R. H. LI ET AL.
Copyright © 2013 SciRes. ENG
and AD817, Anal og Device Instrument), which have low
noise, low drift and high p r e cisio n characteristics, to
achieve much stable sine wave current. Then the sine
wave current signal is fed into the bladder (Rx) and a
reference resistor (Ref) through a pair of excitation elec-
trodes.
c) The measurement channel
It mainly consists of differential amplifier circuits,
phase sensitive demodulation circuit and a 14-bit high
accuracy A/D conversion circuit. Firstly, two sets of tin y
voltage sig nals, one is picked up fr om the bladder and
another is picked up fro m the reference resist or, ar e re-
spectively sent to the Pin1 and Pin2 of the AD8302 after
the fro nt stage differential amplifier (AD620) amplifica-
tion process. The function of AD8302 is calculating the
differenc e of amplitude b et ween the two sets of voltage
signals. In the frequency less than 1MHz, the difference
can be calculated by Equation (2).
12
log( /)
MAGF SLPCP
VRLV VV= +
(2)
where V1 and V2 are respectively the input voltage of the
Pin1 and Pin2, VMAG is t he output corresponding to the
magnitude of the signal level differenc e, RFLSLP is 600
mV/decade or 30 mV/dB with a center-point of 900 mV
(VCP) for 0 dB gain. A range of –30 dB to +30 dB covers
the full-scale swing from 0 V to 1.8 V.
VMAG is fed into the MCU (CC2530) for A/D conver-
sion with a 14-bit high accurac y, using an external 1.8 V
voltage provided by AD8302 as a reference voltage of
A/D conversion. After the A/D conversion, the i mped-
ance of bladder can be figured out by the MCU accord-
ing to VMAG and the reference resistor. Fina lly, impedance
data is transmitted to the human-computer interactio n
module through the Zigbee wireless transmission func-
tion which is integrated into the CC2530. Figure 4
shows the prototype of the data acquisition module with
a portable design.
The human-computer interaction module consists of
two parts: the data receiving module and the monitoring
Figure 4. T he photograph of the dat a acquisition module.
sof tware. The data receiving module, which is inserted
into the computer with a USB interface, could receive the
impedance data fro m the data acquisitio n module through
the Zigbee wireless technology and tra ns mit the data to
the co mputer monitoring software. A MCU (CC2531,
Texas Instrument) is selected as the core of the data re-
ceiving module, which is integrated with Zig bee wireless
transmission function. The monitoring software is de-
veloped based on Labview. It provides the operators with
a good huma n-machine interf ace which we can observe
some impeda nce information such as how the i mpedance
changes by the increasing volume of bladder. We can
also save the measurement res ults for subsequent re-
search and analysis.
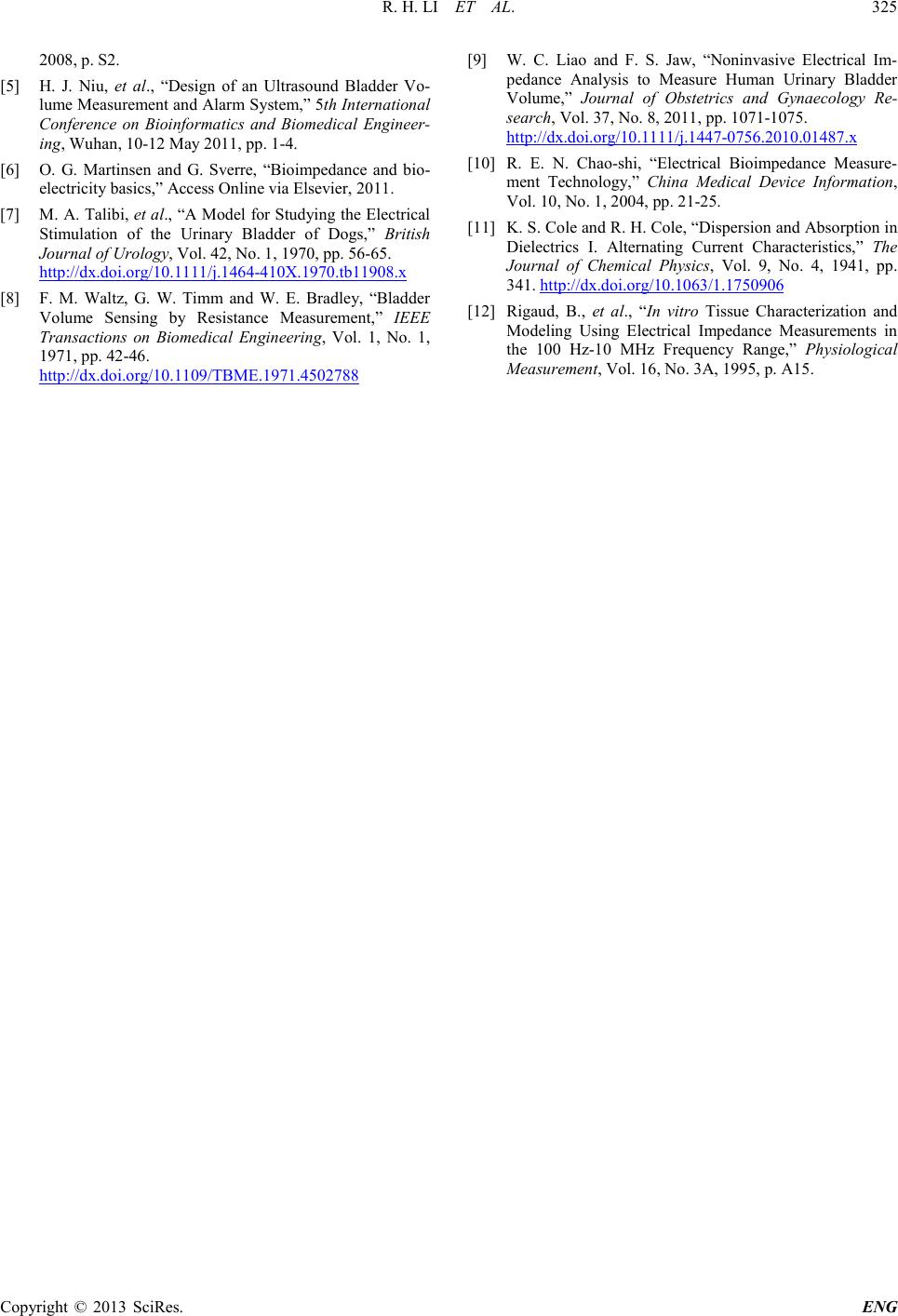
3. Experiments and Results
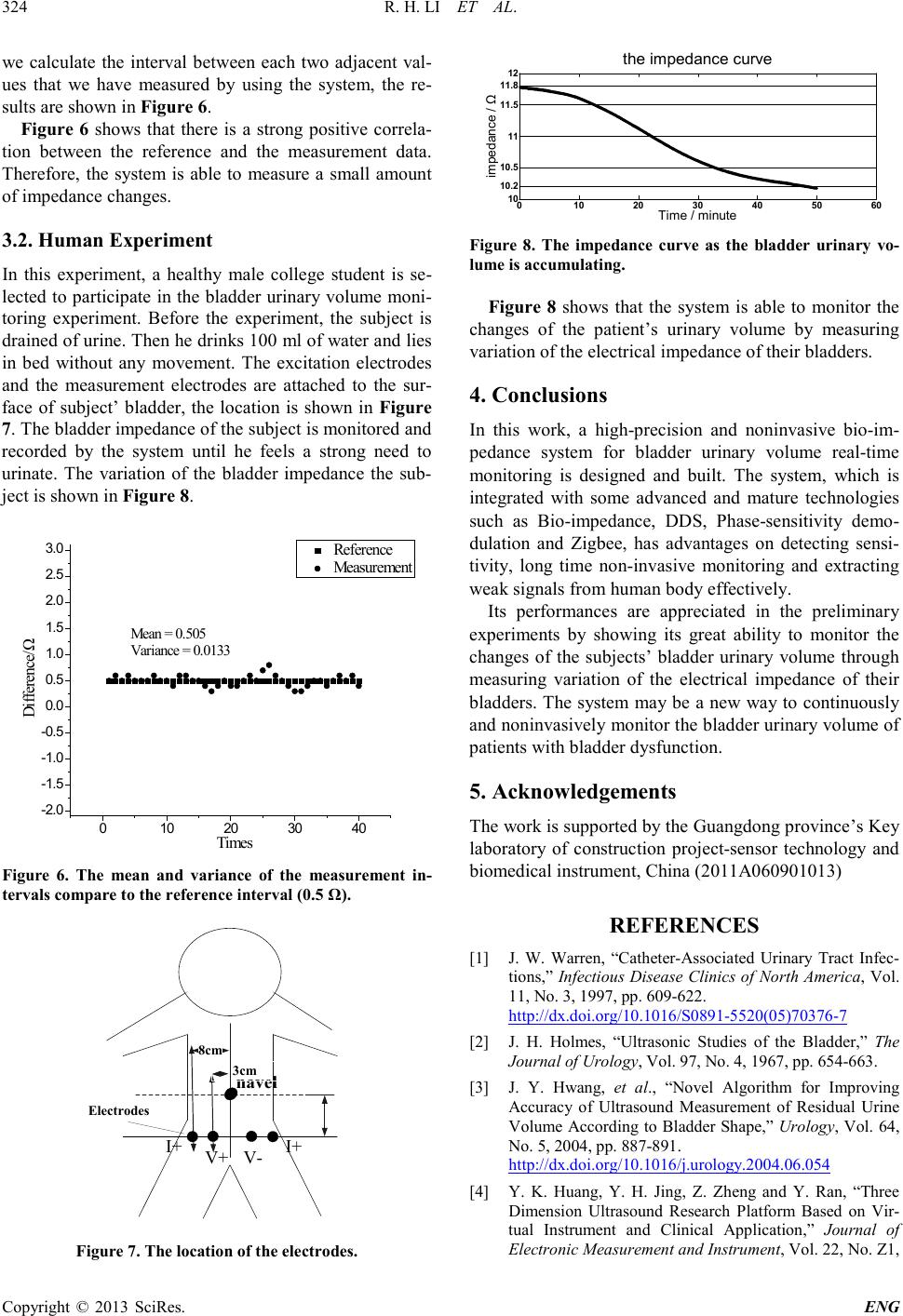
3.1. Accuracy of Measurem ent
As the paper mentioned above, the impedance of the
human bladder shows a downward trend as the increase
of bladder urinary volume [9]. According to previous
laboratory experiments, the impedance values of human
bladder are generally in t he range of 10 Ω - 30 Ω and the
impedance variation of the human bladder ma y be less
than 1 Ω from the beginning of accumulation of urine to
urinating. Therefore, the ability to measure a related
small amount of impedance change needs to be verified.
In this experiment, a varia b le resistance is selected. The
accuracy of it is 1% and the resistance value is 50 Ω. The
excitation electrodes of the system are respectively con-
nected to each end of the r esistor. The measurement
electrodes are also respectively connected to each end of
the resistor, shown in Figure 5. “A+” and “A–” represent
the excitatio n electrodes, “V+” and “V–” rep resent the
measurement electrodes.
Frequency of the exciting current is 50 kHz and
peak-to-peak value is about 1 mA. From 10 Ω to 30 Ω,
we use the system to measure and record every value of
the variable resist ance with an increment of 0.5 Ω. The
Agilent E4980A Pre cisio n LCR meter with accuracy of
0.05% is use d to calibrate the variable resistance and
con fi rm that each t ime our adjustment is accurate. Then,
Figure 5. The connection of accuracy measurement experi-
me nt .