S. AGARWAL ET AL.
288
symptoms include blood mixed nasal discharge, head-
ache, facial pain, frequent clearing of throat, decreased or
loss of smell, epiphora or symptoms suggestive of sinusi-
tis. Inverted papilloma generally occurs unilateral, but
the bilateral involvement of the sinonasal tract has been
reported in less than 1% to 9% patients [19-21 ].
The diagnosis must start by a detailed examination,
investigating environmental exposure, noxious habits,
allergies and associated diseases, and by complete otorhi-
nolaryngological exam. Endoscopic evaluation and ra-
diological (CT and MRI) examinations are required for
tumor study and diagnosis. Biopsy together with histo-
pathology establishes the diagnosis. A unilateral mass
within the nasal cavity or paranasal sinuses with a sur-
face configuration that appears lobulated on CT is a new
sign that strongly suggests inverted papilloma as a pri-
mary diagnosis and also suggests inverted papilloma in
patients with tumor recurrence.
A columnar pattern is a reliable MRI indicator of IP
and reflects its histological architecture (positive predic-
tive value of 95.8%). The combination of this finding
with the absence of extended bone ero sion allows for the
confident discrimination of IPs from malignant tumours
[22].
Complete surgical removal is the first option for the
treatment of IP and is superior to radiation or chemo-
therapy [23,24]. Lateral rhinotomy has been regarded as
the traditional standard surgical approach to control IP
and to avoid recurrence [25]. It gives a good overview
and wide access to the surgical field and can also be per-
formed bilaterally [26]. Alternative techniques are the
midface degloving procedure & Denker’s approach. The
most recent developments in surgery are minimally inva-
sive transnasal endoscopic techniques [27,28]. In endo-
scopically accessible locations, recurrence rates for en-
doscopic vs. open surgery were similar [29]. However,
other studies reported higher recurrence rates of IP [30],
particularly in cases of peripheral extension, especially
into the maxillary sinus [31].
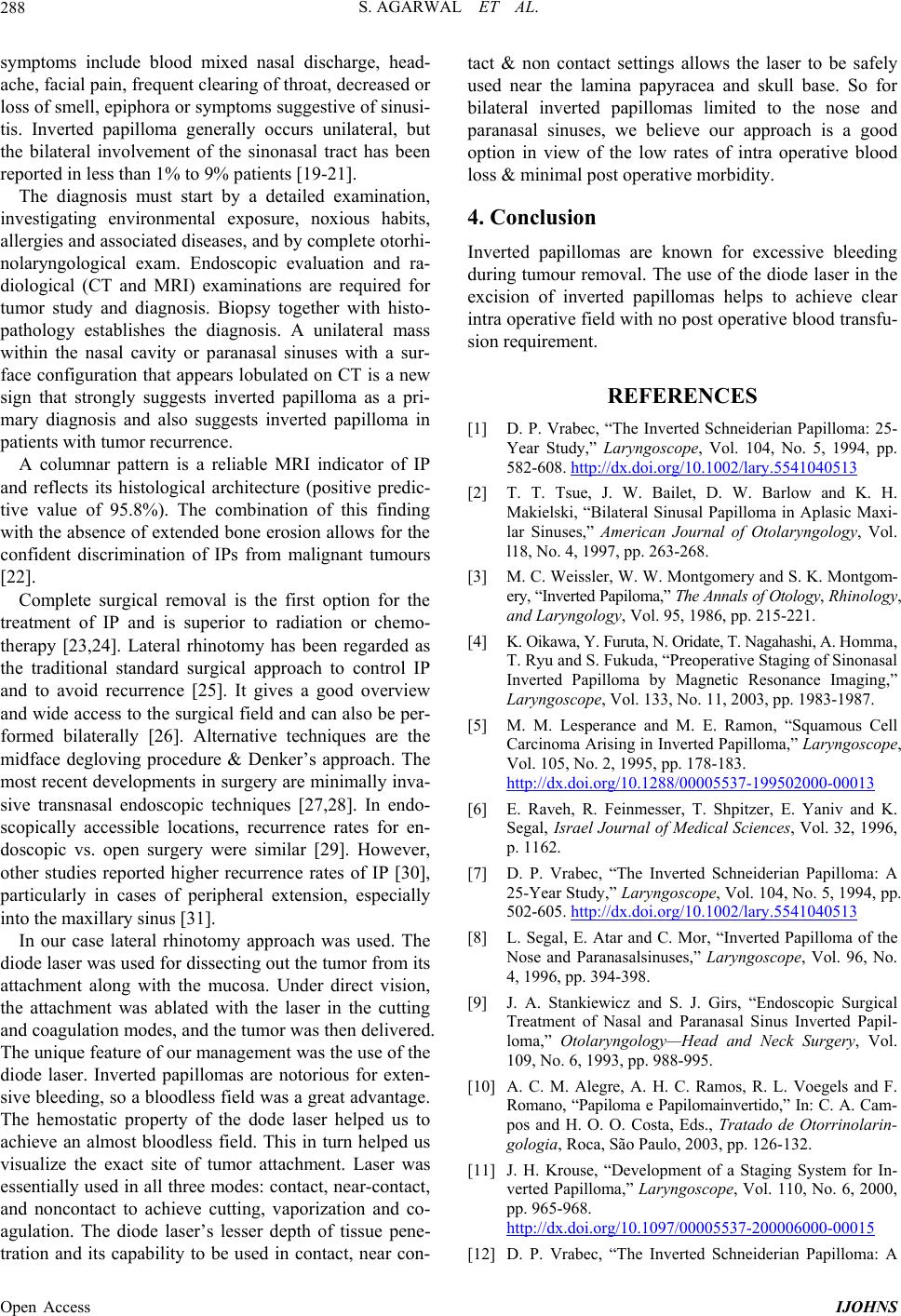
In our case lateral rhinotomy approach was used. The
diode laser was used for dissecting out the tumor from its
attachment along with the mucosa. Under direct vision,
the attachment was ablated with the laser in the cutting
and coagulation modes, and the tumor was then delivered.
The unique feature of our management was the use of the
diode laser. Inverted papillomas are notorious for exten-
sive bleeding, so a bloodless field was a great advantage.
The hemostatic property of the dode laser helped us to
achieve an almost bloodless field. This in turn helped us
visualize the exact site of tumor attachment. Laser was
essentially used in all three modes: contact, near-contact,
and noncontact to achieve cutting, vaporization and co-
agulation. The diode laser’s lesser depth of tissue pene-
tration and its capability to be used in contact, near con-
tact & non contact settings allows the laser to be safely
used near the lamina papyracea and skull base. So for
bilateral inverted papillomas limited to the nose and
paranasal sinuses, we believe our approach is a good
option in view of the low rates of intra operative blood
loss & minimal post operative morbidity.
4. Conclusion
Inverted papillomas are known for excessive bleeding
during tumour removal. The use of the diode laser in the
excision of inverted papillomas helps to achieve clear
intra operative field with no post operative blood transfu-
sion requirement.
REFERENCES
[1] D. P. Vrabec, “The Inverted Schneiderian Papilloma: 25-
Year Study,” Laryngoscope, Vol. 104, No. 5, 1994, pp.
582-608. http://dx.doi.org/10.1002/lary.5541040513
[2] T. T. Tsue, J. W. Bailet, D. W. Barlow and K. H.
Makielski, “Bilateral Sinusal Papilloma in Aplasic Maxi-
lar Sinuses,” American Journal of Otolaryngology, Vol.
l18, No. 4, 1997, pp. 263-268.
[3] M. C. Weissle r, W. W. Montgomery and S. K. Montgom-
ery, “Inverted Papiloma,” The Annals of Otolo gy, Rhinology,
and Laryngology, Vol. 95, 1986, pp. 215-221.
[4] K. Oikawa, Y. Furuta, N. Oridate, T. Nagahashi, A. Homma,
T. Ryu and S. Fukuda, “Preoperative Staging of Sinonasal
Inverted Papilloma by Magnetic Resonance Imaging,”
Laryngoscope, Vol. 133, No. 11, 2003, pp. 1983-1987.
[5] M. M. Lesperance and M. E. Ramon, “Squamous Cell
Carcinoma Arising in Inverted Papilloma,” Laryngoscope,
Vol. 105, No. 2, 1995, pp. 178-183.
http://dx.doi.org/10.1288/00005537-199502000-00013
[6] E. Raveh, R. Feinmesser, T. Shpitzer, E. Yaniv and K.
Segal, Israel Journal of Medical Sciences, Vol. 32, 1996,
p. 1162.
[7] D. P. Vrabec, “The Inverted Schneiderian Papilloma: A
25-Year Study,” Laryngoscope, Vol. 104, No. 5, 1994, pp.
502-605. http://dx.doi.org/10.1002/lary.5541040513
[8] L. Segal, E. Atar and C. Mor, “Inverted Papilloma of the
Nose and Paranasalsinuses,” Laryngoscope, Vol. 96, No.
4, 1996, pp. 394-398.
[9] J. A. Stankiewicz and S. J. Girs, “Endoscopic Surgical
Treatment of Nasal and Paranasal Sinus Inverted Papil-
loma,” Otolaryngology—Head and Neck Surgery, Vol.
109, No. 6, 1993, pp. 988-995.
[10] A. C. M. Alegre, A. H. C. Ramos, R. L. Voegels and F.
Romano, “Papiloma e Papilomainvertido,” In: C. A. Ca m-
pos and H. O. O. Costa, Eds., Tratado de Otorrinolarin-
gologia, Roca, São Paulo, 2003, pp. 126-132.
[11] J. H. Krouse, “Development of a Staging System for In-
verted Papilloma,” Laryngoscope, Vol. 110, No. 6, 2000,
pp. 965-968.
http://dx.doi.org/10.1097/00005537-200006000-00015
[12] D. P. Vrabec, “The Inverted Schneiderian Papilloma: A
Open Access IJOHNS