 Advances in Bioscience and Biotechnology, 2013, 4, 15-23 ABB http://dx.doi.org/10.4236/abb.2013.411A2003 Published Online November 2013 (http://www.scirp.org/journal/abb/) Homocysteine and oxidative stress in acute stroke* Laura Nanetti1#†, Arianna Vignini1#, Francesca Raffaelli1, Alessia Giulietti1, Marco Bartolini2, Cecilia Perozzi2, Mauro Silvestrini2, Leandro Provinciali2, Laura Mazzanti1 1Department of Experimental and Clinical Medicine, Università Politecnica delle Marche, Ancona, Italy 2Department of Clinical Science, Biochemistry Section, Università Politecnica delle Marche, Ancona, Italy Email: †l_nanetti@hotmail.com Received 2 August 2013; revised 15 September 2013; accepted 1 October 2013 Copyright © 2013 Laura Nanetti et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Homocysteine is a sulfhydryl-containing amino acid derived from the essential amino acid methionine. Total Hcy plasma level varies in the range of 5 - 15 μmol/L in the normal population. Our aim in this study was to investigate the possible correlations among homocysteine plasma levels, oxidative stress parameters and clinical evolution of stroke. Fifty pa- tients with large-vessel ischemic stroke were studied. Biochemical determinations were performed at entry (T0) and then repeated one month after stroke (T1). Homocysteine levels were significantly increased at T0 with respect to T1 and showed a significant posi- tive correlation with the expression of oxidative stress markers and a negative correlation with indicators of protective anti stress activity. A significant increase of antioxidant activity occurred from T0 to T1 and changes were associated with the severity of clinical conditions. In particular, the extent of homocysteine and of oxidative stress markers plasmatic levels re- duction and of the contemporary increase in anti stress biochemical activities were associated with a reduction of NIHSS scores. These findings, besides confirming an involvement of oxidative stress in in- fluencing the evolution of stroke, suggest a role for homocysteine as a potentially modifiable biochemical alteration able to modulate some mechanisms in- volved in the production of ischemic damage. Keywords: Homocysteine; Acute Stroke; Oxidative Stress; Platelets 1. INTRODUCTION Homocysteine (Hcy) is a sulfhydryl-containing amino acid derived from the essential amino acid methionine, which is abundant in animal sources of protein [1]. Total Hcy (tHcy) plasma level varies in the range of 5 - 15 μmol/L in the normal population [2]. Minor genetic ab- normalities or nutritional deficiencies of B vitamins, such as folic acid involved in methionine metabolism, can lead to increased tHcy concentration. The involve- ment of homocysteine in atherosclerosis was first prom- ulgated by McCully on the basis of his pathological findings in infants with hyperhomocysteinemia resulting from inborn metabolism deficiency [3]. In experimental studies, homocysteine causes oxidative stress and vascu- lar inflammation, damages endothelial cells, inhibits en- dothelium-dependent relaxation, and enhances throm- bogenicity [4]. A large body of epidemiological studies suggest that increased homocysteine level may be con- sidered as an independent risk factor for vascular dis- eases, including stroke [5-7]. Ischemic stroke is a heterogeneous syndrome caused by multiple disease mechanisms, resulting in a disruption of cerebral blood flow with subsequent tissue damage. The extent of focal cerebral injury is influenced by dif- ferent molecular mechanisms. An alteration of the physi- ologic balance between production and degradation of enzymatic activity involved in the regulation of tissue oxidative status may play a role in influencing the results of the ischemic condition [8,9]. A recent study by our group proposed that cerebral ischemia causes the release of nitric oxide (NO) from the vascular endothelium. An elevated circulating concentration of the sulfur-contain- ing amino acid homocysteine, hyperhomocysteinemia, produces complex changes within blood vessels. In the peripheral circulation, these changes include oxidative stress. Hyperhomocysteinemia-induced oxidative stress may occur as a result of decreased expression and/or activity of key antioxidant enzymes as well as increased enzymatic generation of superoxide anion (the precursor for multiple reactive oxygen and reactive nitrogen spe- *Conflict of interest: The authors declare that they have no conflict o interest. #These Authors equally contributed in this work. †Corresponding author. OPEN ACCESS 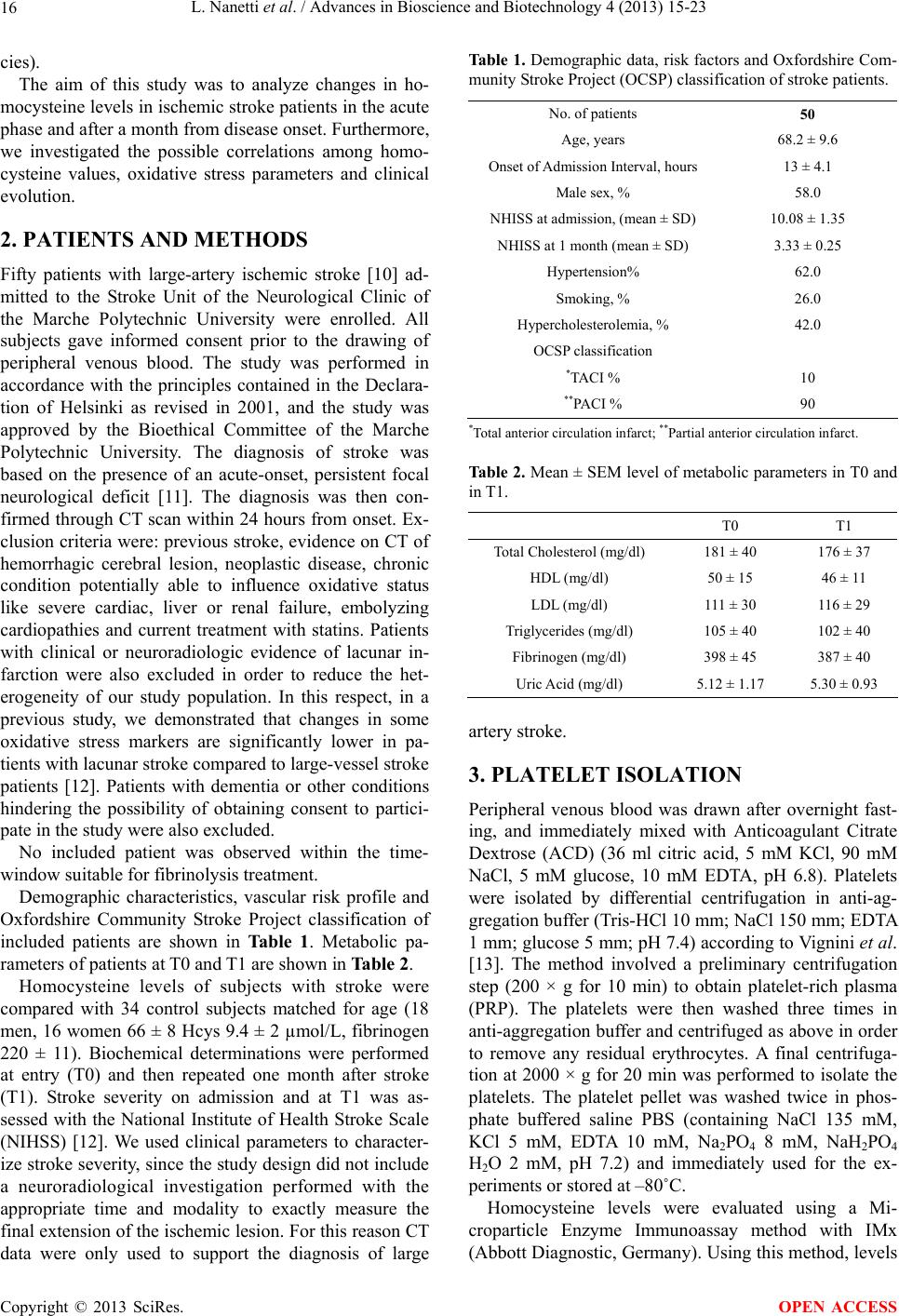 L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 16 cies). The aim of this study was to analyze changes in ho- mocysteine levels in ischemic stroke patients in the acute phase and after a month from disease onset. Furthermore, we investigated the possible correlations among homo- cysteine values, oxidative stress parameters and clinical evolution. 2. PATIENTS AND METHODS Fifty patients with large-artery ischemic stroke [10] ad- mitted to the Stroke Unit of the Neurological Clinic of the Marche Polytechnic University were enrolled. All subjects gave informed consent prior to the drawing of peripheral venous blood. The study was performed in accordance with the principles contained in the Declara- tion of Helsinki as revised in 2001, and the study was approved by the Bioethical Committee of the Marche Polytechnic University. The diagnosis of stroke was based on the presence of an acute-onset, persistent focal neurological deficit [11]. The diagnosis was then con- firmed through CT scan within 24 hours from onset. Ex- clusion criteria were: previous stroke, evidence on CT of hemorrhagic cerebral lesion, neoplastic disease, chronic condition potentially able to influence oxidative status like severe cardiac, liver or renal failure, embolyzing cardiopathies and current treatment with statins. Patients with clinical or neuroradiologic evidence of lacunar in- farction were also excluded in order to reduce the het- erogeneity of our study population. In this respect, in a previous study, we demonstrated that changes in some oxidative stress markers are significantly lower in pa- tients with lacunar stroke compared to large-vessel stroke patients [12]. Patients with dementia or other conditions hindering the possibility of obtaining consent to partici- pate in the study were also excluded. No included patient was observed within the time- window suitable for fibrinolysis treatment. Demographic characteristics, vascular risk profile and Oxfordshire Community Stroke Project classification of included patients are shown in Table 1. Metabolic pa- rameters of patients at T0 and T1 are shown in Table 2. Homocysteine levels of subjects with stroke were compared with 34 control subjects matched for age (18 men, 16 women 66 ± 8 Hcys 9.4 ± 2 µmol/L, fibrinogen 220 ± 11). Biochemical determinations were performed at entry (T0) and then repeated one month after stroke (T1). Stroke severity on admission and at T1 was as- sessed with the National Institute of Health Stroke Scale (NIHSS) [12]. We used clinical parameters to character- ize stroke severity, since the study design did not include a neuroradiological investigation performed with the appropriate time and modality to exactly measure the final extension of the ischemic lesion. For this reason CT data were only used to support the diagnosis of large Table 1. Demographic data, risk factors and Oxfordshire Com- munity Stroke Project (OCSP) classification of stroke patients. No. of patients 50 Age, years 68.2 ± 9.6 Onset of Admission Interval, hours 13 ± 4.1 Male sex, % 58.0 NHISS at admission, (mean ± SD) 10.08 ± 1.35 NHISS at 1 month (mean ± SD) 3.33 ± 0.25 Hypertension% 62.0 Smoking, % 26.0 Hypercholesterolemia, % 42.0 OCSP classification *TACI % 10 **PACI % 90 *Total anterior circulation infarct; **Partial anterior circulation infarct. Table 2. Mean ± SEM level of metabolic parameters in T0 and in T1. T0 T1 Total Cholesterol (mg/dl) 181 ± 40 176 ± 37 HDL (mg/dl) 50 ± 15 46 ± 11 LDL (mg/dl) 111 ± 30 116 ± 29 Triglycerides (mg/dl) 105 ± 40 102 ± 40 Fibrinogen (mg/dl) 398 ± 45 387 ± 40 Uric Acid (mg/dl) 5.12 ± 1.17 5.30 ± 0.93 artery stroke. 3. PLATELET ISOLATION Peripheral venous blood was drawn after overnight fast- ing, and immediately mixed with Anticoagulant Citrate Dextrose (ACD) (36 ml citric acid, 5 mM KCl, 90 mM NaCl, 5 mM glucose, 10 mM EDTA, pH 6.8). Platelets were isolated by differential centrifugation in anti-ag- gregation buffer (Tris-HCl 10 mm; NaCl 150 mm; EDTA 1 mm; glucose 5 mm; pH 7.4) according to Vignini et al. [13]. The method involved a preliminary centrifugation step (200 × g for 10 min) to obtain platelet-rich plasma (PRP). The platelets were then washed three times in anti-aggregation buffer and centrifuged as above in order to remove any residual erythrocytes. A final centrifuga- tion at 2000 × g for 20 min was performed to isolate the platelets. The platelet pellet was washed twice in phos- phate buffered saline PBS (containing NaCl 135 mM, KCl 5 mM, EDTA 10 mM, Na2PO 4 8 mM, NaH2PO4 H2O 2 mM, pH 7.2) and immediately used for the ex- periments or stored at –80˚C. Homocysteine levels were evaluated using a Mi- croparticle Enzyme Immunoassay method with IMx (Abbott Diagnostic, Germany). Using this method, levels Copyright © 2013 SciRes. OPEN ACCESS 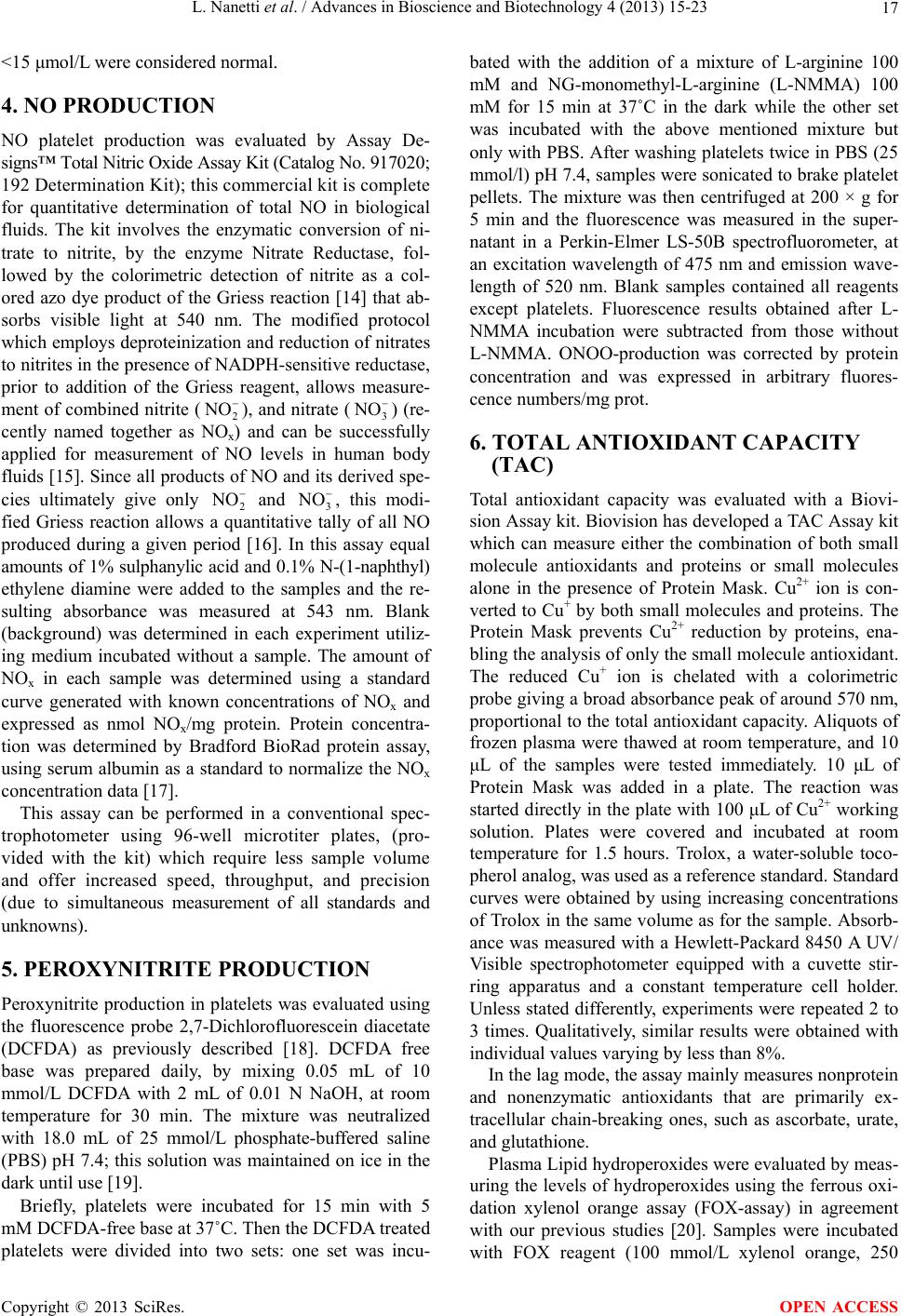 L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 17 <15 μmol/L were considered normal. 4. NO PRODUCTION NO platelet production was evaluated by Assay De- signs™ Total Nitric Oxide Assay Kit (Catalog No. 917020; 192 Determination Kit); this commercial kit is complete for quantitative determination of total NO in biological fluids. The kit involves the enzymatic conversion of ni- trate to nitrite, by the enzyme Nitrate Reductase, fol- lowed by the colorimetric detection of nitrite as a col- ored azo dye product of the Griess reaction [14] that ab- sorbs visible light at 540 nm. The modified protocol which employs deproteinization and reduction of nitrates to nitrites in the presence of NADPH-sensitive reductase, prior to addition of the Griess reagent, allows measure- ment of combined nitrite (2 NO ), and nitrate (3 NO ) (re- cently named together as NOx) and can be successfully applied for measurement of NO levels in human body fluids [15]. Since all products of NO and its derived spe- cies ultimately give only 2 and 3, this modi- fied Griess reaction allows a quantitative tally of all NO produced during a given period [16]. In this assay equal amounts of 1% sulphanylic acid and 0.1% N-(1-naphthyl) ethylene diamine were added to the samples and the re- sulting absorbance was measured at 543 nm. Blank (background) was determined in each experiment utiliz- ing medium incubated without a sample. The amount of NOx in each sample was determined using a standard curve generated with known concentrations of NOx and expressed as nmol NOx/mg protein. Protein concentra- tion was determined by Bradford BioRad protein assay, using serum albumin as a standard to normalize the NOx concentration data [17]. NO NO This assay can be performed in a conventional spec- trophotometer using 96-well microtiter plates, (pro- vided with the kit) which require less sample volume and offer increased speed, throughput, and precision (due to simultaneous measurement of all standards and unknowns). 5. PEROXYNITRITE PRODUCTION Peroxynitrite production in platelets was evaluated using the fluorescence probe 2,7-Dichlorofluorescein diacetate (DCFDA) as previously described [18]. DCFDA free base was prepared daily, by mixing 0.05 mL of 10 mmol/L DCFDA with 2 mL of 0.01 N NaOH, at room temperature for 30 min. The mixture was neutralized with 18.0 mL of 25 mmol/L phosphate-buffered saline (PBS) pH 7.4; this solution was maintained on ice in the dark until use [19]. Briefly, platelets were incubated for 15 min with 5 mM DCFDA-free base at 37˚C. Then the DCFDA treated platelets were divided into two sets: one set was incu- bated with the addition of a mixture of L-arginine 100 mM and NG-monomethyl-L-arginine (L-NMMA) 100 mM for 15 min at 37˚C in the dark while the other set was incubated with the above mentioned mixture but only with PBS. After washing platelets twice in PBS (25 mmol/l) pH 7.4, samples were sonicated to brake platelet pellets. The mixture was then centrifuged at 200 × g for 5 min and the fluorescence was measured in the super- natant in a Perkin-Elmer LS-50B spectrofluorometer, at an excitation wavelength of 475 nm and emission wave- length of 520 nm. Blank samples contained all reagents except platelets. Fluorescence results obtained after L- NMMA incubation were subtracted from those without L-NMMA. ONOO-production was corrected by protein concentration and was expressed in arbitrary fluores- cence numbers/mg prot. 6. TOTAL ANTIOXIDANT CAPACITY (TAC) Total antioxidant capacity was evaluated with a Biovi- sion Assay kit. Biovision has developed a TAC Assay kit which can measure either the combination of both small molecule antioxidants and proteins or small molecules alone in the presence of Protein Mask. Cu2+ ion is con- verted to Cu+ by both small molecules and proteins. The Protein Mask prevents Cu2+ reduction by proteins, ena- bling the analysis of only the small molecule antioxidant. The reduced Cu+ ion is chelated with a colorimetric probe giving a broad absorbance peak of around 570 nm, proportional to the total antioxidant capacity. Aliquots of frozen plasma were thawed at room temperature, and 10 μL of the samples were tested immediately. 10 μL of Protein Mask was added in a plate. The reaction was started directly in the plate with 100 μL of Cu2+ working solution. Plates were covered and incubated at room temperature for 1.5 hours. Trolox, a water-soluble toco- pherol analog, was used as a reference standard. Standard curves were obtained by using increasing concentrations of Trolox in the same volume as for the sample. Absorb- ance was measured with a Hewlett-Packard 8450 A UV/ Visible spectrophotometer equipped with a cuvette stir- ring apparatus and a constant temperature cell holder. Unless stated differently, experiments were repeated 2 to 3 times. Qualitatively, similar results were obtained with individual values varying by less than 8%. In the lag mode, the assay mainly measures nonprotein and nonenzymatic antioxidants that are primarily ex- tracellular chain-breaking ones, such as ascorbate, urate, and glutathione. Plasma Lipid hydroperoxides were evaluated by meas- uring the levels of hydroperoxides using the ferrous oxi- dation xylenol orange assay (FOX-assay) in agreement with our previous studies [20]. Samples were incubated with FOX reagent (100 mmol/L xylenol orange, 250 Copyright © 2013 SciRes. OPEN ACCESS 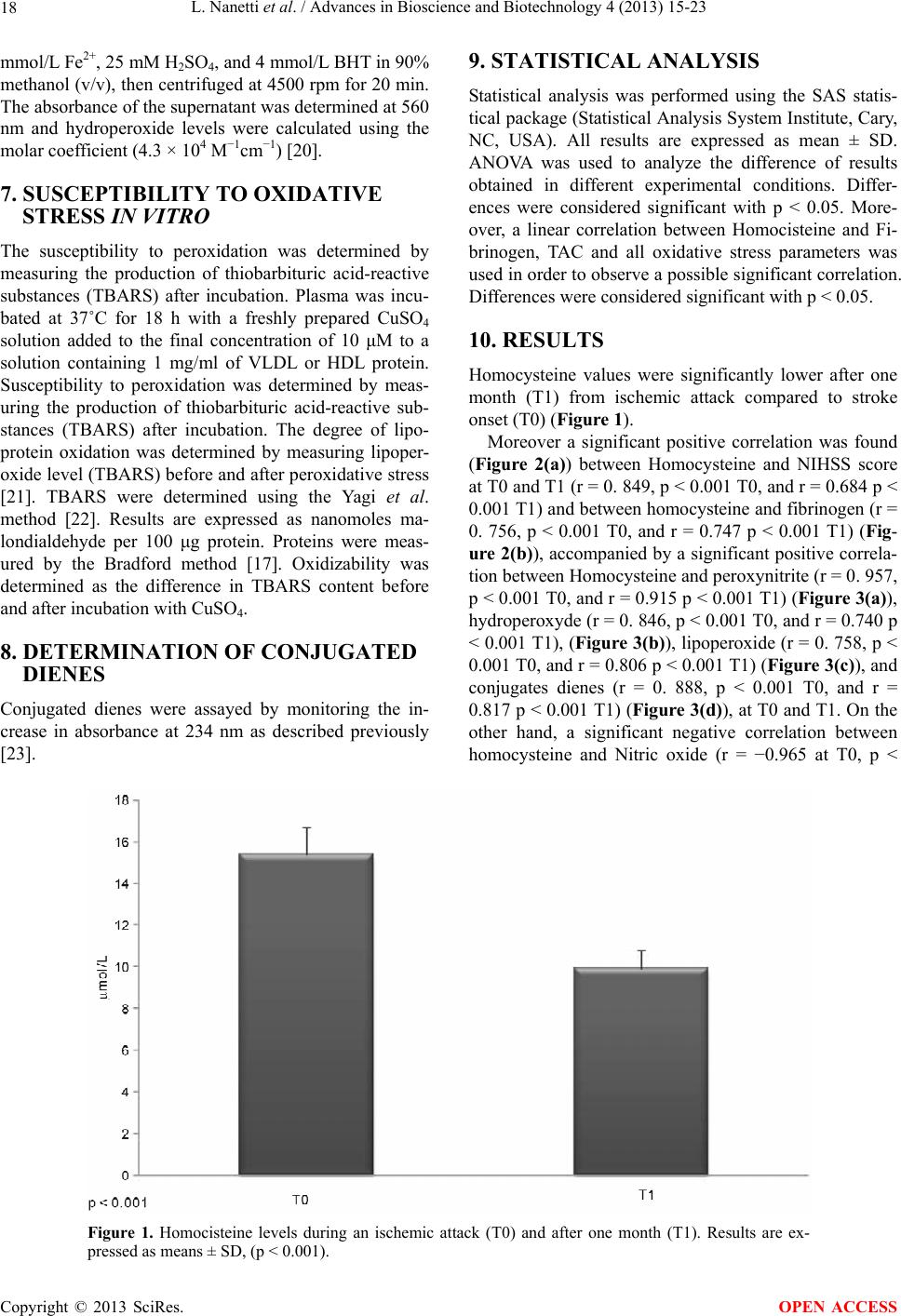 L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 Copyright © 2013 SciRes. 18 9. STATISTICAL ANALYSIS mmol/L Fe2+, 25 mM H2SO4, and 4 mmol/L BHT in 90% methanol (v/v), then centrifuged at 4500 rpm for 20 min. The absorbance of the supernatant was determined at 560 nm and hydroperoxide levels were calculated using the molar coefficient (4.3 × 104 M−1cm−1) [20]. Statistical analysis was performed using the SAS statis- tical package (Statistical Analysis System Institute, Cary, NC, USA). All results are expressed as mean ± SD. ANOVA was used to analyze the difference of results obtained in different experimental conditions. Differ- ences were considered significant with p < 0.05. More- over, a linear correlation between Homocisteine and Fi- brinogen, TAC and all oxidative stress parameters was used in order to observe a possible significant correlation. Differences were considered significant with p < 0.05. 7. SUSCEPTIBILITY TO OXIDATIVE STRESS IN VITRO The susceptibility to peroxidation was determined by measuring the production of thiobarbituric acid-reactive substances (TBARS) after incubation. Plasma was incu- bated at 37˚C for 18 h with a freshly prepared CuSO4 solution added to the final concentration of 10 μM to a solution containing 1 mg/ml of VLDL or HDL protein. Susceptibility to peroxidation was determined by meas- uring the production of thiobarbituric acid-reactive sub- stances (TBARS) after incubation. The degree of lipo- protein oxidation was determined by measuring lipoper- oxide level (TBARS) before and after peroxidative stress [21]. TBARS were determined using the Yagi et al. method [22]. Results are expressed as nanomoles ma- londialdehyde per 100 μg protein. Proteins were meas- ured by the Bradford method [17]. Oxidizability was determined as the difference in TBARS content before and after incubation with CuSO4. 10. RESULTS Homocysteine values were significantly lower after one month (T1) from ischemic attack compared to stroke onset (T0) (Figure 1). Moreover a significant positive correlation was found (Figure 2(a)) between Homocysteine and NIHSS score at T0 and T1 (r = 0. 849, p < 0.001 T0, and r = 0.684 p < 0.001 T1) and between homocysteine and fibrinogen (r = 0. 756, p < 0.001 T0, and r = 0.747 p < 0.001 T1) (Fig- ure 2(b)), accompanied by a significant positive correla- tion between Homocysteine and peroxynitrite (r = 0. 957, p < 0.001 T0, and r = 0.915 p < 0.001 T1) (Figure 3(a)), hydroperoxyde (r = 0. 846, p < 0.001 T0, and r = 0.740 p < 0.001 T1), (Figure 3(b)), lipoperoxide (r = 0. 758, p < 0.001 T0, and r = 0.806 p < 0.001 T1) (Figure 3(c)), and conjugates dienes (r = 0. 888, p < 0.001 T0, and r = 0.817 p < 0.001 T1) (Figure 3(d)), at T0 and T1. On the other hand, a significant negative correlation between homocysteine and Nitric oxide (r = −0.965 at T0, p < 8. DETERMINATION OF CONJUGATED DIENES Conjugated dienes were assayed by monitoring the in- crease in absorbance at 234 nm as described previously [23]. Figure 1. Homocisteine levels during an ischemic attack (T0) and after one month (T1). Results are ex- pressed as means ± SD, (p < 0.001). OPEN ACCESS 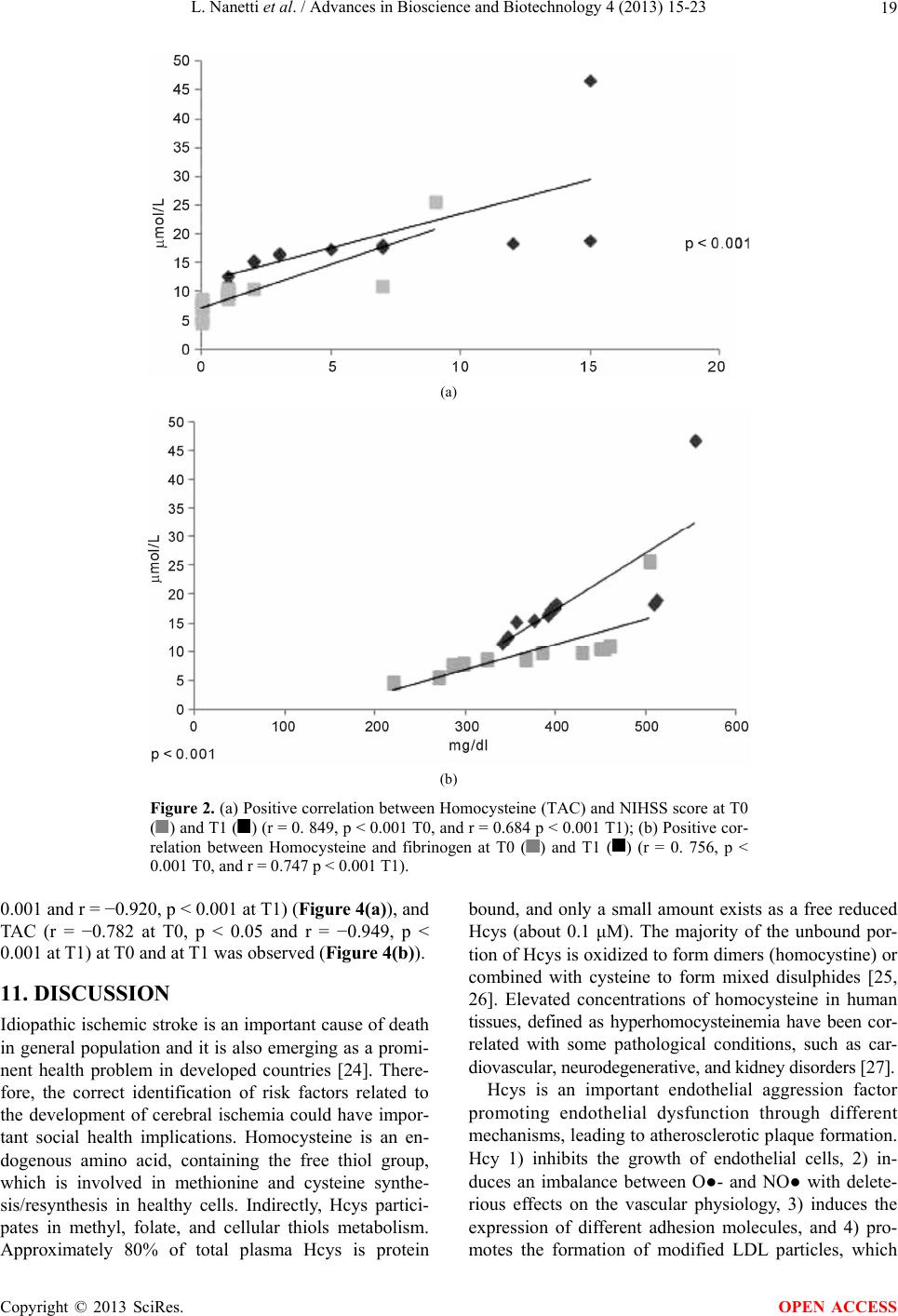 L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 19 (a) (b) Figure 2. (a) Positive correlation between Homocysteine (TAC) and NIHSS score at T0 ( ) and T1 () (r = 0. 849, p < 0.001 T0, and r = 0.684 p < 0.001 T1); (b) Positive cor- relation between Homocysteine and fibrinogen at T0 () and T1 () (r = 0. 756, p < 0.001 T0, and r = 0.747 p < 0.001 T1). 0.001 and r = −0.920, p < 0.001 at T1) (Figure 4(a)), and TAC (r = −0.782 at T0, p < 0.05 and r = −0.949, p < 0.001 at T1) at T0 and at T1 was observed (Figure 4(b)). 11. DISCUSSION Idiopathic ischemic stroke is an important cause of death in general population and it is also emerging as a promi- nent health problem in developed countries [24]. There- fore, the correct identification of risk factors related to the development of cerebral ischemia could have impor- tant social health implications. Homocysteine is an en- dogenous amino acid, containing the free thiol group, which is involved in methionine and cysteine synthe- sis/resynthesis in healthy cells. Indirectly, Hcys partici- pates in methyl, folate, and cellular thiols metabolism. Approximately 80% of total plasma Hcys is protein bound, and only a small amount exists as a free reduced Hcys (about 0.1 μM). The majority of the unbound por- tion of Hcys is oxidized to form dimers (homocystine) or combined with cysteine to form mixed disulphides [25, 26]. Elevated concentrations of homocysteine in human tissues, defined as hyperhomocysteinemia have been cor- related with some pathological conditions, such as car- diovascular, neurodegenerative, and kidney disorders [27]. Hcys is an important endothelial aggression factor promoting endothelial dysfunction through different mechanisms, leading to atherosclerotic plaque formation. Hcy 1) inhibits the growth of endothelial cells, 2) in- duces an imbalance between O●- and NO● with delete- rious effects on the vascular physiology, 3) induces the expression of different adhesion molecules, and 4) pro- otes the formation of modified LDL particles, which m Copyright © 2013 SciRes. OPEN ACCESS 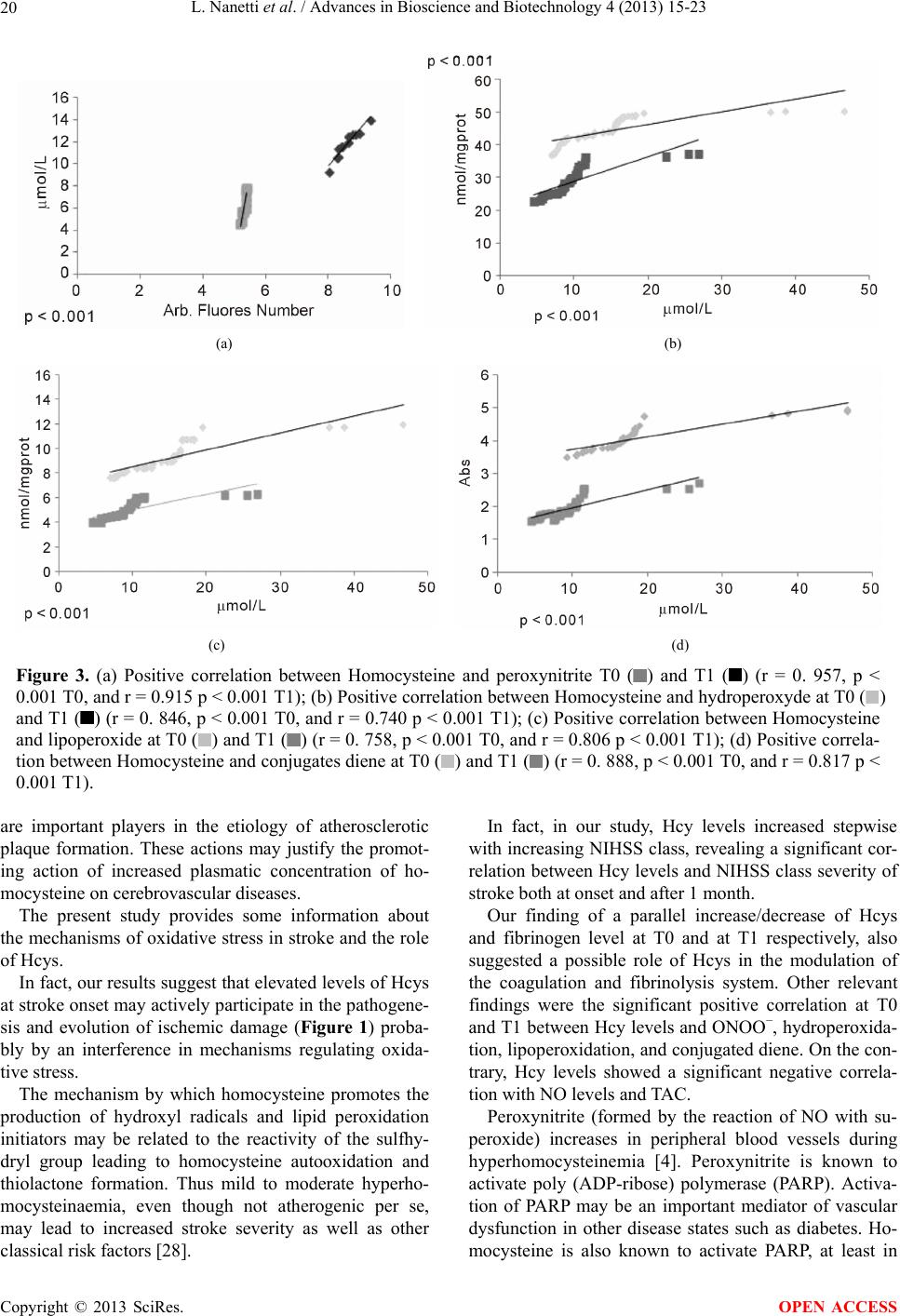 L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 20 (a) (b) (c) (d) Figure 3. (a) Positive correlation between Homocysteine and peroxynitrite T0 () and T1 () (r = 0. 957, p < 0.001 T0, and r = 0.915 p < 0.001 T1); (b) Positive correlation between Homocysteine and hydroperoxyde at T0 () and T1 () (r = 0. 846, p < 0.001 T0, and r = 0.740 p < 0.001 T1); (c) Positive correlation between Homocysteine and lipoperoxide at T0 ( ) and T1 ( ) (r = 0. 758, p < 0.001 T0, and r = 0.806 p < 0.001 T1); (d) Positive correla- tion between Homocysteine and conjugates diene at T0 () and T1 () (r = 0. 888, p < 0.001 T0, and r = 0.817 p < 0.001 T1). are important players in the etiology of atherosclerotic plaque formation. These actions may justify the promot- ing action of increased plasmatic concentration of ho- mocysteine on cerebrovascular diseases. The present study provides some information about the mechanisms of oxidative stress in stroke and the role of Hcys. In fact, our results suggest that elevated levels of Hcys at stroke onset may actively participate in the pathogene- sis and evolution of ischemic damage (Figure 1) proba- bly by an interference in mechanisms regulating oxida- tive stress. The mechanism by which homocysteine promotes the production of hydroxyl radicals and lipid peroxidation initiators may be related to the reactivity of the sulfhy- dryl group leading to homocysteine autooxidation and thiolactone formation. Thus mild to moderate hyperho- mocysteinaemia, even though not atherogenic per se, may lead to increased stroke severity as well as other classical risk factors [28]. In fact, in our study, Hcy levels increased stepwise with increasing NIHSS class, revealing a significant cor- relation between Hcy levels and NIHSS class severity of stroke both at onset and after 1 month. Our finding of a parallel increase/decrease of Hcys and fibrinogen level at T0 and at T1 respectively, also suggested a possible role of Hcys in the modulation of the coagulation and fibrinolysis system. Other relevant findings were the significant positive correlation at T0 and T1 between Hcy levels and ONOO−, hydroperoxida- tion, lipoperoxidation, and conjugated diene. On the con- trary, Hcy levels showed a significant negative correla- tion with NO levels and TAC. Peroxynitrite (formed by the reaction of NO with su- peroxide) increases in peripheral blood vessels during hyperhomocysteinemia [4]. Peroxynitrite is known to activate poly (ADP-ribose) polymerase (PARP). Activa- tion of PARP may be an important mediator of vascular dysfunction in other disease states such as diabetes. Ho- ocysteine is also known to activate PARP, at least in m Copyright © 2013 SciRes. OPEN ACCESS 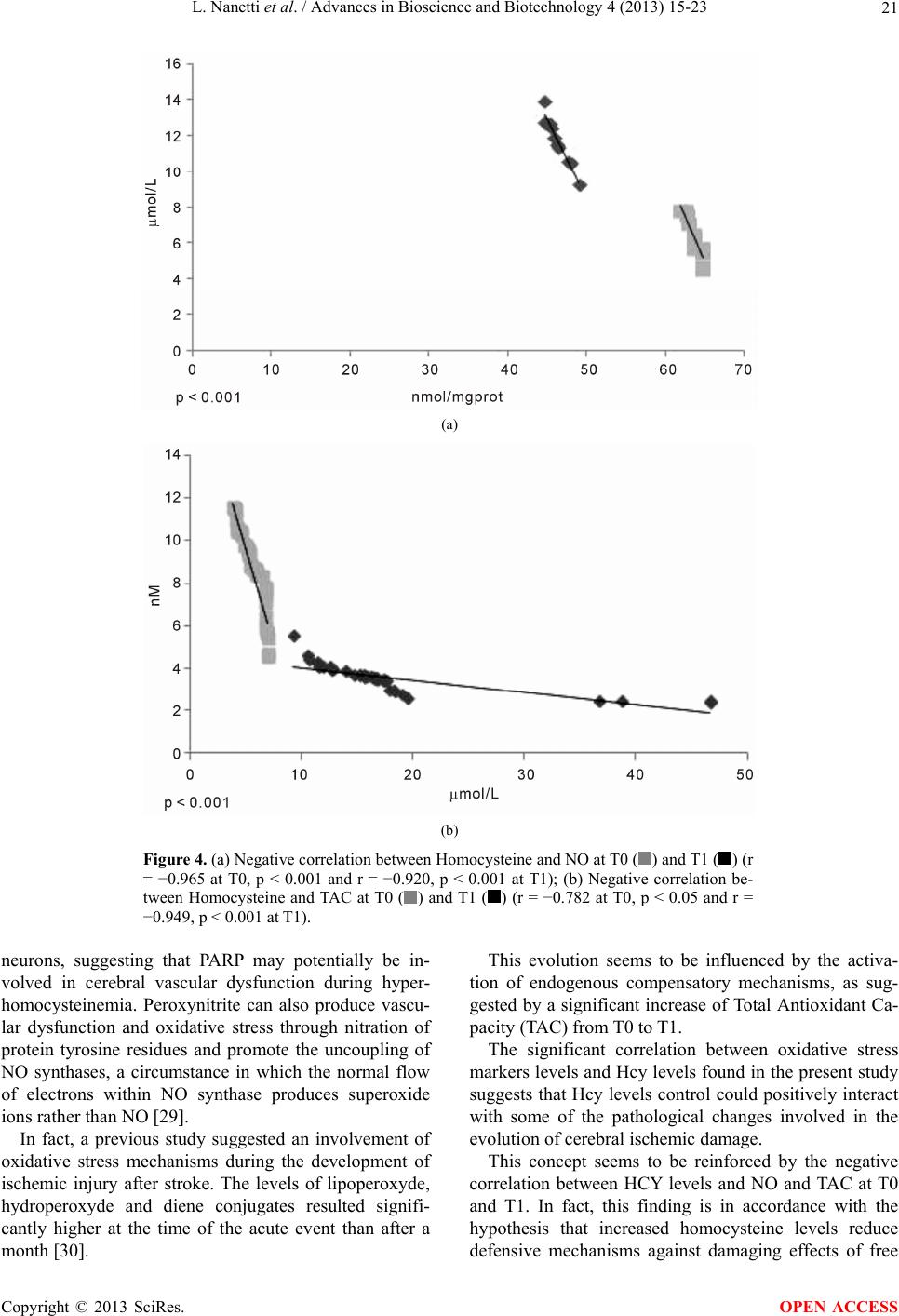 L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 21 (a) (b) Figure 4. (a) Negative correlation between Homocysteine and NO at T0 () and T1 () (r = −0.965 at T0, p < 0.001 and r = −0.920, p < 0.001 at T1); (b) Negative correlation be- tween Homocysteine and TAC at T0 () and T1 () (r = −0.782 at T0, p < 0.05 and r = −0.949, p < 0.001 at T1). neurons, suggesting that PARP may potentially be in- volved in cerebral vascular dysfunction during hyper- homocysteinemia. Peroxynitrite can also produce vascu- lar dysfunction and oxidative stress through nitration of protein tyrosine residues and promote the uncoupling of NO synthases, a circumstance in which the normal flow of electrons within NO synthase produces superoxide ions rather than NO [29]. In fact, a previous study suggested an involvement of oxidative stress mechanisms during the development of ischemic injury after stroke. The levels of lipoperoxyde, hydroperoxyde and diene conjugates resulted signifi- cantly higher at the time of the acute event than after a month [30]. This evolution seems to be influenced by the activa- tion of endogenous compensatory mechanisms, as sug- gested by a significant increase of Total Antioxidant Ca- pacity (TAC) from T0 to T1. The significant correlation between oxidative stress markers levels and Hcy levels found in the present study suggests that Hcy levels control could positively interact with some of the pathological changes involved in the evolution of cerebral ischemic damage. This concept seems to be reinforced by the negative correlation between HCY levels and NO and TAC at T0 and T1. In fact, this finding is in accordance with the hypothesis that increased homocysteine levels reduce defensive mechanisms against damaging effects of free Copyright © 2013 SciRes. OPEN ACCESS  L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 22 radicals. In conclusion, our data, obtained in a subgroup of pa- tients with large-artery stroke, suggest an involvement of homocysteine in the pathogenesis of ischemic damage. In this respect, besides the possible use of hyper-Hcy as a prognostic marker, acute therapeutic interventions aimed at modulating Hcy levels should be considered as a fur- ther therapeutic strategy in patients with ischemic stroke, in the attempt to positively interfere with the biochemical mechanisms involved inoxidative stress. REFERENCES [1] Hankey, G.J. and Eikelboom, J.W. (1999) Homocysteine and vascular disease. Lancet, 354, 407-413. http://dx.doi.org/10.1016/S0140-6736(98)11058-9 [2] Durand, P., Prost, M., Loreau, N., Lussier-Cacan, S. and Blache, D. (2001) Impaired homocysteine metabolism and atherothrombotic disease. Laboratory Investigation, 81, 645-672. http://dx.doi.org/10.1038/labinvest.3780275 [3] McCully, K.S. (1969) Vascular pathology of homocys- teinemia: Implications for the pathogenesis of arterioscle- rosis. The American Journal of Pathology, 56, 111-128. [4] Faraci, F.M. and Lentz, S.R. (2004) Hyperhomocystei- nemia, oxidative stress, and cerebral vascular dysfunction. Stroke, 35, 345-347. http://dx.doi.org/10.1161/01.STR.0000115161.10646.67 [5] Homocystein Studies Collaboration (2002) Homocysteine and risk of ischemic heart disease and stroke: A meta- analysis. JAMA, 288, 2015-2022. http://dx.doi.org/10.1001/jama.288.16.2015 [6] Klerk, M., Verhoef, P., Clarke, R., Blom, H.J., Kok, F.J., Schouten, E.G., MTHFR Studies Collaboration Group (2002) MTHFR 677CT polymorphism and risk of coro- nary heart disease: A meta-analysis. JAMA, 288, 2023- 2031. http://dx.doi.org/10.1001/jama.288.16.2023 [7] Towfighi, A., Markovic, D. and Ovbiagele, B. (2010) Pro- nounced association of elevated serum homocysteine with stroke insubgroups of individuals: A nationwide study. Journal of the Neurological Sciences, 298, 153-157. http://dx.doi.org/10.1016/j.jns.2010.07.013 [8] Nanetti, L., Giannubilo, S.R., Raffaelli, F., Curzi, C.M., Vignini, A., Moroni, C., Tanase, L., Carboni, E., Turi, A., Mazzanti, L. and Tranquilli, A.L. (2008) Nitric oxide and peroxynitrite platelet levels in women with small-for- gestational-age fetuses. BJOG, 115, 14-21. http://dx .doi.org/1 0.1111/j.1471-0528.2007.01567.x [9] Nanetti, L., Moroni, C., Vignini, A., Vannini, P., Fran- ceschi, C. and Mazzanti, L. (2005) Age-related changes on platelet membrane: A study on elderly and centenarian monozygotic twins. Experimental Gerontology, 40, 519- 525. [10] Adams, H.P., Kappelle, L.J., Biller, J., Gordon, D.L., Love, B.B. and Gomez, F. (1995) Ischemic stroke in young adults. Experience in 329 patients enrolled in the Iowa Registry of stroke in young adults. Archives of Neurol- ogy, 52, 491-495. http://dx.doi.org/10.1001/archneur.1995.00540290081021 [11] Aho, K., Harmsen, P. and Hatano, S. (1980) Cerebrovas- cular disease in the community: Results of a WHO col- laborative study. Bulletin of the WHO, 58, 113-130. [12] Taffi, R., Nanetti, L., Mazzanti, L., Bartolini, M., Vignini, A., Raffaelli, F., Provinciali, L. and Silvestrini, M. (2008) Plasma levels of nitric oxide and stroke outcome. Journal of Neurology, 255, 94-98. http://dx.doi.org/10.1007/s00415-007-0700-y [13] Vignini, A., Nanetti, L., Raffaelli, F., Petrini, F., Tiano, L., Littarru, G.P. and Mazzanti, L. (2008) Effect of sup- plementation with fortified olive oil on biochemical mar- kers of bone turnover in healthy women. Mediterranean Journal of Nutrition and Metabolism, 2, 117-120. http://dx.doi.org/10.1007/s12349-008-0015-2 [14] Sun, J., Zhang, X., Broderick, M. and Fein, H. (2003) Measurement of nitric oxide production in biological systems by using Griess reaction assay. Sensors, 3, 276- 284. http://dx.doi.org/10.3390/s30800276 [15] Guevara, I., Iwanejko, J., Dembińska-Kieć, A., Pankie- wicz, J., Wanat, A. and Anna, P. (1998) Determination of nitrite/nitrate in human biological material by the simple Griess reaction. Clinica Chimica Acta, 274, 177-188. http://dx.doi.org/10.1016/S0009-8981(98)00060-6 [16] Moshage, H., Kok, B., Huizenga, J.R. and Jansen, P.L.M. (1995) Nitrite and nitrate determinations in plasma: A critical evaluation. Clinical Chemistry, 41, 892-896. [17] Bradford, M. (1975) A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Analytical Bioche- mistry, 72, 248-254. http://dx.doi.org/10.1016/0003-2697(76)90527-3 [18] Vignini, A., Nanetti, L., Moroni, C., Tanase, L., Bartolini, M., Luzzi, S., Provinciali, L. and Mazzanti, L. (2007) Mo- difications of platelet from Alzheimer disease patients: A possible relation between membrane properties and NO metabolites. Neurobiology of Aging, 28, 987-994. http://dx.doi.org/10.1016/j.neurobiolaging.2006.05.010 [19] Nanetti, L., Taffi, R., Vignini, A., Moroni, C., Raffaelli, F., Bacchetti, T. and Mazzanti, L. (2007) Reactive oxy- gen species plasmatic levels in ischemic stroke. Molecu- lar and Cellular Biochemistry, 303, 19-25. http://dx.doi.org/10.1007/s11010-007-9451-4 [20] Ferretti, G., Bacchetti, T., Moroni, C., Vignini, A., Na- netti, L. and Curatola, G. (2004) Effect of homocystei- nylation of low density lipoproteins on lipid peroxidation of human endothelial cells. Journal of Cellular Bioche- mistry, 92, 351-360. http://dx.doi.org/10.1002/jcb.20069 [21] Rabini, R.A., Fumelli, P., Galassi, R., Dousset, N., Taus, M., Ferretti, G., Mazzanti, L., Curatola, G., Solera, M.L. and Valdiguié, P. (1994) Increased susceptibility to lipid oxidation of low-density lipoproteins and erythrocyte mem- branes from diabetic patients. Metabolism, 43, 1470-1474. http://dx.doi.org/10.1016/0026-0495(94)90003-5 [22] Yagi, K. (1994) Lipid peroxides and related radicals in clinical medicine. Advances in Experimental Medicine & Biology, 366, 1-15. http://dx.doi.org/10.1007/978-1-4615-1833-4_1 Copyright © 2013 SciRes. OPEN ACCESS  L. Nanetti et al. / Advances in Bioscience and Biotechnology 4 (2013) 15-23 Copyright © 2013 SciRes. 23 OPEN ACCESS [23] Esterbauer, H., Gebicki, J., Puhl, H. and Jürgens, G. (1992) The role of lipid peroxidation and antioxidants in oxidative modification of LDL. Free Radical Biology & Medicine, 13, 341-349. http://dx.doi.org/10.1016/0891-5849(92)90181-F [24] Dragoni, F., Chiarotti, F., Rosano, G., Simioni, P., Tor- mene, D., Mazzucconi, M.G., Cafolla, A. and Avvisati, G. (2011) Thrombophilic screening in young patients (<40 years) with idiopathic ischemic stroke: A controlled study. Thrombosis Research, 127, 85-90. http://dx.doi.org/10.1016/j.thromres.2010.11.013 [25] Dietrich-Muszalska, A., Malinowska, J., Olas, B., Gło- wacki, R., Bald, E., Wachowicz, B. and Rabe-Jabłońska, J. (2012) The oxidative stress may be induced by the ele- vated homocysteine in schizophrenic patients. Neuroche- mical Research, 37, 1057-1062. http://dx.doi.org/10.1007/s11064-012-0707-3 [26] Ramakrishnan, S., Sulochana, K.N., Lakshm, S., Selvi, R. and Angayarkanni, K. (2006) Biochemistry of homocys- teine in health and diseases. Indian Journal of Biochem- istry & Biophysics, 43, 275-283. [27] Manolescu, B.N., Oprea, E., Farcasanu, I.C., Berteanu, M. and Cercasov, C. (2010) Homocysteine and vitamin ther- apy in stroke prevention and treatment: A review. Acta Biochimica Polonica, 57, 467-477. [28] Nanetti, L., Vignini, A., Raffaelli, F., Moroni, C., Silves- trini, M., Provinciali, L. and Mazzanti, L. (2008) Platelet membrane fluidity and Na+/K+ ATPase activity in acute stroke. Brain Research, 1205, 21-26. http://dx.doi.org/10.1016/j.brainres.2008.02.005 [29] Faraci, F.M. (2003) Hyperhomocysteinemia: A million ways to lose control. Arteriosclerosis, Thrombosis, and Vascular Biology, 23, 371-373. http://dx.doi.org/10.1161/01.ATV.0000063607.56590.7F [30] Nanetti, L., Raffaelli, F., Vignini, A., Perozzi, C., Silves- trini, M., Bartolini, M., Mazzanti, L. and Provinciali, L. (2011) Oxidative stress in ischaemic stroke. European Journal of Clinical Investigation, 41, 1318-1322. http://dx .doi.org/1 0.1111/j.1365-2362.2011.02546.x
|