Paper Menu >>
Journal Menu >>
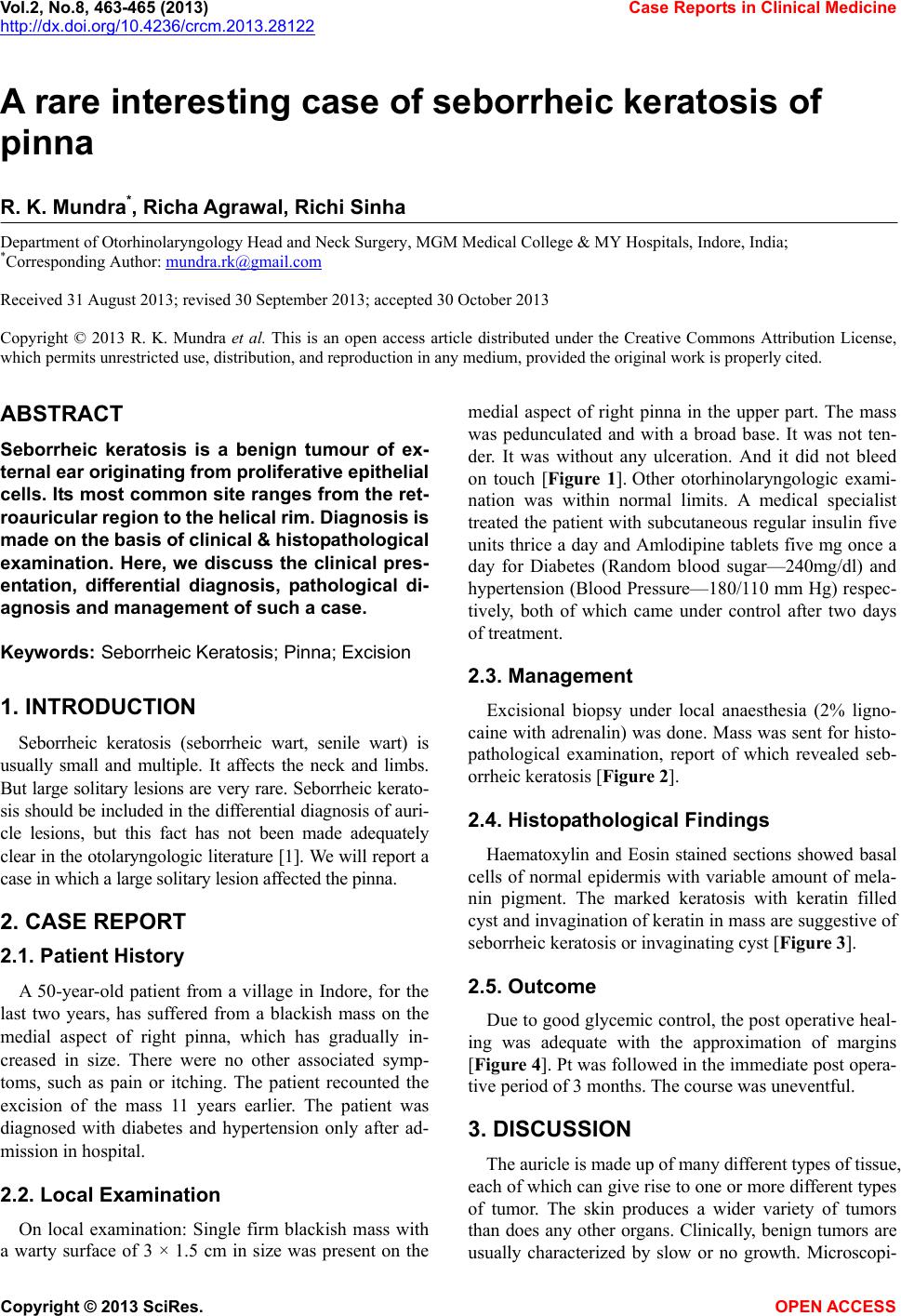 Vol.2, No.8, 463-465 (2013) Case Reports in Clinical Medicine http://dx.doi.org/10.4236/crcm.2013.28122 A rare interesting case of seborrheic keratosis of pinna R. K. Mundra*, Richa Agrawal, Richi Sinha Department of Otorhinolaryngology Head and Neck Surgery, MGM Medical College & MY Hospitals, Indore, India; *Corresponding Author: mundra.rk@gmail.com Received 31 August 2013; revised 30 September 2013; accepted 30 October 2013 Copyright © 2013 R. K. Mundra et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Seborrheic keratosis is a benign tumour of ex- ternal ear originating from proliferative epithelial cells. Its most common site ranges from the ret- roauricular region to the helical rim. Diagno sis is made on the basis of clinical & histopathological examination. Here, we discuss the clinical pres- entation, differential diagnosis, pathological di- agnosis and management of such a case. Keywords: Seborrheic Keratosis; Pinna; Excision 1. INTRODUCTION Seborrheic keratosis (seborrheic wart, senile wart) is usually small and multiple. It affects the neck and limbs. But large solitary lesions are very rare. Seborrheic kerato- sis should be included in the differential diagnosis of auri- cle lesions, but this fact has not been made adequately clear in the otolaryngologic literature [1]. We will report a case in which a large solitary lesion af fected the pi nna. 2. CASE REPORT 2.1. Patient History A 50-year-old patient from a village in Indore, for the last two years, has suffered from a blackish mass on the medial aspect of right pinna, which has gradually in- creased in size. There were no other associated symp- toms, such as pain or itching. The patient recounted the excision of the mass 11 years earlier. The patient was diagnosed with diabetes and hypertension only after ad- mission in hospital. 2.2. Local Examination On local examination: Single firm blackish mass with a warty surface of 3 × 1.5 cm in size was present on the medial aspect of right pinna in the upper part. The mass was pedunculated and with a broad base. It was not ten- der. It was without any ulceration. And it did not bleed on touch [Figure 1]. Other otorhinolaryngologic exami- nation was within normal limits. A medical specialist treated the patient with subcutaneous regular insulin five units thrice a day and Amlodipine tablets five mg once a day for Diabetes (Random blood sugar—240mg/dl) and hypertension (Blood Pressure—180/110 mm Hg) respec- tively, both of which came under control after two days of treatment. 2.3. Management Excisional biopsy under local anaesthesia (2% ligno- caine with adrenalin) was done. Mass was sent for histo- pathological examination, report of which revealed seb- orrheic keratosis [Figure 2]. 2.4. Histopathological Findings Haematoxylin and Eosin stained sections showed basal cells of normal epidermis with variable amount of mela- nin pigment. The marked keratosis with keratin filled cyst and invagination of keratin in mass are suggestive of seborrheic keratosis or invaginating cyst [Figur e 3]. 2.5. Outcome Due to good glycemic control, the post operative heal- ing was adequate with the approximation of margins [Figure 4]. Pt was followed in the immediate post opera- tive period of 3 months. The course was uneventful. 3. DISCUSSION The auricle is made up of many different types of tissue, each of which can give rise to one or more different types of tumor. The skin produces a wider variety of tumors than does any other organs. Clinically, benign tumors are usually characterized by slow or no growth. Microscopi- Copyright © 2013 SciRes. OPEN ACCESS  R. K. Mundra et al. / Case Reports in Clinical Medicine 2 (2013) 463-465 464 Figure 1. Photograph showing blackish mass over pinna. Figure 2. Gross specimen of mass exc ised. Figure 3. Haematoxylin & Eosin stained high power section microphotograph showing keratin pearls with hyperchromatic epithelium. cally, these tumors feature a well-organized cellular pat- tern [2]. Figure 4. Post-operative photograph showing pinna after exci- sion of mass. Ultraviolet light exposure, human papillomavirus in- fection, hereditary factors, action of oestrogen and other sex hormones are among those factors which have been suggested in the aetiology of this disease. Secondary ma- lignant changes may occur but are extremely rare [3]. Since it may be confused with malignant melanoma or squamous cell carcinoma, obtaining a specimen for his- tology is essential. Histologically this lesion can be di- vided into seven subtypes: acanthotic, hyperkeratotic, adenoidal or reticu lated, clonal, irritated, inverted follicu- lar keratosis, and melanoacanthom a variants. 3.1. Differential Diagnosis Other lesions mimicking seborrheic keratosis in clini- cal presentation are: Atheroma (sebaceous cyst, atheroma, steatoma, keratinous cyst) is a benign tumor which is mostly located in the back of the ear lobe. On clinical ex- amination, it appears as a 5 - 25 mm firm displace- able nodule and may show signs of secondary infec- tion. Sometimes, a pinpoint depression at the surface of the cyst corresponds to the infundibulum of a pre- existing hair follicle [3]. Actinic keratoses (solar keratoses or senile kera- toses) is a UV light-induced lesion which is often lo- cated on the ear, especially on the helical rim. Its fre- quency increases with age and can progress to inva- sive squamous cell carcinoma in 20%. Its prevalence is higher in individuals with fair complexion. Mostly, a well-defined patch with a rough texture, 3 - 8 mm in diameter, and a typically erythematous base is visible, accompanied by occasional hyperkeratosis. Signs of inflammation may occur [3]. Lentigomaligna (Hutchinson’s freckle) is a slow- growing, non-invasive melanoma in situ. The lesion begins as an unevenly pigmented and irregularly Copyright © 2013 SciRes. OPEN ACCESS 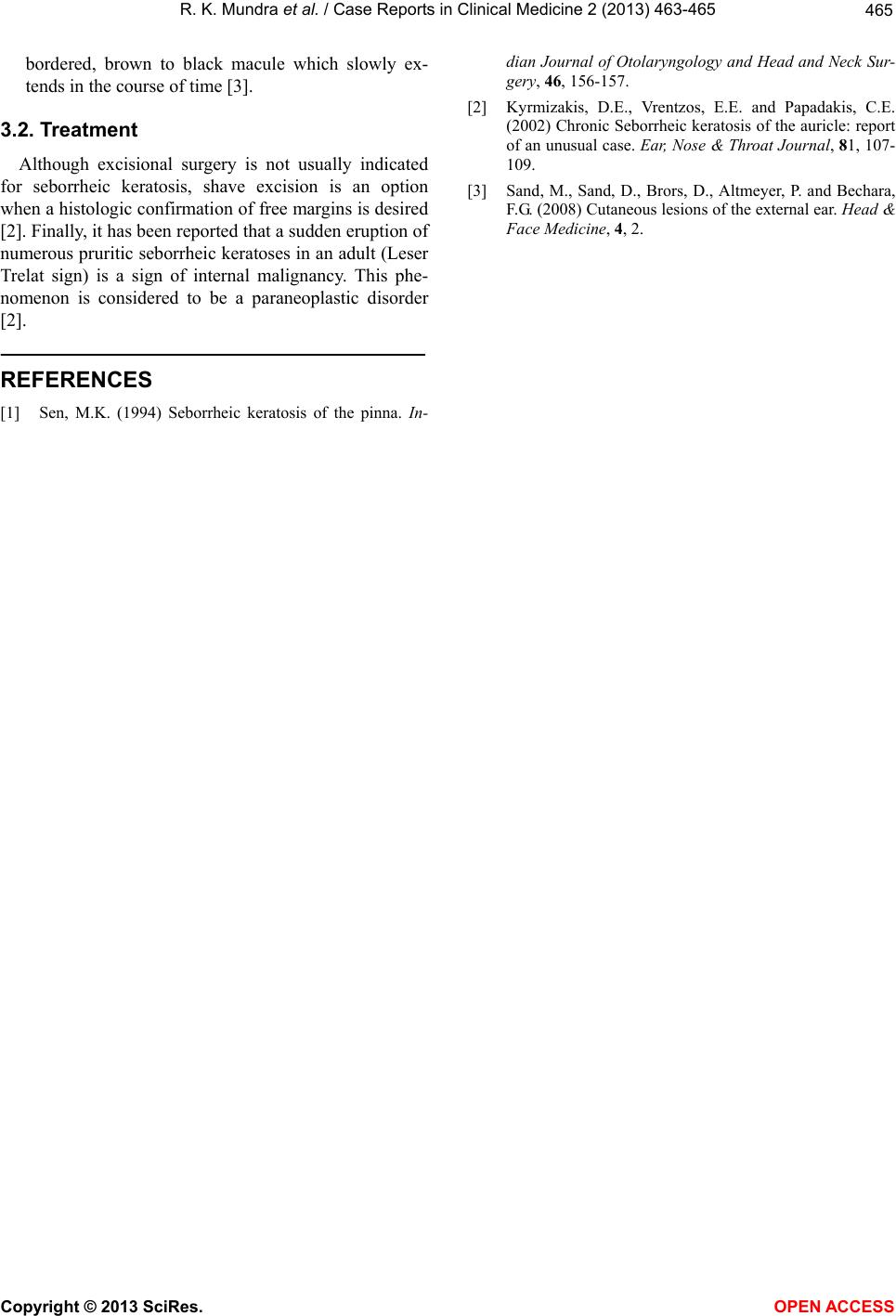 R. K. Mundra et al. / Case Reports in Clinical Medicine 2 (2013) 463-465 Copyright © 2013 SciRes. OPEN ACCESS 465 bordered, brown to black macule which slowly ex- tends in the course of time [3]. 3.2. Treatment Although excisional surgery is not usually indicated for seborrheic keratosis, shave excision is an option when a histologic confirmation of free margins is desired [2]. Finally, it has been reported that a su dd en erup tion of numerous pruritic seborrheic keratoses in an adult (Leser Trelat sign) is a sign of internal malignancy. This phe- nomenon is considered to be a paraneoplastic disorder [2]. REFERENCES [1] Sen, M.K. (1994) Seborrheic keratosis of the pinna. In- dian Journal of Otolaryngology and Head and Neck Sur- gery, 46, 156-157. [2] Kyrmizakis, D.E., Vrentzos, E.E. and Papadakis, C.E. (2002) Chronic Seborrheic keratosis of the auricle: report of an unusual case. Ear, Nose & Throat Journal, 81, 107- 109. [3] Sand, M., Sand, D., Brors, D., Altmeyer, P. and Bechara, F.G. (2008) Cutaneous lesions of the external ear. Head & Face Medicine, 4, 2. |