X. M. Shi et al. / Case Rep orts in Clinical Med icine 2 (2013) 460-462
Copyright © 2013 SciRes. OPEN ACCESS
462
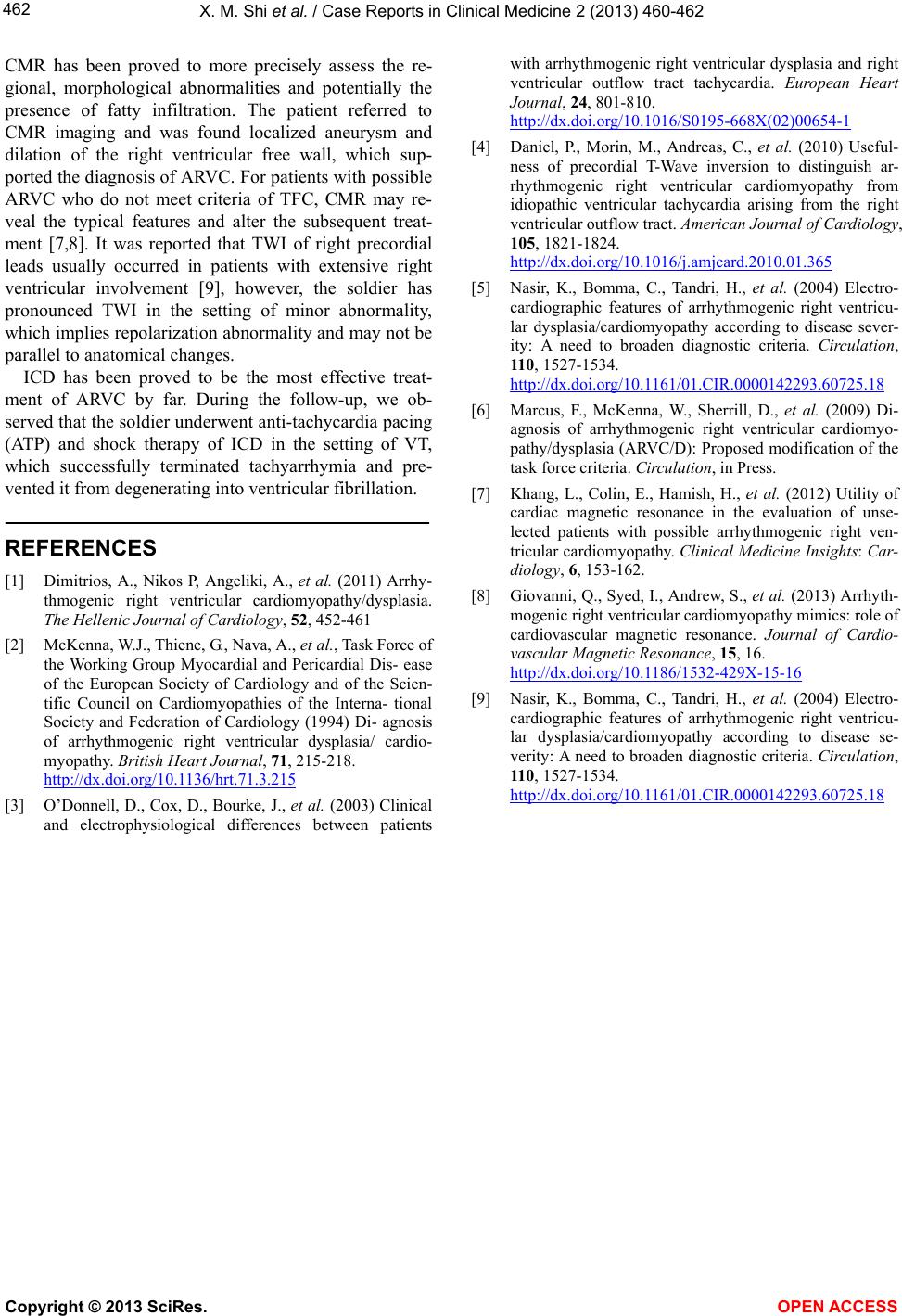
CMR has been proved to more precisely assess the re-
gional, morphological abnormalities and potentially the
presence of fatty infiltration. The patient referred to
CMR imaging and was found localized aneurysm and
dilation of the right ventricular free wall, which sup-
ported the diagnosis of ARVC. For patients with possible
ARVC who do not meet criteria of TFC, CMR may re-
veal the typical features and alter the subsequent treat-
ment [7,8]. It was reported that TWI of right precordial
leads usually occurred in patients with extensive right
ventricular involvement [9], however, the soldier has
pronounced TWI in the setting of minor abnormality,
which implies repolarization abnormality and may not be
parallel to anatomical changes.
ICD has been proved to be the most effective treat-
ment of ARVC by far. During the follow-up, we ob-
served that the soldier und erwent anti-tachycardia pacing
(ATP) and shock therapy of ICD in the setting of VT,
which successfully terminated tachyarrhymia and pre-
vented it from degenerating in to ventricular fibrillation.
REFERENCES
[1] Dimitrios, A., Nikos P, Angeliki, A., et al. (2011) Arrhy-
thmogenic right ventricular cardiomyopathy/dysplasia.
The Hellenic Journal of Cardiology, 52, 452-461
[2] McKenna, W.J., Thiene, G., Na va, A., et al., Task Force of
the Working Group Myocardial and Pericardial Dis- ease
of the European Society of Cardiology and of the Scien-
tific Council on Cardiomyopathies of the Interna- tional
Society and Federation of Cardiology (1994) Di- agnosis
of arrhythmogenic right ventricular dysplasia/ cardio-
myopathy. British Heart Journal, 71, 215-218.
http://dx.doi.org/10.1136/hrt.71.3.215
[3] O’Donnell, D., Cox, D., Bourke, J., et al. (2003) Clinical
and electrophysiological differences between patients
with arrhythmogenic right ventricular dysplasia and right
ventricular outflow tract tachycardia. European Heart
Journal, 24, 801-810.
http://dx.doi.org/10.1016/S0195-668X(02)00654-1
[4] Daniel, P., Morin, M., Andreas, C., et al. (2010) Useful-
ness of precordial T-Wave inversion to distinguish ar-
rhythmogenic right ventricular cardiomyopathy from
idiopathic ventricular tachycardia arising from the right
ventricular outflow tract. American Journal of Cardiology,
105, 1821-1824.
http://dx.doi.org/10.1016/j.amjcard.2010.01.365
[5] Nasir, K., Bomma, C., Tandri, H., et al. (2004) Electro-
cardiographic features of arrhythmogenic right ventricu-
lar dysplasia/cardiomyopathy according to disease sever-
ity: A need to broaden diagnostic criteria. Circulation,
110, 1527-1534.
http://dx.doi.org/10.1161/01.CIR.0000142293.60725.18
[6] Marcus, F., McKenna, W., Sherrill, D., et al. (2009) Di-
agnosis of arrhythmogenic right ventricular cardiomyo-
pathy/dysplasia (ARVC/D): Proposed modification of the
task force criteria. Circulation, in Pres s .
[7] Khang, L., Colin, E., Hamish, H., et al. (2012) Utility of
cardiac magnetic resonance in the evaluation of unse-
lected patients with possible arrhythmogenic right ven-
tricular cardiomyopathy. Clinical Medicine Insights: Car-
diology, 6, 153-162.
[8] Giovanni, Q., Syed, I., Andrew, S., et al. (2013) Arrhyth-
mogenic right ventricular cardiomyopathy mimics: role of
cardiovascular magnetic resonance. Journal of Cardio-
vascular Magnetic Resonance, 15, 16.
http://dx.doi.org/10.1186/1532-429X-15-16
[9] Nasir, K., Bomma, C., Tandri, H., et al. (2004) Electro-
cardiographic features of arrhythmogenic right ventricu-
lar dysplasia/cardiomyopathy according to disease se-
verity: A need to broaden diagnostic criteria. Circulation,
110, 1527-1534.
http://dx.doi.org/10.1161/01.CIR.0000142293.60725.18