B. Abir et al. / Open Journal of Stomatology 3 (2013) 419-424
422
Figure 9. Intraoperative view of a harvested osteocutaneous
fibula free flap.
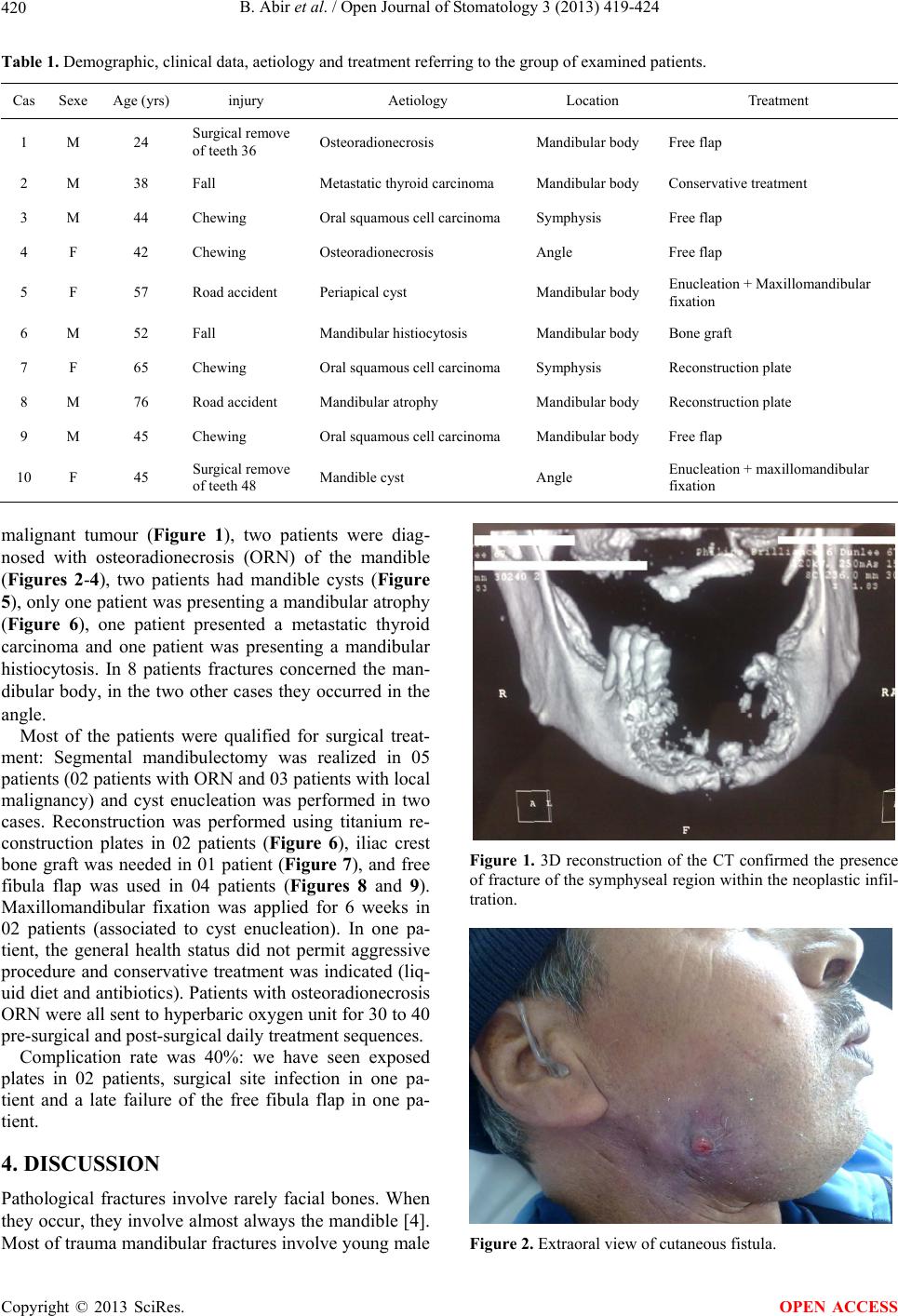
years (80% of our series). This might be explained by the
fact that elderly patients are more concerned by malign-
nant conditions and atrophic edentulous jaws [1]. Copes
suggested that spontaneous fractures of the mandible are
often in relation with mastication forces. Anterior man-
dibular fractures are due to the action of depressor mus
cles, while posterior fractures are due to the action of
elevator muscles [5]. In the most cases, osteoradionecro-
sis ORN is suggested as a cause of pathological man-
dibular fractures [2]. ORN occurs after radiotherapy, and
is in relation with hypoxia, hypovascularity and hypo-
cellularity as suggested by the 3H theory of Marx [6].
These phenomena alter bone capacity of reparation. They
occur more often in angular, retromolar and horizontal
parts of mandible because of their unique centromedullar
vascularity. A study including 1000 patients who had
head and neck radiation showed that 2,6% of them de-
veloped ORN, and 23% of these progressed to patho-
logical fracture of mandible [7]. In ORN context, patho-
logical fracture of the mandible is classified as a stage III
ORN by Marx a nd Myers [8].
In this study, ORN comes in the second rank after ma-
lignancies. Oral primary cancer as spinocellular carci-
nomas, or mandibular metastasis are also frequently in-
volved in pathological fractures. Leukaemias, lympho-
mas and especially multiple myeloma are blood produc-
tive system cancers that can cause pathological fractures
of mandible when they concern this bone. It is estimated
that only 1% of malignant tumours found in the oral re-
gion are metastases of breast, prostate, thyroid, kidney or
lung cancer [2]. In fact, the true incidence of metastases
in mandible is unknown, as radiography exam of this
region is not included in systematic survey for metastasis.
Facial bones are less often touched by metastases than
long bones. It seems like it is because of the decrease of
red bone marrow and blood vessels that occurs in the
jaws with age. When they occur, metastases concern
almost always the mandible. This is thought that it is due
to the greater presence of hematopoietic tissue in mandi-
ble than in the other facial bones [9].
Osteomyelitis was also described as a frequent cause
of pathological mandibular fractures. In a 44 patients
study reported by Coletti and Ord [3], osteomyelitis
came in second position (19%) after ORN (49%). Os-
teomyelitis can be associated with implants or third
moral extractions, and there are often causes underlying
predisposing condition such as diabetes.
Biphosphonate related osteonecrosis is a relatively re-
cent recognized pathology, as Marx and other authors
(Wang, Migliorati) [10-12] described the first reports of
this condition in 2003, even if “phossy jaws” cases were
reported more than a century ago. This condition appears
often associated with predisposing pathology as corti-
cotherapy or immunosuppressive treatment, chemother-
apy, osseous diseases, bad nutritional condition or to-
bacco consumption and bad oral condition [11,13]. The
most common clinical presentation is an osteitis occur-
ring after a tooth extraction (86%) [14]. The physiopa-
thology of osteochemonecrosis remains unclear, however
four factors appear to have a role in its occurrence: A)
An accumulation of biphosphonates in the jaw, due to a
fast osseous turnover in relation to the presence of teeth
and the daily activity of jaws. This phenomenon stops
bone remodelling around teeth and periodontal ligament.
B) A high release of cytokines. C) The inhibition of an-
giogenesis and the acceleration of apoptosis. D) The
immunosuppressive condition seen in all patients with a
metastatic disease and under chemotherapy or corticos-
teroids [15].
Iatrogenic condition as a wisdom-tooth extraction can
be the cause of a mandibular fracture. It occurs most
frequently in male patients aged between 25 and 50-year-
old, in the two weeks following surgery [3]. Fractures in
atrophic or long-time edentulous mandible can be seen
after a trauma. However, spontaneous fracture in an
atrophic mandible is an uncommon event. Luhr et al.
[16], defined the atrophic mandible as having less than
20 mm in its body vertical height. In their study include-
ing 84 edentulous patients, they classified atrophic man-
dibles in 3 stages: I) 16 - 20 mm, II) 11 - 15 mm, III) 10
mm or less. Other conditions can also be involved in
pathological fractures of mandible. They can be classi-
fied in different ways.
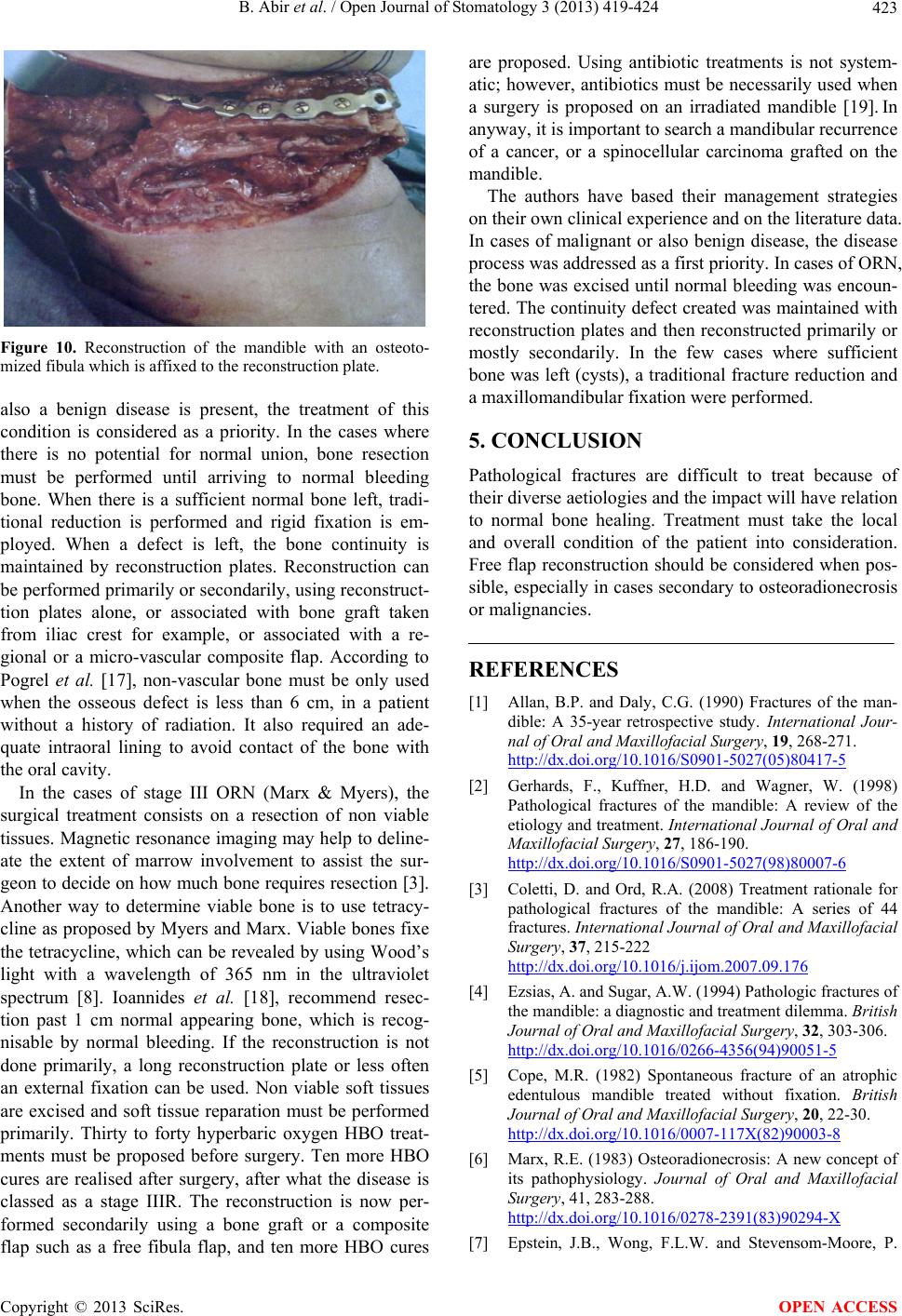
Treatments of pathological fractures of mandible are
complex because of their multiple aetiologies, their oc-
currence in patients suffering several serious diseases,
and the local bone condition which is very often infected
and non viable. Bone healing in these situations has big
chances to fail, and takes longer time. Treatment strategy
must be adapted to each patient individually. And even if
management strategies are different from aetiology to
another, some rules are common according to Coletti and
Ord’s paper (Figure 10) [3]. A special attention should
be paid to optimize the general health condition of the
patient. Pain, functional and nutritional problems must be
cared, and a soft diet must be started. If a malignant or
Copyright © 2013 SciRes. OPEN ACCESS