Y. L. SUN ET AL.
Copyright © 2013 SciRes. ENG
the assessment was conducted according to 8 dimensions
and 35 items. The eight dimensions included the physio-
logical function (10 items), physical performance (4
items), general health (5 items), body pain (2 items), vi-
tality (4 items), social communication function (2 items),
emotional functions (3 items) and mental health (5 ite ms).
The score of the physiological function was 10~30
points, the score of body pain was 2 ~ 11 points, and all
the other items were 1 ~ 5 points. The score for each item
was positively proportion al to the quality of life.
The happiness indexes of 93 Patients selected were
assessed and assessment was conducted based on Me-
morial University of Newfoundland scale of Happiness
(MUNSH) [5]. MUNSH contains 24 items. Among the
24 items, 10 items are considered to reflect the positive
and negative emotions, 5 items the positive emotion (PA),
5 items the negative emotion (NA), 14 items positive and
negative experiences, 7 items the positive experience
(PE), and 7 items the negative experience (NE). The total
happiness index: PA-NA + PE-NE. The determination of
score was based on the following rule: that the answer to
each item was “yes” was recorded 2 points, that the an-
swer to each item was “I don’t know” was recorded 1
point, and that the answer to each item was “No” was
recorded 0 point; that the answer to item 19 was “the
residence where he or she is living now” was recorded
points and “any other residence” was recorded 0 point;
that the answer to item 23 was “satisfactory” was rec-
orded 2 points and “unsatisfying” was recorded 0 point.
The range of the total average point was from −24 to +24
points. In order to be easy to calculate the score, 24, as
the constant, was added, and the score range was from 0
to 48; the higher the score the higher the happiness index.
The community nurses implemented their human care
by applying the 10 factors for the human care described
in the theory of human care set up by Dr. Watson J. The
patients were made three appointments a week, the time
for each appointment was not less than 60 minutes, the
care was implemented in a way of a small course or sep-
arately aiming at the particular case for different patients
and the appointment could not be missed. During the
care, the human care were particularly emphasized,
science and humanities knowledge was integrated and
used to communicate with the patients, and the human
care was completed based on 10 factors proposed in the
theory of human care. 10 factors for human included
forming a value system of the human altruism; inculcat-
ing a trust and hope; developing a sensitivity of them-
selves and others; building up a relationship in helping,
trusting and caring; encouraging and accepting the ex-
pression of positive emotions and negative emotions
from the clients; applying scientific methods to solve
problems in the decision-making system; providing a
psychological, social and spiritual environment to sup-
port, protect and correct them; helping meet individual
needs; allowing the presence of existentialism, phenom-
enology and spiritual power. The community nurses
should follow the nature of human care to give the pa-
tients with cancer a psychological support and cultural
care, answer any questions for them or explain the re-
lated successful stories and so on.
After the community human care was implemented
over 3 months, the life quality and the happiness index of
the 93 patients was assessed again based on the life qual-
ity scale (SF-36) and MUN SH.
2.3. Statistical Method
SPSS soft ware was used to analyze the survey data in
this study. The least significant difference (LSD) and
SNK variance analysis methods were applied to compare
a pair of data obtained before the care and after the care.
P < 0.05 meant a significant difference.
3. Results
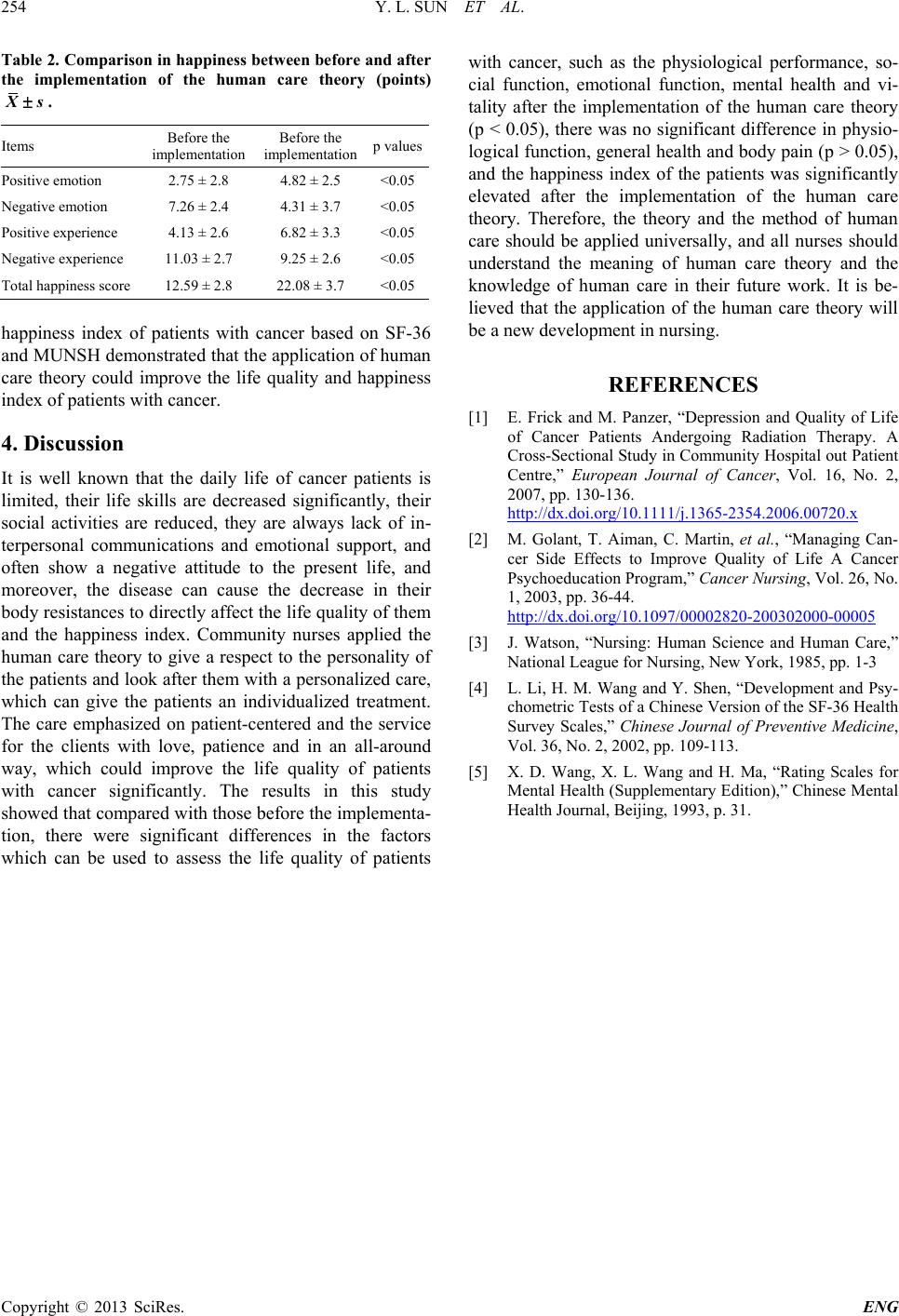
The results showed that both patients’ life quality and
happiness index after the human care were different from
those before the human care, there were significant dif-
ferences in 5 dimensions which could reflect the life
quality of the patien ts, such as physical performance, life
vitality, social communication ability, emotion al function
and spiritual health (<0.05), which were shown in Table
1 in detail; average scores of the positive emotion and
positive experience were significantly increased after the
care (<0.05), those of the negative emotion and the nega-
tive experience were significantly decreased (<0.05), and
the difference in the total average sore of the happiness
index was significant before and after the application of
the human care theory (<0.05), which were shown in
Table 2 in detail. The assessment on the life quality and
Table 1. Comparison in SF-36 score between before and
after the implementation of the human care theory (points)
.
Dimensions
Average sore at the
first assess Average sore after
the human care p values
Physiological
function
13.21 ± 6.12 13.91 ± 4.62 >0.05
Phusical
performance
6.06 ± 2.22 7.81 ± 1.82 <0.05
General health
10.03 ± 3.57 10.52 ± 4.89 >0.05
Physical pain
6.25 ± 3.09 6.94 ± 4.99 >0.05
Life vitality
8.71 ± 4.28 12.29 ± 5.97 <0.05
Social contact
function
6.42 ± 5.83 8.97 ± 2.72 <0.05
Emotional
functions
4.14 ± 3.36 5.76 ± 1.79 <0.05
Spiritual health
8.63 ± 4.18 13.11 ± 2.79 <0.05