Journal of Cosmetics, Dermatological Sciences and Applications, 2013, 3, 1-3
Published Online November 2013 (http://www.scirp.org/journal/jcdsa)
http://dx.doi.org/10.4236/jcdsa.2013.33A2001
Open Access JCDSA
1
Undifferentiated Pleomorphic Sarcoma of the Cheek
with Surface Ulceration: Mimicking Spindle Cell
Squamous Cell Carcinoma
Fumiko Momma*, Chihiro Onami, Takayuki Konno, Tamio Suzuki
Department of Dermatology, Faculty of Medicine, Yamagata University, Yamagata, Japan.
Email: *fmonma@med.id.yamagata-u.ac.jp
Received August 9th, 2013; revised September 4th, 2013; accepted September 11th, 2013
Copyright © 2013 Fumiko Momma et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Undifferentiated pleomorphic sarcoma (UPS), also called malignant fibrous histiocytoma (MFH), belongs to the soft
tissue tumors and is more likely in elder patients. UPS currently accounts for approximately 18% of cutaneous soft tis-
sue sarcoma except Kaposi sarcoma. The most common sites are the extremities and head and n eck. UPS is rapidly en-
larging, and easily invades subcutaneous tissue and muscle without overlying skin changes. UPS tumors, which are
confined to subcutaneous tissue, have been reported to be less than 10%. On the other hand, the involvement of the ep-
idermis, occasionally with ulceration, is rare. Here, we describe a case of UPS of the cheek with surface ulceration. An
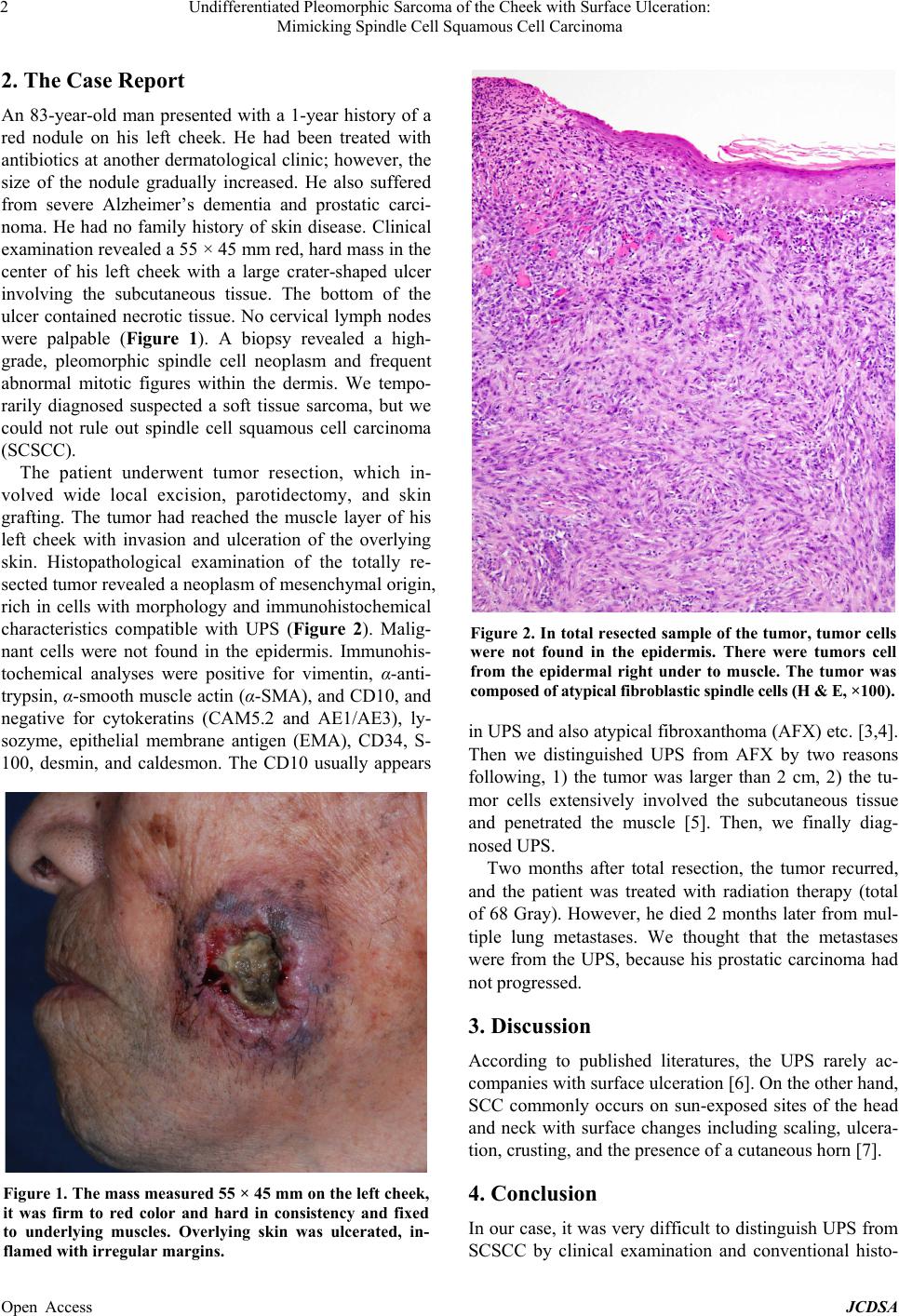
83-year-old man presented with a 1-year history of a red nodule on his left cheek. The size of the nodule gradually in-
creased. Clinical examination revealed a 55 × 45 mm red, hard mass in the center of his left cheek with a large crater-
shaped ulcer involving the subcutaneous tissue. The bottom of the ulcer contained necrotic tissue. No cervical lymph
nodes were palpable. A biopsy revealed a high-grade, pleomorphic spindle cell neoplasm and frequent abnormal mitotic
figures within the dermis. We temporarily diagnosed and suspected a soft tissue sarcoma, but we could not rule out
spindle cell squamous cell carcinoma (SCSCC). The patient underwent tumor resection and skin grafting. The tumor
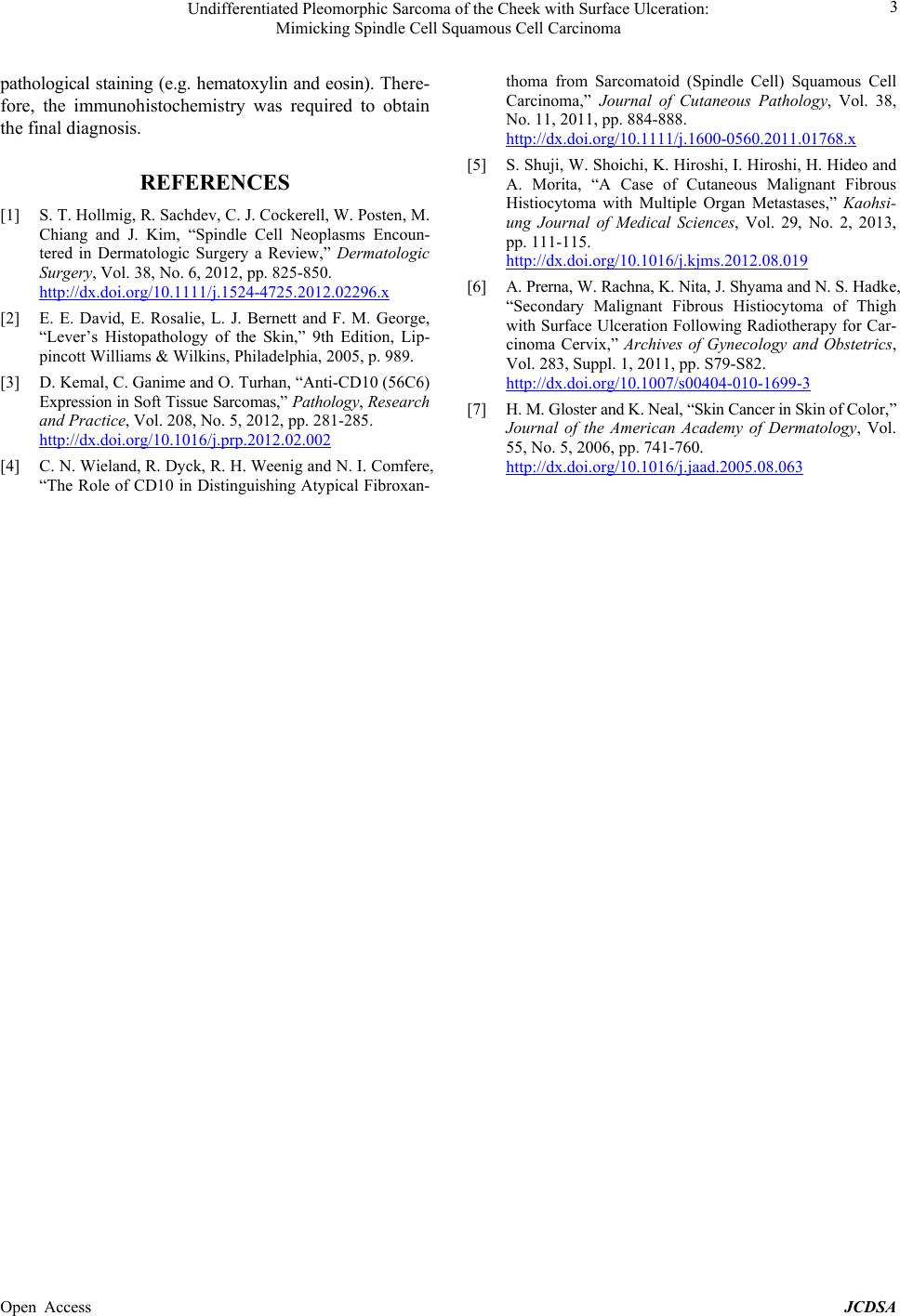
had reached the muscle layer of his left cheek with invasion and ulceration of the overlying skin. Histopathological
examination of the totally resected tumor revealed a neoplasm of mesenchymal origin, rich in cells with morphology
and immunohistochemical characteristics compatible with UPS. Malignant cells were not found in the epidermis. Im-
munohistochemical analyses were positive for vimentin, α-anti-trypsin, α-smooth muscle actin (α-SMA), and CD10,
and negative for cytokeratins (CAM5.2 and AE1/AE3), lysozyme, epithelial membrane antigen (EMA), CD34, S-100,
desmin, and caldesmon. Two months after total resection, the tumor recurred, and the patient was treated with radiation
therapy. However, he died 2 months later from multiple lun g metastases. We thought that the metastases were from the
UPS, because his prostatic carcinoma had not progressed. According to published literatures, the UPS rarely accompa-
nies with surface ulceration. On the other hand, SCC commonly occurs on sun-exposed sites of the head and neck with
surface changes including scaling, ulceration, crusting, and the presence of a cutaneous horn. In our case, it was very
difficult to distinguish UPS from SCSCC by clinical examination and conventional histopathological staining (e.g. he-
matoxylin and eosin). Therefore, the immunohistochemistry was required to obtain the final diagnosis.
Keywords: Undifferentiated Pleomorphic Sarcoma; Ulcer; Spindle Cell Squamous Cell Carcinoma
1. Introduction
Undifferentiated pleomorphic sarcoma (UPS), also called
malignant fibrous histiocytoma (MFH), belongs to the
soft tissue tumors and is more likely in elder patients.
UPS currently accounts for approximately 18% of cuta-
neous soft tissue sarcoma except Kaposi sarcoma [1].
The most common sites are the extremities and head and
neck [1]. UPS is rapidly enlarging, and easily invades
subcutaneous tissue and muscle without overlying skin
changes [1]. UPS tumors, which are confined to subcu-
taneous tissue, have been reported to be less than 10%.
On the other hand, the involvement of the epidermis,
occasionally with ulceration, is rare [2]. Here, we de-
scribe a case of UPS of the cheek with surface ulceration.
*Corresponding author.