L. L. Yang et al. / Open Journal of Stomatology 3 (2013) 425-432 431
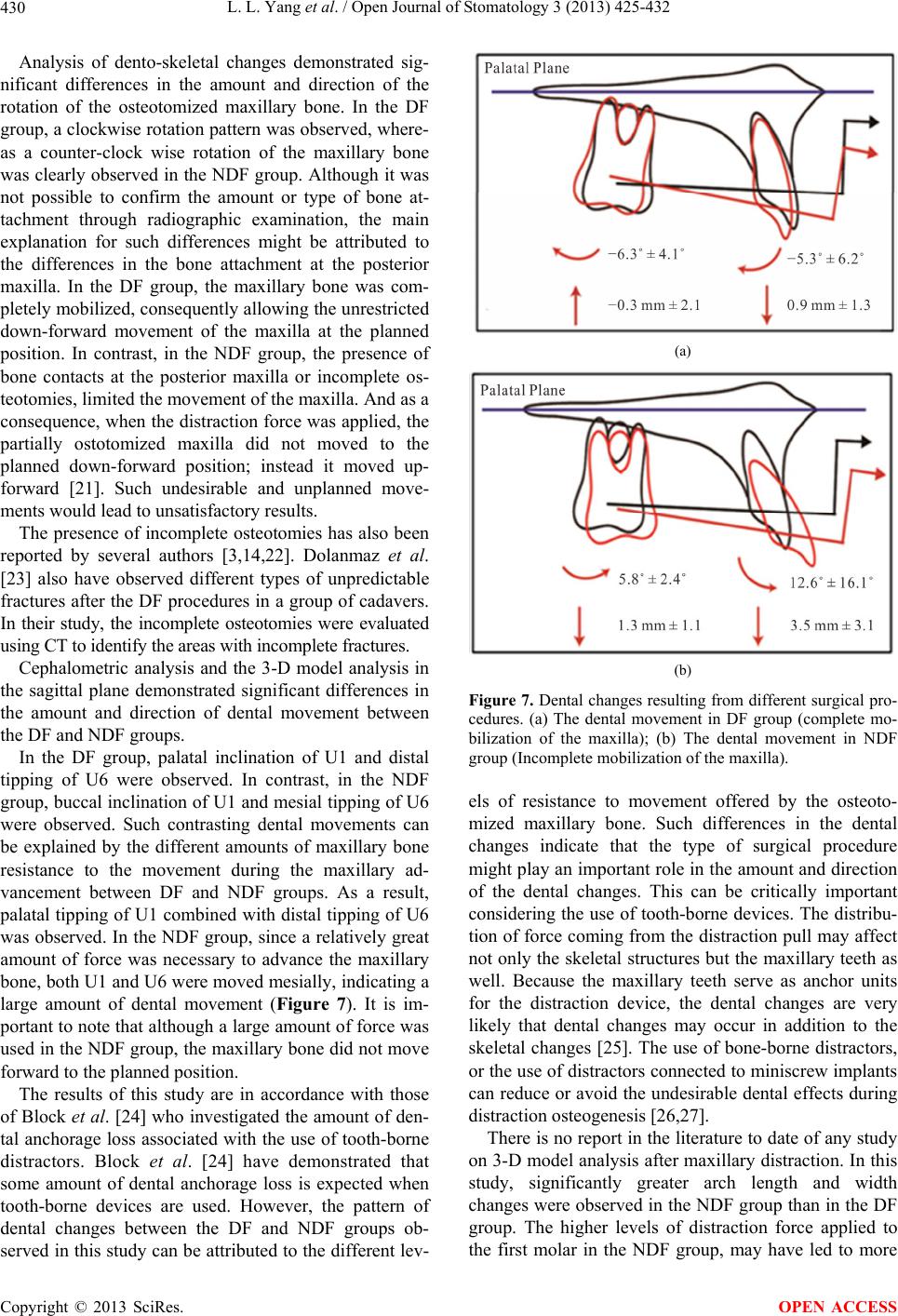
dental movement than in the DF group. Greater buccal
inclination of the maxillary first molar produced a
greater arch width increase, and greater anterior move-
ment, and labial inclination of the maxillary incisors
produced a greater arch length increase. The mostly force
applied to the maxillary first molar might cause this ex-
pansion effect because the distraction force was deliv-
ered by a tooth-borne device that was attached to the
band on the first molar. The inclination effect on the first
molar was greater than on the incisor, canine and premo-
lar due to the attended mode.
In the NDF group, the second premolar and first molar
extrusion might be due to the counter rotation of the
tooth-borne device. The posterior maxilla remained con-
nected to the skull base following the NDF procedure,
which might have led to the extrusion of the second
premolar and first molar. In contrast, the osteotomized
maxilla was completely mobilized in the DF group. In
this study, the mobilized maxilla was not just the result
of forward movement, but also of downward movement.
This downward movement may have led to clockwise
rotation of the tooth-borne device, which may have pro-
duced the second premolar and first molar intrusion.
5. CONCLUSIONS
The use of the NDF procedure resulted in greater
amounts of dental anchorage loss than resulted from the
DF procedures when tooth-borne devices were used dur-
ing maxillary distraction osteogenesis. The type of sur-
gical procedure might play an important role in the
amount and direction of the dental changes.
Further studies, with increased numbers of subjects,
are necessary to evaluate the effects of different cleft
types on the dentoalveolar changes during maxillary dis-
traction osteogenesis.
6. ACKNOWLEDGMENTS
The authors gratefully acknowledge a grant from Thailand research
Fund (RSA 5480029), and grant from the Faculty of Dentistry, Chiang
Mai University. The authors acknowledge the assistance of Dr. M. K.
Kevin O. Carroll, Professor Emeritus of the University of Mississippi
School of Dentistry, USA, and Faculty Consultant at the Chiang Mai
University Faculty of Dentistry, Thailand, in the preparation of the
manuscript.
REFERENCES
[1] Ilizarov, G.A. (1989) The tension-stress effect on the
genesis and growth of tissues. Part I. The influence of
stability of fixation and soft-tissue preservation. Clinical
Orthopaedics and Related Research, 238, 249-281.
[2] Ilizarov, G.A. (1989) The tension-stress effect on the
genesis and growth of tissues: Part II. The influence of
the rate and frequency of distraction. Clinical Orthopae-
dics and Related Research, 239, 263-285.
[3] Molina, F., et al. (1998) Maxillary distraction: Aesthetic
and functional benefits in cleft lip-palate and prognathic
patients during mixed dentition. Plastic and Reconstruc-
tive Surgery, 101, 951-963.
http://dx.doi.org/10.1097/00006534-199804040-00010
[4] Samchukov, M.L., Cherkashin, A.M. and Cope, J.B.,
(1998) Distraction osteogenesis: History and biologic ba-
sis of new bone formation. In: Lynch, S. E. Genco, R.J.
and Marx, R.E., Eds., Tissue Engineering: Applications in
Maxillofacial Surgery and Periodontics, Quintessence,
Carlo Stream.
[5] Figueroa, A.A., Polley, J.W. and Ko, E.W. (1999) Maxil-
lary distraction for the management of cleft maxillary hy-
poplasia with a rigid external distraction system. Semi-
nars in Orthodontics, 5, 46-51.
http://dx.doi.org/10.1016/S1073-8746(99)80042-5
[6] Polley, J.W. and Figueroa, A.A. (1997) Management of
severe maxillary deficiency in childhood and adolescence
through distraction osteogenesis with an external, adjust-
able, rigid distraction device. Journal of Craniofacial
Surgery, 8, 186.
http://dx.doi.org/10.1097/00001665-199705000-00008
[7] Polley, J.W. and Figueroa, A.A. (1998) Rigid external
distraction: its application in cleft maxillary deformities.
Plastic and Reconstructive Surgery, 102, 1373-1374.
http://dx.doi.org/10.1097/00006534-199810000-00007
[8] Figueroa, A.A., et al. (2004) Long-term skeletal stability
after maxillary advancement with distraction osteogenesis
using a rigid external distraction device in cleft maxillary
deformities. Plastic and Reconstructive Surgery, 114,
1393-1394.
http://dx.doi.org/10.1097/01.PRS.0000138593.89303.1B
[9] Rachmiel, A., Aizenbud, D. and Peled, M. (2006) Dis-
traction osteogenesis in maxillary deficiency using a rigid
external distraction device. Plastic and Reconstructive
Surgery, 117, 2399-2406.
http://dx.doi.org/10.1097/01.prs.0000204798.50710.a7
[10] Suzuki, E.Y., Motohashi, N. and Ohyama, K. (2004)
Longitudinal dento-skeletal changes in UCLP patients
following maxillary distraction osteogenesis using RED
system. Journal of Medical and Dental Sciences, 51,
27-33.
[11] Lo, L.J., Hung, K.F. and Chen, Y.R. (2002) Blindness as
a complication of Le Fort I osteotomy for maxillary dis-
traction. Plastic and Reconstructive Surgery, 109, 699-
700.
[12] Yamauchi, K., Mitsugi, M. and Takahashi, T. (2006)
Maxillary distraction osteogenesis using Le Fort I os-
teotomy without intraoperative down-fracture. Interna-
tional Journal of Oral and Maxillofacial Surgery, 35,
493-498. http://dx.doi.org/10.1016/j.ijom.2006.01.008
[13] Kanno, T., et al. (2008) Long-term skeletal stability after
maxillary advancement with distraction osteogenesis in
non-growing patients. Journal of Oral and Maxillofacial
Surgery, 66, 1833-1846.
http://dx.doi.org/10.1016/j.joms.2007.10.013
[14] Nadjmi, N., Schutyser, F. and Van Erum, R. (2006)
Copyright © 2013 SciRes. OPEN ACCESS