T. A. ALI ET AL.
284
cystadenocarcinoma often shows little atypia [13]. Dif-
ferentiation of tumou r types depends largely on the id en-
tification of actual infiltration of salivary gland paren-
chyma or surrounding connective tissue by either cystic
or solid epithelium in cystadenocarcino mas.
The suggested management for these benign lesions is
conservative and consists of complete local excision
[5,14]. Open laryngeal surgery like Lateral/Median Thy-
rotomy and pharyngotomy approach or transoral ap-
proach is required for the cartilaginous structures of the
larynx; if the position of larynx is to be altered, or if the
anatomical situation of lesion prevents adequate endo-
scopic visualization .
Laryngeal lesions located in the mucosa or sub muco-
sal space is easily accessible to endoscopic approach
with advantages of avoidance of skin incisions, division
of the thyroid cartilage and tracheotomy.
The surgical approach and excision depend on the tu-
mor size and location; but in general, preservation of
laryngeal function is the primary aim of treatment in the
form of complete excision with tumor-free margins. With
improvements in imaging, histopathology, and surgical
techniques—endoscopy, microscopic magnification, ap-
plication of lasers—there has been marked improvement
in the accuracy of diagnosis and the ability to perform
precision excision surgery for benign tumors. This means
more preservation and restoration of laryngeal function
than was previously possible [15]. As per the recom-
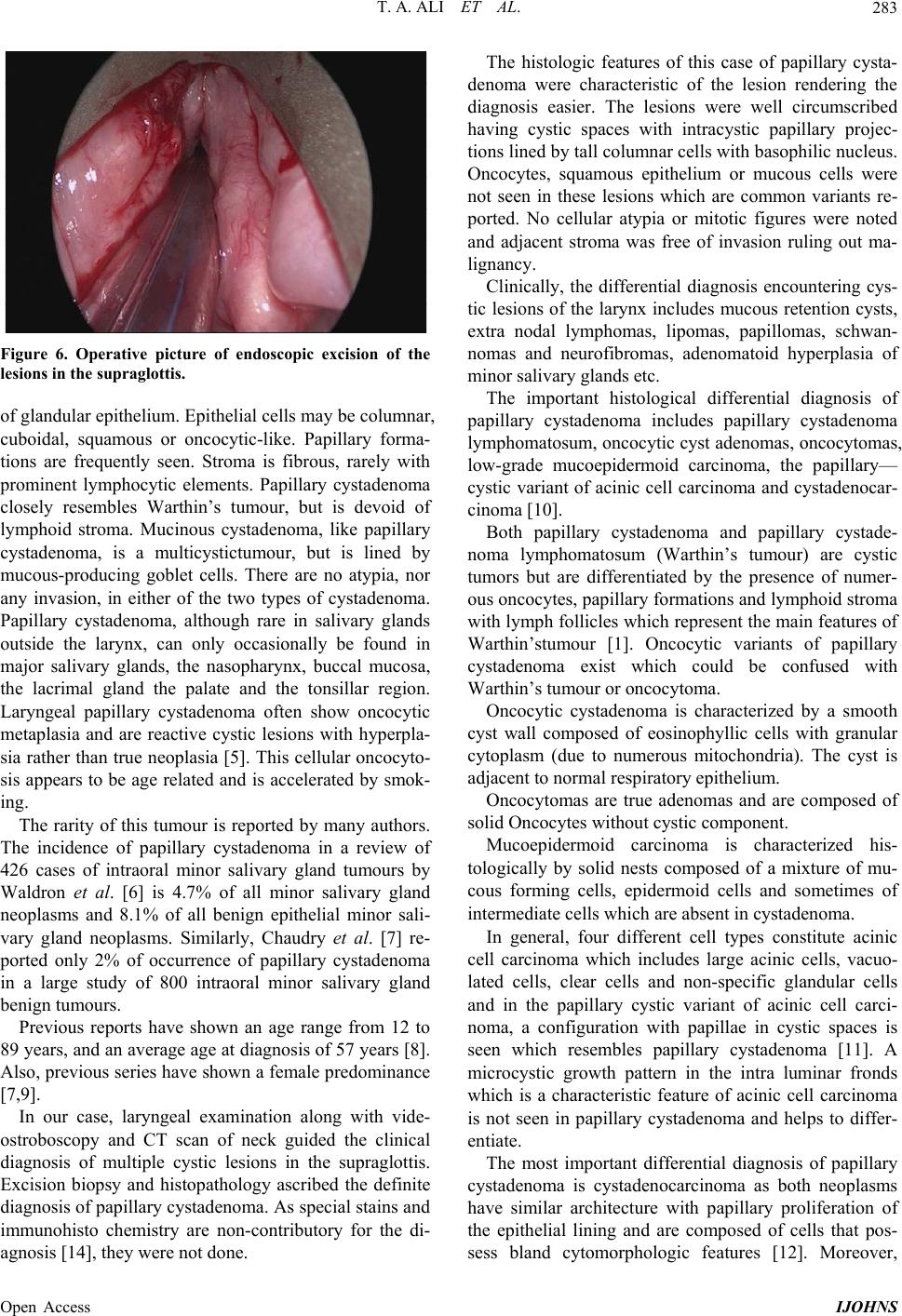
mendations, we completely excised the entire cysts in
supraglottis by endoscopic micro laryngeal surgery and
histopathology reconfirmed the diagnosis as benign pap-
illary cystadenoma. Although papillary cystadenoma are
benign lesions, follow-up is recommended, as recom-
mended for oncocytic cysts since recurrence is possible,
especially in the case of patients with multiple involve-
ments, with a tendency to develop new cysts [16]. In our
case, considering the benign nature of the lesions, annual
revisions were decided for a minimum period of five
years.
4. Conclusion
We present this case of multiple laryngeal papillary cys-
tadenomas, a rare benign lesion presenting with hoarse-
ness and dysphagia as this clinical en tity h as to be kept in
mind while evaluating patients with above mentioned
symptoms. Moreover, the histo-pathological diagnosis is
crucial as many tumours are with similar features and
management of each varies.
REFERENCES
[1] P. L. Auclair, G. L. Ellis and D. R. Gnepp, “Other Benign
Epithelial Neoplasms,” In: G. L. Ellis, P. L. Auclair and
D. R. Gnepp, Eds., Surgical Pathology of the Salivary
Glands, Saunders, Philadelphia, 1991, pp. 252-268.
[2] C. A. Waldron, S. K. El-Mofty and D. R. Gnepp, “Tu-
mors of the Intraoral Minor Salivary Glands: A Demo-
graphic and Histologic Study of 426 Cases,” Oral Surgery,
Oral Medicine, Oral Pathology, Vol. 66, No. 3, 1988, pp.
323-333.
http://dx.doi.org/10.1016/0030-4220(88)90240-X
[3] J. Alexis, “Dewbrow Papillary Cystadenoma of a Minor
Salivary Gland,” Journal of Oral and Maxillofacial Sur-
gery, Vol. 53, No. 1, 1995, pp. 70-72.
http://dx.doi.org/10.1016/0278-2391(95)90506-5
[4] G. Seifert, “Histological Typing of Salivary Gland Tu-
mors,” In: World Health Organization International His-
tological Classification of Tumors, S p ri nge r , G en e va, 1991.
[5] L. Michaels and H. B. Hellquist, “Ear Nose and Throat
Histopathology,” 2nd Edition, Springer, Berlin, 2001, p.
489. http://dx.doi.org/10.1007/978-1-4471-0235-9
[6] C. A. Waldron, S. K. El-Mofty and D. R. Gnepp, “Tu-
mors of the Intraoral Minor Salivary Glands: A Demo-
graphic and Histologic Study of 426 Cases,” Oral Sur-
gery, Vol. 66, No. 3, 1988, pp. 323-333.
http://dx.doi.org/10.1016/0030-4220(88)90240-X
[7] A. P. Chaudhry, R. A. Vickers and R. J. Gorlin, “Intraoral
Minor Salivary Gland Tumors: An Analysis of 1414 Cases,”
Oral Surgery, Oral Medicine, Oral Pathology, Vol. 14,
No. 10, 1961, pp. 1194-1126.
http://dx.doi.org/10.1016/0030-4220(61)90209-2
[8] C. S. Lim, I. Ngu, A. P. Collins and G. M. McKellar,
“Papillary Cystadenoma of a Minor Salivary Gland: Re-
port of a Case Involving Cytological Analysis and Re-
view of the Literature,” The Online Version of Oral Sur-
gery, Oral Medicine, Oral Pathology, Oral Radiology, and
Endodontology, Vol. 105, No. 1, 2008, pp. e28-e33.
http://dx.doi.org/10.1016/j.tripleo.2007.07.019
[9] G. L. Ellis and P. L. Auclair, “Atlas of Tumor Pathology:
Tumors of the Salivary Glands,” Armed Forces Institute
of Pathology, Washington DC, 1995, pp. 115-120.
[10] J. W. Eveson and T. Nago, “Cystadenoma,” In: L. Barnes,
Ed., Diseases of the Salivary Glands. Surgical Pathology
of the Head and Neck, 3rd Edition, Informa Healthcare,
New York, 2009, pp. 538-540.
[11] G. Seifert, C. Brocheriou, A. Cardesa and J. W. Eveson,
“WHO International Histol ogic Classification of Tumours.
Tentative Histological Classification of Salivary Gland
Tumours,” Pathology, Research and Practice, Vol. 186,
No. 5, 1990, pp. 555-581.
http://dx.doi.org/10.1016/S0344-0338(11)80220-7
[12] L. Gallego, L. Junquera, M. F. Fresno and J. C. De V i cen t e ,
“Papillary Cystadenoma and Cystadenocarcinoma of Sali-
vary Glands: Two Unusual Entities,” Medicina Oral Pa-
tologia Oral y Cirugia Bucal, Vol. 13, No. 7, 2008, pp.
460-463.
[13] R. D. Foss, G. L. Ellis and P. L. Auclair, “Salivary Gland
Cystadenocarcinomas. A Clinicopathologic Study of 57
Cases,” American Journal of Surgical Pathology, Vol. 20,
No. 12, 1996, pp. 1440-1447.
http://dx.doi.org/10.1097/00000478-199612000-00002
[14] A. N. Kalof, M. F. Evans and K. Cooper, “Special Diag-
Open Access IJOHNS