzymes involved in me- thionine metabolism in human liver cirrhosis and hepato- cellular carcinoma. Journal of Hepatology, 33, 907-914. http://dx.doi.org/10.1016/S0168-8278(00)80122-1 [43] Lambert, D., Benhayoun, S., Adjalla, C., Gelot, M.M., Renkes, P., Gerard, P., Felden, F., Belleville, F., Gaucher, P., Guéant, J.L. and Nicolas, J.P. (1997) Alcoholic cir- rhosis and cobalamin metabolism. Digestion, 58, 64-71. http://dx.doi.org/10.1159/000201425 [44] Halifeoglu, I., Gur, B. and Aydin, S. (2004) Plasma trace elements, vitamin B12, folate and homocysteine levels in cirrhotic patients compared to controls. Biochemistry, 69, 693-696. [45] Gulsen, M., Yesilova, Z., Bagci, S., Uygun, A., Ozcan, A., Ercin, C.N., Erdil, A., Sanisoglu, S.Y., Cakir, E., Ates, Y., Erbil, M.K., Karaeren, N. and Dagalp, K. (2005) Elevated plasma homocysteine concentrations as a predictor of steatohepatitis in patients with non-alcoholic fatty liver disease. Journal of Gastroenterology and Hepatology, 20, 1448-1455. [46] Jaeckel, E., Cornberg, M., Wedemeyer, H., Santantonio, T., Mayer, J., Zankel, H., Dietrich, M., Trautwein, C. and Manns, M.P. (2001) Treatment of acute hepatitis C with interferon alfa-2b. The New England Journal of Medicine, 345, 1452-1457. http://dx.doi.org/10.1056/NEJMoa011232 [47] Werstuck, G.H., Lentz, S.R. and Dayal, S. (2001) Ho- mocysteine-induced endoplasmic reticulum stress causes dysregulation of the cholesterol and triglyceride biosyn- thetic pathways. The Journal of Clinical Investigation, 107, 1263-1267. http://dx.doi.org/10.1172/JCI11596 [48] Mudd, S.H., Levy, H.L. and Skovby, F. (1995) Disorders of transsulfuration. In: Scriver, C.R., Beaudet, A.L., Sly, W.S. and Valle, D., Eds., The metabolic and molecular bases of inherited disease, Vol. 1, McGraw-Hill, New York, 1279-1327. [49] Carey, M.C., Donovan, D.E., FitzGerald, O. and McAuley, F.D. (1968) Homocystinuria: A clinical and pathological study of nine subjects in six families. The American Journal of Medicine, 45, 7-25. http://dx.doi.org/10.1016/0002-9343(68)90003-X [50] Mudd, S.H., Skovby, F., Levy, H.L., et al. (1985) The natural history of homocystinuria due to cystathionine b-synthase deficiency. The American Journal of Human Genetics, 37, 1-31. [51] Malinow, M.R., Kang, S.S., Taylor, L.M., et al. (1989) Prevalence of hyperhomocyst(e)inemia in patients with peripheral arterial occlusive disease. Circulation, 79, 1180-1188. http://dx.doi.org/10.1161/01.CIR.79.6.1180 [52] Coull, B.M., Malinow, M.R., Beamer, N., Sexton, G., Nordt, F. and de Garmo, P. (1990) Elevated plasma ho- mocyst(e)ine concentration as a possible independent risk factor for stroke. Stroke, 21, 572-576. http://dx.doi.org/10.1161/01.STR.21.4.572 [53] Malinow, M.R., Sexton, G., Averbuch, M., Grossman, M., Wilson, O. and Upson, B. (1990) Homocyst(e)ine in daily practice: Levels in coronary heart disease. Coronary Ar- tery Disease, 2, 4-12. [54] Mudd, S.H., Uhlendorf, B.W., Freeman, J.M., Finkelstein, J.D. and Shih, V.E. (1972) Homocystinuria associated with decreased methylenetetrahydrofolate reductase ac- tivity. Biochemical and Biophysical Research Communi- cations, 46, 905-912. http://dx.doi.org/10.1016/S0006-291X(72)80227-4 [55] Erbe, R.W. (1986) Inborn errors of folate metabolism. In: Blakely, R.L. and Whitehead, V.M., Eds., Folate and pterins: Nutritional, pharmacological, and physiological aspects. Marcel Dekker, New York, 413-425. [56] D’Angelo, A. and Selhub, J. (1997) Homocysteine and thrombotic disease. Blood, 90, 1-11. [57] Kang, S.S., Zhou, J., Wong, P.W.K., Kowalisyn, J. and Strokosch, G. (1988) Intermediate homocysteinemia: A thermolabile variant of methylenetetrahydrofolate reduce- tase. The American Journal of Human Genetics, 43, 414- 421. [58] Frosst, P., Blom, H.J., Milos, R., et al. (1995) A candi- date genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nature Genetics, 10, 111-113. http://dx.doi.org/10.1038/ng0595-111 [59] Frosst, P., Blom, H.J., Milos, R., Goyette, P., Sheppard, C.A., Matthews, R.G., Boers, G.J., den Heijer, M., Kluijtmans, L.A., van den Heuvel, L.P. and Rozen, R. (1995) A candidate genetic risk factor for vascular dis- ease: A common mutation in methylenetetrahydrofolate reductase. Nature Genetics, 10, 111-113. http://dx.doi.org/10.1038/ng0595-111 [60] Goyette, P., Sumner, J.S., Milos, R., Duncan, A.M., Rosenblatt, D.S., Matthews, R.G. and Rozen, R. (1994) Human methylenetetrahydro folate reductase: Isolation of cDNA, mapping and mutation identification. Nature Ge- Copyright © 2013 SciRes. OPEN ACCESS  A. R. Kazmi et al. / World Journal of Cardiovascular Diseases 3 (2013) 499-505 Copyright © 2013 SciRes. 505 OPEN ACCESS netics, 7, 195-200. http://dx.doi.org/10.1038/ng0694-195 [61] Put van der, N.M.J., Gabreels, F., Stevens, E.M., Smeit- ink, J.A., Trijbels, F.J., Eskes, T.K., van den Heuvel, L.P. and Blom, H.J. (1998) A second common mutation in the methylenetetrahydrofolate reductase gene: An additional risk factor for neural-tube defects? The American Journal of Human Genetics, 62, 1044-1051. http://dx.doi.org/10.1086/301825 [62] Andreassi, M.G., Botto, N., Battaglia, D., Antonioli, E., Masetti, S., Manfredi, S., Colombo, M.G., Biagini, A. and Clerico, A. (2003) Methylenetetrahydro folate reduc- tase gene C677T polymorphism, homocysteine, vitamin B12, and DNA damage in coronary artery disease. Hu- man Genetics, 112, 171-177.
|