P. J. Boda / Health 5 (20 13) 12-18 17
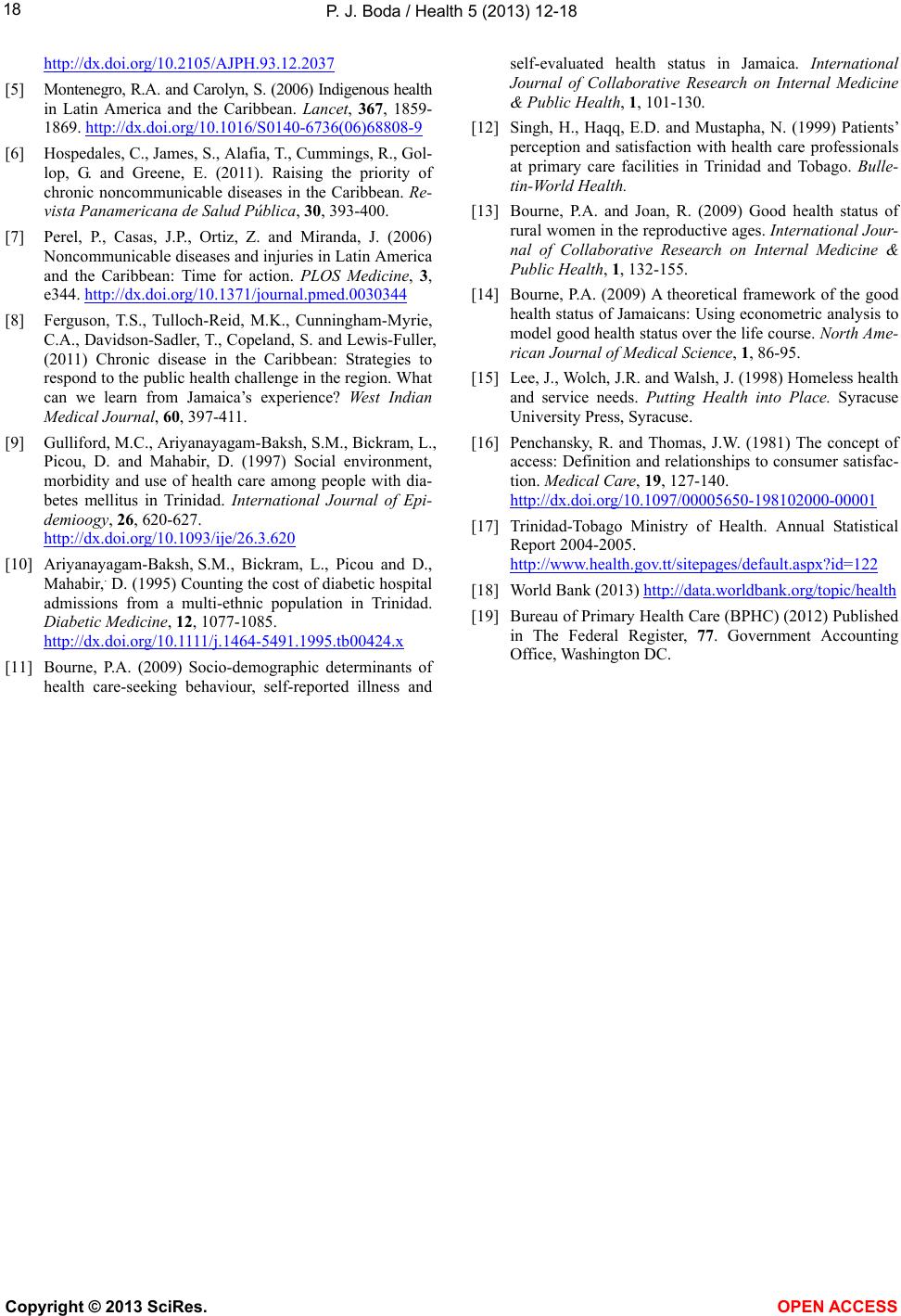
ing by the hospital or any number of other possibilities.
Likewise, in the Sangre Grande facility, digestive and
respiratory illness accounted for the majority of hospital
stays but represented a much smaller volume at the other
facilities. Again, while likely explanation may exist, it
appears that different NCDs prevail in different areas.
This warrants further investigation
4. SUMMARY
The disease burden of Trinidad is equal to the burden
of higher income countries. The small size limits natural,
economic, human and infrastructure resources and there-
fore limits the ability of SIDS to effectively combat
NCDs. Although there are a number of medical schools
throughout the re gion, ther e remains a shor tag e of trained
medical doctors on many islands, including Trinidad.
This shortage impacts access hospital services for tens of
thousands on the island.
Penchansky’s five dimensions of access are all chal-
lenging on the island. The first, availability, defines
numbers of providers such as physicians and hospital
facilities in relation to the demand for their services. On
Trinidad, the availability b arrier is rooted in the shortage
of physicians. This study revealed that the population to
provider ratio was excessive in many areas. The second
dimension, geographic accessibility, is a barrier for ap-
proximate 71,500 people who live outside the 15 mile
zone from each of the four hospitals and experience ex-
cessive time and excessive distances to receive hospital
care.
Accommodation, the degree that services meet the
needs of patients and include hours of service, waiting
times, appointments and scheduling, is also a barrier on
Trinidad, again due to provider shortages. Research has
documented that patient satisfaction is low [11-14].
Acceptability impedes access on the island due to
mixed ethnicity, language and culture differences. Ap-
proximately 45% of the population are Indian, 45% Af-
rican, and 10% other ethnicities. It is often difficult, for
example, for an African to locate a physician that under-
stands the African cu lture.
Affordability is a person’s ability to pay for services
and includes insurance coverage. Due to limited re-
sources, there are also limited employments, insurance
and affordability that become barriers.
In other words, all five barriers as outlined by Pen-
chansky and Thomas are operating on the island of
Trinidad and impact the ability of health care officials to
effectively reduce the burden of NCDs [16]. Although
Trinidad has made progress toward its commitment to
the Port of Spain Declaration, th ere is additional work to
complete to reach the country’s goals in combatting the
increase of NCD deaths.
Additional research is needed to evaluate access to
clinics in the health districts with updated figures. How-
ever, many government agencies that collect and manage
the data are reluctant to share that information for a va-
riety of reasons. With more cooperation and access to
information, the human resource shortage in the region
would be greatly abetted by others. Many researchers in
the region have requested that organizations make spatial
data available. Unfortunately, to date, many Caribbean
SIDS often are not willing or able to provide these nec-
essary items due to limited size, as well as limited human,
economic and technology resources.
Further research is also needed regarding the regional
variations in illnesses reported by the hospital discharge
summaries. Are these variations indeed representative of
the populations living near these facilities? If so, addi-
tional clinic hours and educational programs would be
valuable interven tions for maintaining healthy communi-
ties and minimizing hospital use.
5. ACKNOWLEDGEMENTS
A special note of acknowledgement is due to the University of the
West Indies, St. Augustine Campus and Dr. Bheshem Ramlal for shape-
files, physician and community data.
6. FUNDING ACKNOWLEDGE MENTS
This study was significantly aided financially by a grant from Middle
Tennessee State University and the Faculty Research and Creative
Activity Committee grant. The grant provided travel expenses to Trini-
dad-Tobago in 2011 and 2012.
REFERENCES
[1] World Health Organization (WHO) (2013) Chronic ill-
nesses.
http://www.who.int/topics/chronicdiseases/factsheets/en/
index.html
[2] Population Reference Bureau (2013) Noncommunicable
diseases and youth: A critical window of opportunity for
Latin America/Caribbean. Policy Brief, Population Ref-
erence Bureau.
[3] Dachs, J., Norberto, W., Ferrer, M., Florez, C., Elisa, B.,
Aluisio, J.D., Narváez, R. and Valdivia, M. (2002) Ine-
qualities in health in Latin America and the Caribbean:
Descriptive and exploratory results for self-reported
health problems and health care in twelve countries. Re-
vista Panamericana de Salud Pública, 11 , 335-355.
http://www.scielosp.org/scielo.php?script=sci_arttext&pi
d=S1020-498920 0200050000 9&lng=en&tlng=e n.10.1590/
S1020-49892002000500009
[4] Naomar, A.-F., Ichiro, K., Alberto, P.F. and Norberto,
W.D.J. (2003) Research on health inequalities in Latin
America and the Caribbean: Bibliometric analysis (1971-
2000) and Descriptive Content Analysis (1971-1995).
American Journal of Public Health, 93, 2037-2043.
Copyright © 2013 SciRes. OPEN A CCESS