Vol.2, No.8, 437-438 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.28114
A case of mixed geno—Phenotype of generalized
dystonia and strumpel disease*
Vadim Belenky
Yavorskiy Homeopathic Clinic, Saint Petersburg, Russia; vadimbele@yahoo.com
Received 3 September 2013; revised 30 September 2013; accepted 29 October 2013
Copyright © 2013 Vadim Belenky. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Background: St rumpel disease and dystonia are
inherited disorders with the clinical picture of
spastic paraparesis and hyperkinesis respec-
tively. We present a case of a patient born from
parents with these diseases who developed
neurologic phenomena uncharacteristic for the
classical clinical picture of his parents’ disor-
ders. Case report: Patient V., 12, born from his
father with generalized dystonia and mother
with Strumpel disease, has flaccid lower para-
plegia along with dystonic hyperkinesis in neck
and arms. Discussion: The flaccid lower para-
plegia could be caused by the anterior horn le-
sion. This phenomenon is unclear because an-
terior horn lesions were not diagnosed in the
proband’s parents.
Keywords: Dystonia; Strumpel Disease; DYT 1
1. INTRODUCTION
Dystonia and Strumpel diseases, i.e. hereditory spastic
paraparesis (HSP), are heterogenious conditions; muta-
tions in more than 50 different genetic loci have been
described to cause HSP and more than 20 different ge-
netic forms of dystonia. Lesions of extrapyramidal sys-
tem are responsible for clinical signs of dystonia with
extrapyramidal rigidity in muscles. In case of Strumpel
disease with lower spastic paraparesis, caused by lesions
of corticospinal tract, spasticity in muscles grows by a
pyramidal type. Flaccid paresis is not characteristic for
either of these two disorders. Patient V., 12, born from
his father with generalized non-DYT 1 dystonia and
mother with Strumpel disease, has flaccid lower paraple-
gia along with hands and neck dystonia.
2. CASE STORY
I first met patient S. with generalized non-DYT 1
dystonia in 1987 on summer practice at neurologic de-
partment, being a third year student of a medical school.
He then was 21. He fell ill at the age of 9 and soon in-
voluntary movements became generalized. None of his
relatives was affected by this disease. Though classical
research of Eldridge [1] established superior IQ of pa-
tients with recessive forms of dystonia, we observed very
clever and vivid mind in our patient. Later he married a
woman with indolently progressive Strumpel disease,
and their son inherited both parents’ diseases—from
early childhood he developed flaccid lower paraplegia
with complete absence of strength in legs and dystonic
hyperkinesis in neck and arms, while having IQ as high
as his father’s. The son underwent embryonal transplan-
tation surgery into his brain with no significant effect.
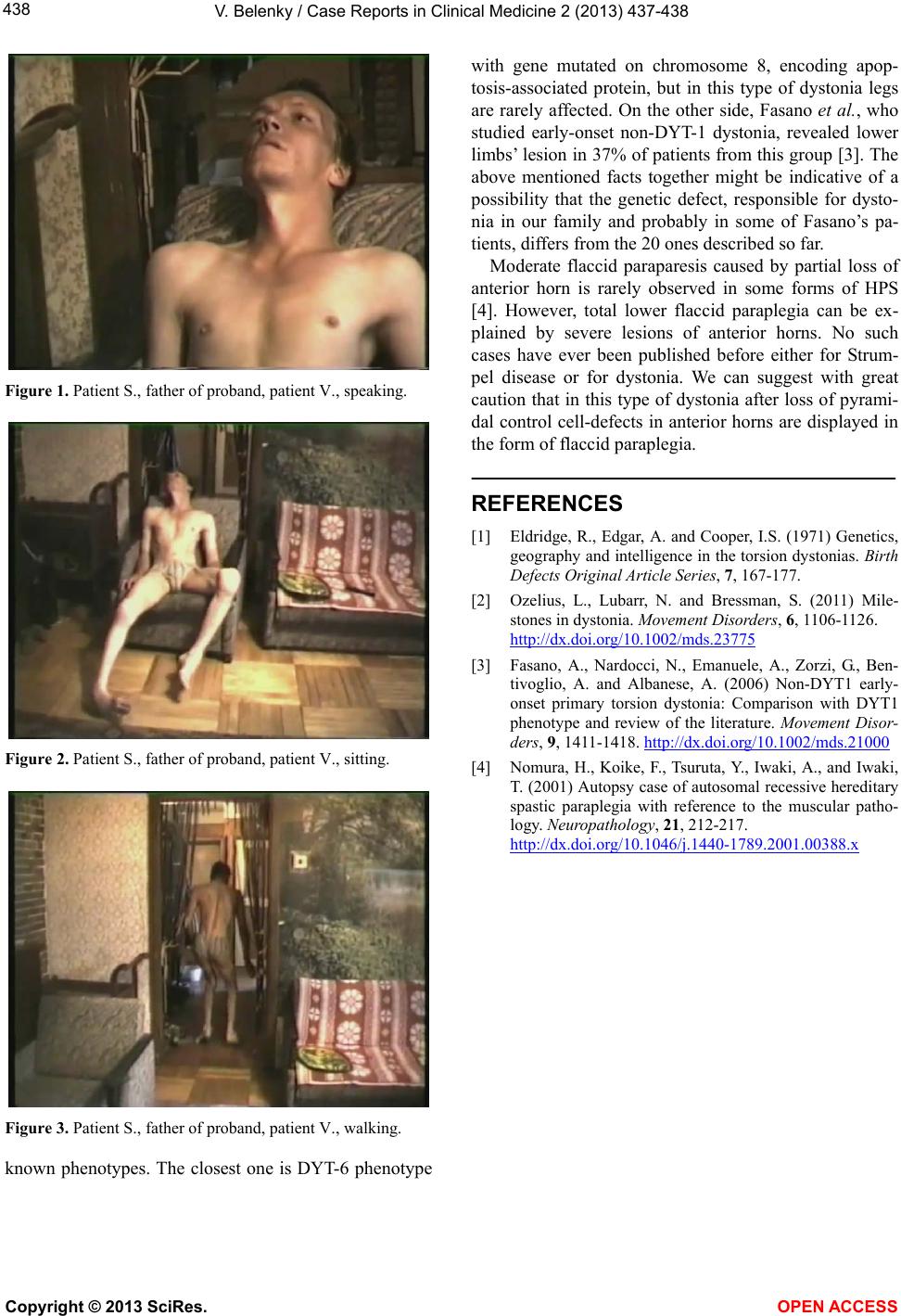
His father—patient S.—when hospitalized was given
L-Dopa with no effect. I started tryhehyphenidyl therapy
for patient S, which resulted in considerable improve-
ment in his condition. Test for DYT 1 proved negative.
Along with test results of my other primary dystonia pa-
tients from the monitored group his serotonin exchange
tended to be on the increase. His videoexamination was
conducted befo re tryhehyph enidyl therap y (Figures 1-3).
Unfortunately, the mother of the proband refused to
videotype her son after brutal murder of her hus-
band—patient S. on May 9th 2005—Russia’s national
Victory Day holiday; patient S. ventured to leave the
house in his wheelchair for the first time after the winter
and never got back. Later he was found dead with tens of
stab wounds and his neck cut.
3. DISCUSSION
More than 20 genetic loci of dystonia have been dis-
covered so far [2 ], but the clinical picture of the disorder
of our proband’s father, i.e. non DYT-1 early onset gen-
eralized autosomal dominant dystonia, differs from all
*Financial disclosure: The study was not funded.
Copyright © 2013 SciRes. OPEN ACCESS