Journal of Cancer Therapy, 2013, 4, 1426-1428
Published Online November 2013 (http://www.scirp.org/journal/jct)
http://dx.doi.org/10.4236/jct.2013.49169
Open Access JCT
Do All Prostate Cancers Behave the Same?
Dissanayake Thusitha1*, Arze Elizabeth2, Rogers Mailien3
1Department of Internal Medicine, James H. Quillen College of Medicine, East Tennessee State University, Johnson City, USA;
2Department of Pathology, James H. Quillen College of Medicine, East Tennessee State University, Johnson City, USA; 3Division of
Hematology-Oncology, James H. Quillen College of Medicine, East Tennessee State University, Johnson City, USA.
Email: *thusithard007@gmail.com
Received August 27th, 2013; revised September 25th, 2013; accepted October 3rd, 2013
Copyright © 2013 Dissanayake Thusitha et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Two different immunohistochemical types suggestive of Large Cell Neuroendocrine (NE) carcinoma and Adenocarci-
noma in a patient with known diffusely metastatic, ho rmone refractory prostate carcinoma are rarities. Interestingly, our
patient had documented history of exposure to Agent Orange during his time of service. The use of routinely used im-
munohistochemical stains for pathological diagnosis was a challenge in this case, though throughout his disease course,
the diagnosis was confirmed as Adenocarcinoma of prostate with biopsies from all various sites of metastases. Systemic
chemotherapy has been historically suboptimal in management of aggressively behaved prostate carcinomas. Finding
any association of Agent Orange as a causative etiology and improving diagnosis and management of such aggressive
hormone refractory prostate carcinoma need further investigations.
Keywords: Large Cell Neuroendocrine Carcinoma; Adenocarcinoma of Prostate; Hormone Refractory Prostate
Carcinoma; Agent Orange
1. Introduction
A 62-year-old white male was diagnosed with metastatic
hormone refractory adenocarcinoma of prostate and was
treated with luteinizing hormone releasing hormone ago-
nist. The patient gave a history of melanoma and remote
history of tobacco abuse. Several months after treatment
was initiated, the patient was presented to the emergency
room for stroke like symptoms and was found to have
brain metastases secondary to his prostate.
Further workup revealed a mediastinal lymph node
wi th inconclusive biopsy result for a primary though adeno-
carcinoma was primarily suspected.
We present an interesting yet complicated case raising
the question of prostate cancer with exposure to Agent
Orange, to which our patient was exposed during the
Vietnam War.
2. Case Report and Discussion
A Vietnam veteran was originally diagnosed with Stage
IV Prostate Adenocarcinoma July 2011 when he pre-
sented with new onset urinary retention.
He underwent cystoscopy July 26th, 2011 and 4 out of
4 core biopsies were reported as adenocarcinoma of
prostate with Gleason score of 8.
His bone scan showed extensive bony metastases.
At the time of diagnosis, his PSA was only mildly
elevated at 5.66. He was started on an drogen depriv ation
therapy (ADT) with Zoladex in jections.
In November 2011, patient presented to VA ER with
vomiting and left sided weakness. On suspicion of cere-
bral vascular accident, CT scanning revealed a 4-cm right
frontal white matter centrally necrotic mass with sur-
rounding vasogenic edema. He was transferred to local
level 4 tertiary care center and brain biopsy performed.
Due to rarity of adenocarcinoma of prostate metasta-
sizing to the brain, search for more common sources
were sought. Further investigation proved his history of
melanoma was actually squamous cell but due to history
of smoking, lung primary was also a possibility.
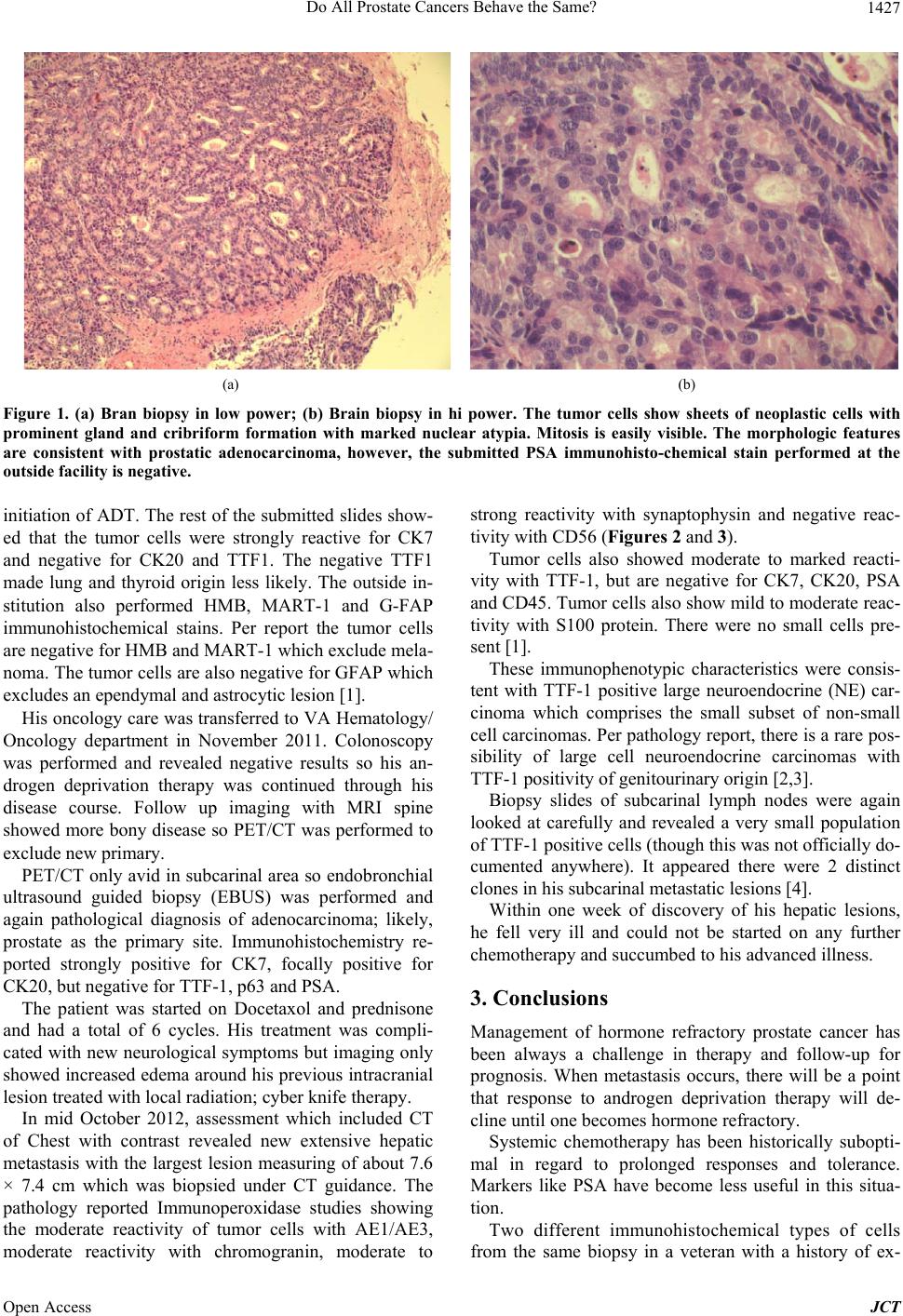
Pathology of brain biopsies reported as tumor cells
showing sheets of neoplastic cells with prominent gland
and cruciform formation with marked nuclear atypia with
easily visible mitosis. The morphological features were
consistent with prostate adenocarcinoma per pathology
report (Figures 1(a) and (b)).
The submitted PSA immunohistochemical stains at the
outside facility were negative which is common after
*Corresponding aut hor.