Y. K. LEE ET AL.
6
6. Conclusion
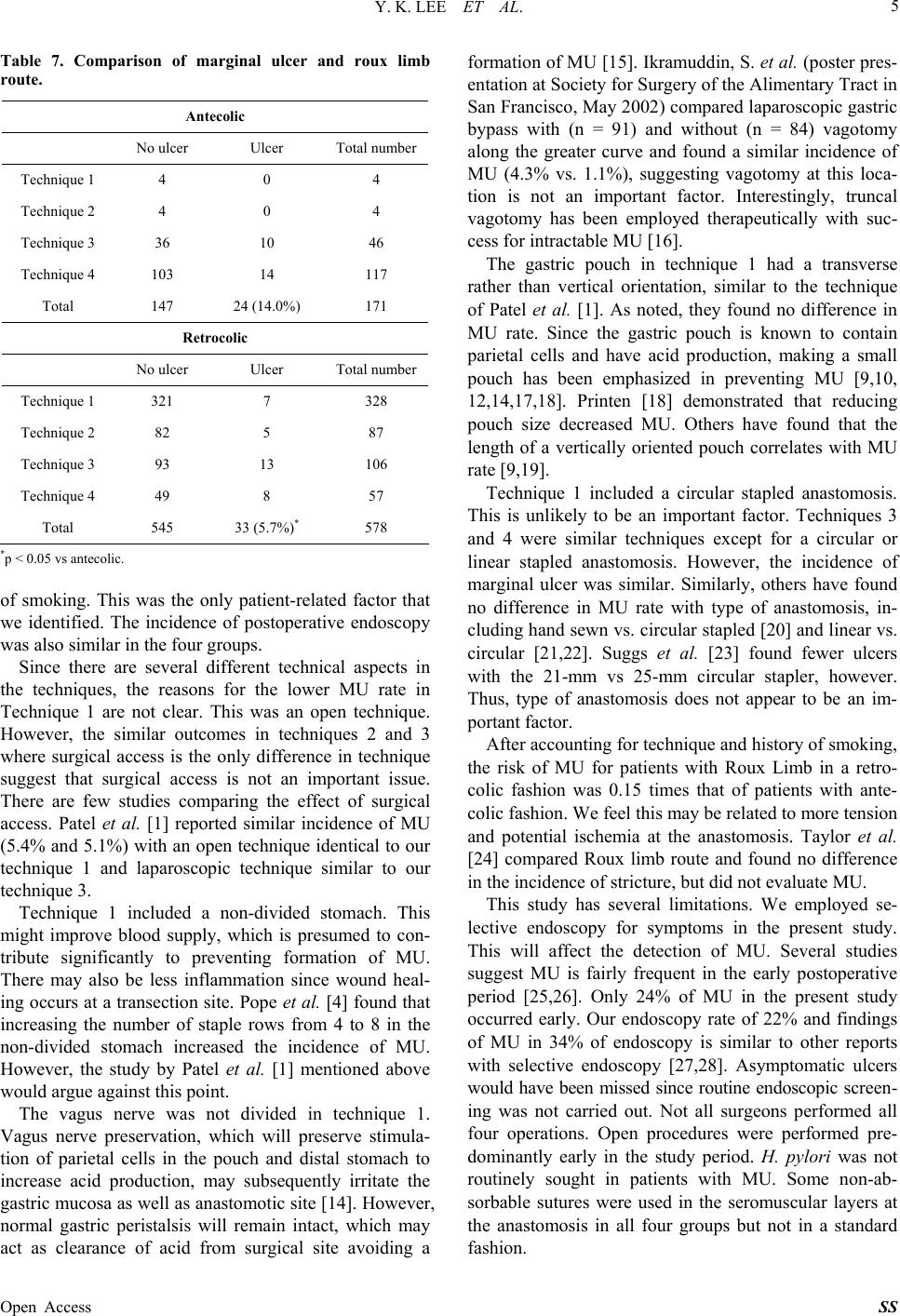
In conclusion, the incidence of MU after RGBP surgery
is influenced by surgical technique. The overall 7.5%
incidence of MU is consistent with other studies. The
lowest incidence of MU was the technique with a non-
divided stomach, no vagotomy, and a circular anastomo-
sis. A retrocolic Roux limb was protective. There was no
difference of MU using linear or circular stapler for the
gastrojejunostomy and no difference in laparoscopic ver-
sus open bypass if a similar technique was employed.
REFERENCES
[1] R. A. Patel, R. E. Brolin and A. Gandhi, “Revisional Ope-
rations for Marginal Ulcer after Roux-en-Y Gastric By-
pass,” Surgery for Obesity and Related Diseases, Vol. 5,
No. 3, 2009, pp. 317-322.
http://dx.doi.org/10.1016/j.soard.2008.10.011
[2] L. D. MacLean, B. M. Rhode, C. Nohr, S. Katz and A. P.
McLean, “Stomal Ulcer after Gastric Bypass,” Journal of
the American College of Surgeons, Vol. 185, No. 1, 1997,
pp. 1-7.
http://dx.doi.org/10.1016/S1072-7515(01)00873-0
[3] J. F. Capella and R. F. Capella, “Gastro-Gastric Fistulas
and Marginal Ulcers in Gastric Bypass Procedures for
Weight Reduction,” Obesity Surgery, Vol. 9, No. 1, 1999,
pp. 22-27.
http://dx.doi.org/10.1381/096089299765553674
[4] G. D. Pope, P. P. Goodney, K. W. Burchard, R. R. Proia,
A. Olafsson, B. E. Lacy and L. J. Burrows, “Peptic Ul-
cer/Stricture after Gastric Bypass: A Comparison of Tech-
nique and Acid Suppression Variables,” Obesity Surgery,
Vol. 12, No. 1, 2002, pp. 30-33.
http://dx.doi.org/10.1381/096089202321144540
[5] B. C. Sacks, S.G. Mattar, F.G. Qureshi, G.M. Eid, J.L.
Collins, E.J. Barinas-Mitchell, P.R. Schauer and R.C.
Ramanathan, “Incidence of Marginal Ulcers and the Use
of Absorbable Anastomotic Sutures in Laparoscopic Roux-
en-Y Gastric Bypass,” Surgery for Obesity and Related
Diseases, Vol. 2, No. 1, 2006, pp. 11-16.
http://dx.doi.org/10.1016/j.soard.2005.10.013
[6] R. M. Dallal and L. A. Bailey, “Ulcer Disease after Gas-
tric Bypass Surgery,” Surgery for Obesity and Related
Diseases, Vol. 2, No. 4, 2006, pp. 455-459.
http://dx.doi.org/10.1016/j.soard.2006.03.004
[7] A. A. Gumbs, A. J. Duffy and R. L. Bell, “Incidence and
Management of Marginal Ulceration after Laparoscopic
Roux-Y Gastric Bypass,” Surgery for Obesity and Re-
lated Diseases, Vol. 2, No. 4, 2006, pp. 460-463.
http://dx.doi.org/10.1016/j.soard.2006.04.233
[8] J. A. Wilson, J. Romagnuolo, T. K. Byrne, K. Morgan
and F. A. Wilson, “Predictors of Endoscopic Findings af-
ter Roux-en-Y Gastric Bypass,” The American Journal of
Gastroenterology, Vol. 101, No. 10, 2006, pp. 2194-
2199.
http://dx.doi.org/10.1111/j.1572-0241.2006.00770.x
[9] J. H. Jordan, M. P. Hocking, W. R. Rout and E. R. Wood-
ward, “Marginal Ulcer Following Gastric Bypass for Mor-
bid Obesity,” The American Surgeon, Vol. 57, No. 5, 1991,
pp. 286-288.
[10] J. A. Sapala, M. H. Wood, M. A. Sapala and T. M. Flake
Jr., “Marginal Ulcer after Gastric Bypass: A Prospective
3-Year Study of 173 Patients,” Obesity Surgery, Vol. 8,
No. 5, 1998, pp. 505-516.
http://dx.doi.org/10.1381/096089298765554061
[11] E. E. Frezza, H. Herbert, R. Ford and M. S. Wachtel, “En-
doscopic Suture Removal at Gastrojejunal Anastomosis
after Roux-en-Y Gastric Bypass to Prevent Marginal Ul-
ceration,” Surgery for Obesity and Related Diseases, Vol.
3, No. 6, 2007, pp. 619-622.
http://dx.doi.org/10.1016/j.soard.2007.08.019
[12] J. Hedberg, H. Hedenstrom, S. Nilsson, M. Sundbom and
S. Gustavsson, “Role of Gastric Acid in Stomal Ulcer af-
ter Gastric Bypass,” Obesity Surgery, Vol. 15, No. 10,
2005, pp. 1375-1378.
http://dx.doi.org/10.1381/096089205774859380
[13] C. S. Yang, W. J. Lee, H. H. Wang, S. P. Huang, J. T. Lin
and M. S. Wu, “The Influence of Helicobacter Pylori In-
fection on the Development of Gastric Ulcer in Sympto-
matic Patients after Bariatric Surgery,” Obesity Surgery,
Vol. 16, No. 6, 2006, pp. 735-739.
http://dx.doi.org/10.1381/096089206777346754
[14] H. Siilin, A. Wanders, S. Gustavsson and M. Sundbom,
“The Proximal Gastric Pouch Invariably Contains Acid-
Producing Parietal Cells in Roux-en-Y Gastric Bypass,”
Obesity Surgery, Vol. 15, No. 6, 2005, pp. 771-777.
http://dx.doi.org/10.1381/0960892054222849
[15] J. A. Sapala, M. H. Wood and M. P. Schuhknecht, “Va-
gotomy at the Time of Gastric Bypass: Can It Be Harm-
ful?” Obesity Surgery, Vol. 14, No. 5, 2004, pp. 575-576.
http://dx.doi.org/10.1381/096089204323093327
[16] J. Hunter, R. D. Stahl, M. Kakade, I. Breitman, J. Grams
and R. H. Clements, “Effectiveness of Thoracoscopic
Truncal Vagotomy in the Treatment of Marginal Ulcers
after Laparoscopic Roux-en-Y Gastric Bypass,” The Ame-
rican Surgeon, Vol. 78, No. 6, 2012, pp. 663-668.
[17] E. E. Mason, J. R. Munns, G. P. Kealey, R. Wangler, W.
R. Clarke, H. F. Cheng and K. J. Printen, “Effect of Gas-
tric Bypass on Gastric Secretion,” American Journal of
Surgery, Vol. 131, No. 2, 1976, pp. 162-168.
http://dx.doi.org/10.1016/0002-9610(76)90090-8
[18] K. J. Printen, D. Scott and E. E. Mason, “Stomal Ulcers
after Gastric Bypass,” Archives of Surgery, Vol. 115, No.
4, 1980, pp. 525-527.
http://dx.doi.org/10.1001/archsurg.1980.01380040147026
[19] D. E. Azagury, B. K. Abu Dayyeh, I. T. Greenwalt and C.
C. Thompson, “Marginal Ulceration after Roux-en-Y Gas-
tric Bypass Surgery: Characteristics, Risk Factors, Treat-
ment and Outcomes,” Endoscopy, Vol. 43, No. 11, 2011,
pp. 950-954. http://dx.doi.org/10.1055/s-0030-1256951
[20] R. Gonzalez, E. Lin, K. R. Venkatesh, S. P. Bowers and
C. D. Smith, “Gastrojejunostomy during Laparoscopic
Gastric Bypass: Analysis of 3 Techniques,” Archives of
Surgery, Vol. 138, No. 2, 2003, pp. 181-184.
[21] F. P. Bendewald, J. N. Choi, L. S. Blythe, D. J. Selzer, J.
H. Ditslear and S. G. Mattar, “Comparison of Hand-Sewn,
Linear-Stapled, and Circular-Stapled Gastrojejunostomy
Open Access SS