Vol.2, No.8, 445-447 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.28116
Successful left-sided accessory pathway ablation
without reference catheter in patient with atresia of
coronary sinus and thin persistent left superior
vena cava*
Qingxing Chen, Ye Xu, Kuang Cheng, Wenqing Zhu#
Department of Cardiology, Zhongshan Hospital, The Shanghai Institute of Cardiovascular Diseases, Fudan University, Shanghai,
China; #Corresponding Author: zhu.wenqing@zs-hospital.sh.cn
Received 7 September 2013; revised 1 October 2013; accepted 29 October 2013
Copyright © 2013 Qingxing Chen et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
We report a case of atrioventricular reentrant
tachycardia (AVRT) with ostial atresia of the
coronary sinus (CS). Without the anatomic an-
giography, radiofrequency (RF) energy was ap-
plied at the mitral valve annulus and the bypass
tract was eliminated. After the therapy proce-
dure, by CS angiography, we knew the persis-
tent left superior vena cava (PLSVC), and the
coronary sinus was connected with vena cava
superior, very thin in a diameter. The therapy
procedure was successful. The patient has re-
mained completely symptom free.
Keyw ords: Ablation; Accessory Pathway; Atresia of
the Coronary Sinus
1. INTRODUCTION
Coronary sinus (CS) atresia is a rare cardiac anatomic
variant which causes failure to cannulate CS and consid-
erable challenges in affecting cure. CS ostial atresia was
associated with a few persistent left superior vena cavas
(PLSVC), an unroofed coronary sinus, or was a postop-
erative complication [1-5]. Patients with CS ostial atresia
have been reported to have atrioventricular reentrant
tachycardia [3-5], atrial flutter [4], and atrioventricular
nodal reentrant tachycardia [6].
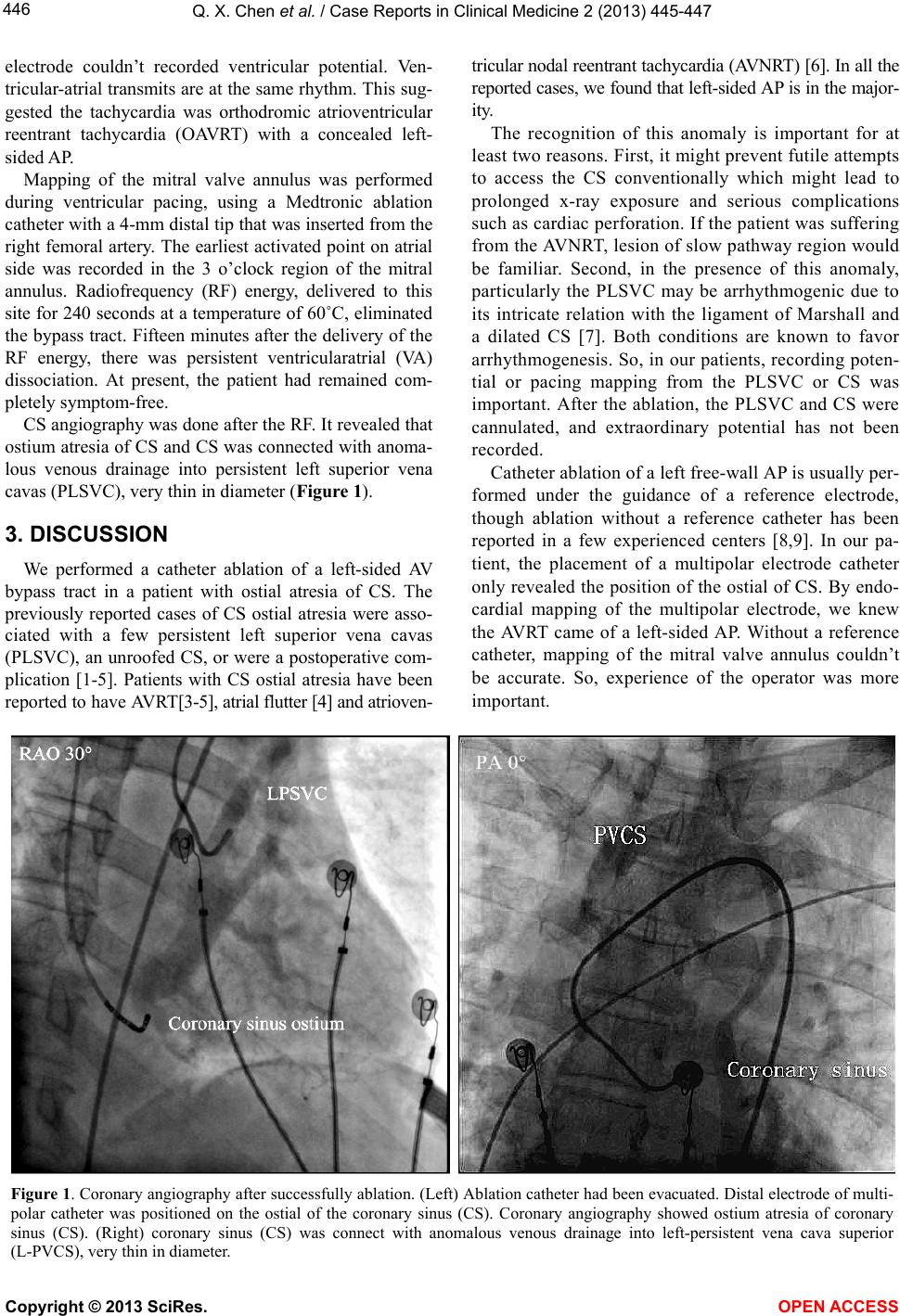
We report a case of CS ostial atresia with anomalous
venous drainage into PLSVC with a left-sided accessory
pathway (AP) that was successfully eliminated by cathe-
ter ablation.
2. CASE REPORT
A 57-year-old man with recurrent paroxysmal su-
praventricular tachycardia (PSVT) effective to propa-
fenone was referred to our hospital for a cardiac electro-
physiologicstudy (EPS) and ablation one month ago. A
12-lead electrocardiogram (ECG) done during sinus
rhythm exhibited no delta waves. A 12-lead ECG done
during the palpitation revealed a regular, narrow QRS
tachycardia at a rate of 170 bpm with P’-waves in leads
II and aVF, QRS-P’ interval was 86ms; this suggested
that the patient had an atrioventricular reentrant tachy-
cardia (AVRT) through a concealed accessory pathway
(AP). The physical examination, chest x-ray, echocar-
diograms and serological examinations were normal.
After written informed consent was obtained from the
patient, EPS was done after the withdrawal of all antiar-
rhythmic drugs for five elimination half-lives.
One quadripolar electrode catheter was cannulated
from Vena cava inferior, positioned in the right ventricu-
lar apex. One multipolar electrode catheter was cannu-
lated from Subclavian Vein. Attempts to cannulate the
coronary sinus (CS) were unsuccessful. Without CS an-
giography, we set a proximal electrode of multipolar
catheter on the ostial of CS.
Baseline intervals during sinus were as follows: sinus
cycle length 660 ms, atrial His (AH) interval 79 ms, and
His-ventricular (HV) interval 64 ms. There was no ven-
tricular preexcitation during sinus rhythm and decre-
mental ventricular pacing down to 350 ms. A regular,
narrow QRS tachycardia with a cycle length of 350 ms
was repeatly induced. During tachycardia, proximal mul-
tipolar electrode was revealed V-A interval 86 ms, mid-
dle electrode was revealed V-A interval 145 ms, distal
*Conflict of Interest: None.
Copyright © 2013 SciRes. OPEN A CCESS