Engineering, 2013, 5, 176-180
http://dx.doi.org/10.4236/eng.2013.510B038 Published Online October 2013 (http://www.scirp.org/journal/eng)
Copyright © 2013 SciRes. ENG
Cardiovas cula r Di sea ses Detecting via Pulse Analysis
Jingjing Xia, Simon Liao
Department of Applied Computer Science, University of Winnipeg, Winnipeg, Canada
Email: xia-j@webmail.uwinnipeg.ca, s.liao@uwinnipeg.ca
Received May 2013
ABSTRACT
In this research, we have performed pulse analysis on the data of 127 subjects collected from Department of Cardiology
at Shandong Provincial Hospital in China. By taking the first and third derivatives of an entire pulse wave, we have
firstly identified the locations of wave foot, systolic peak, and reflected point. Then we calculated Reverse Shoulder
Index (RSI) and Ratio of Distance of the evaluated subjects, and correlated them to age, th e history of hypertension, and
different cardiovascular diseases of the subjects.
Keywords: Pulse Wave Analysis; Wave Reflections; RSI; Cardiovascular Diseases Detection
1. Introduction
In the year of 1872, the father of pulse wave analysis,
Mahomed, wrote the following statement in his research
[1], “Since the information that the pulse affords is of so
great importance, and so often consulted, surely it must
be to our advantage to appreciate fully all it tells us, and
to draw from it every detail that it is capable of impart-
ing”. Since then more and more scientists put lots of ef-
forts to discover the important points from pulse wave
and connected them to age and different kinds of diseases,
especially cardiovascular diseases, for instance, hyper-
tension, acute myocardial infarction and coronary heart
disease.
In 19th century, pulse wave was recorded invasively
from the aortic ascending artery. Therefore, during that
period, pulse wave analysis is mainly concentrated in
ascending aorta. The invasive method has lots of short
comings. It is greatly inconvenient to be obtained and
hard to keep consistency of wave form. Later on, scien-
tists developed noninvasively methods for obtaining
pulse wave. Furthermore, not only the pulse wave of aor-
tic central artery, but also waves of peripheral arterial,
carotid, brachial and femoral arteries can be recorded. In
our study, pulse waves were recorded noninvasively
from index finger using a finger clip with infra-red sen-
sor.
The noninvasi vely met hod of rec ording pul se wave does
make a great contribution to the process of pulse analysis.
Among all related research of pulse wave, the study of
reflection of the primary pressure pulse along the human
arterial tree has important significance in medical re-
search. In 1890, Murgo et al. pointed out that wave ref-
lection was h ighly ass ociated with age [2]. Both Mitchell
et al. in 2004 [3] and O’Rourke, Nichols and in 2005 [4]
proved there was inextricable link between wave reflec-
tion and age. Furthermore, Eshan et al. [5] correlated
wave reflection with cardiovascular risks. They empha-
sized that it may be a useful measure of assessing overall
rick for coronary artery disease. Certainly wave reflec-
tion is a momentous aspect for pulse analysis, and it is a
different issue between central aortic pulse pressure and
peripheral arterial pulse pressure. For central aortic pres-
sure, augmentation index is used as an incidence of re-
flected waves among total pulse pressure, as mentioned
in [6]. For peripheral arterial pressure, another index
would be adopted, which is RSI (Reverse Shoulder In-
dex). Due to all of the pulse waves for our study are rec-
orded from peripheral artery, we applied the method dis-
cussed in [7]. According to [7], we verified the wave foot
by the first derivative form and located the reflected
point and systolic peak via the third derivative curve. RSI
(Reverse Shoulder Index) and Ratio of Distance were
calculated using those two points. In the following part,
we will introduce the details of the method. Finally, we
associated those two parameters with age, hypertension,
coronary artery disease and chest pain. Results will be
shown in the following statement.
2. Subjects and Device
We evaluated 127 subjects from August, 2008 to August,
2010 in Department of Cardiology at Shandong Provin-
cial Hospital in China. All the pulse waves were recorded
noninvasively by finger clip with infra-red senor. The
device is made by Anhui Huake Electronic Technical
Research Institute in China, and the model of the device
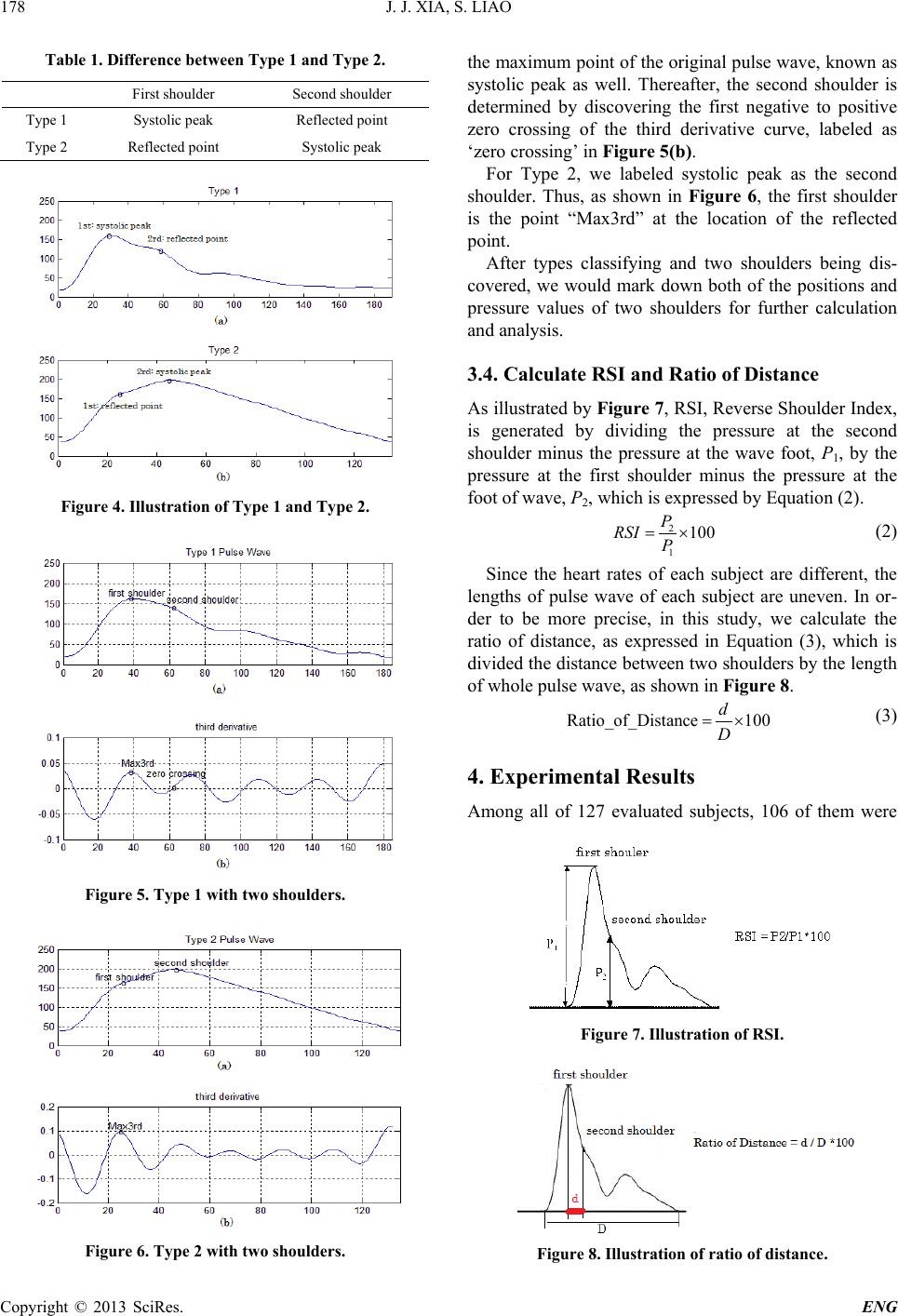
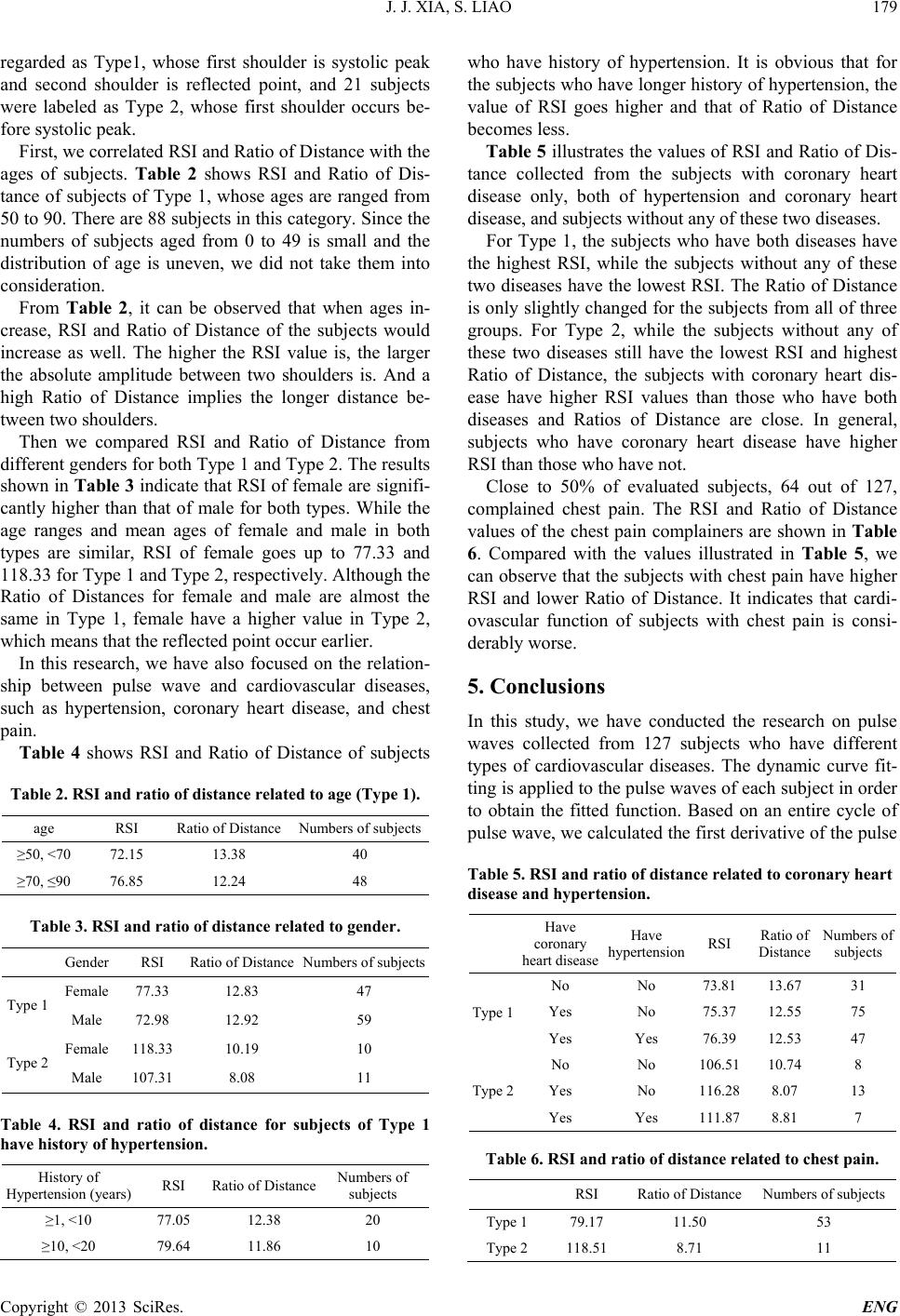
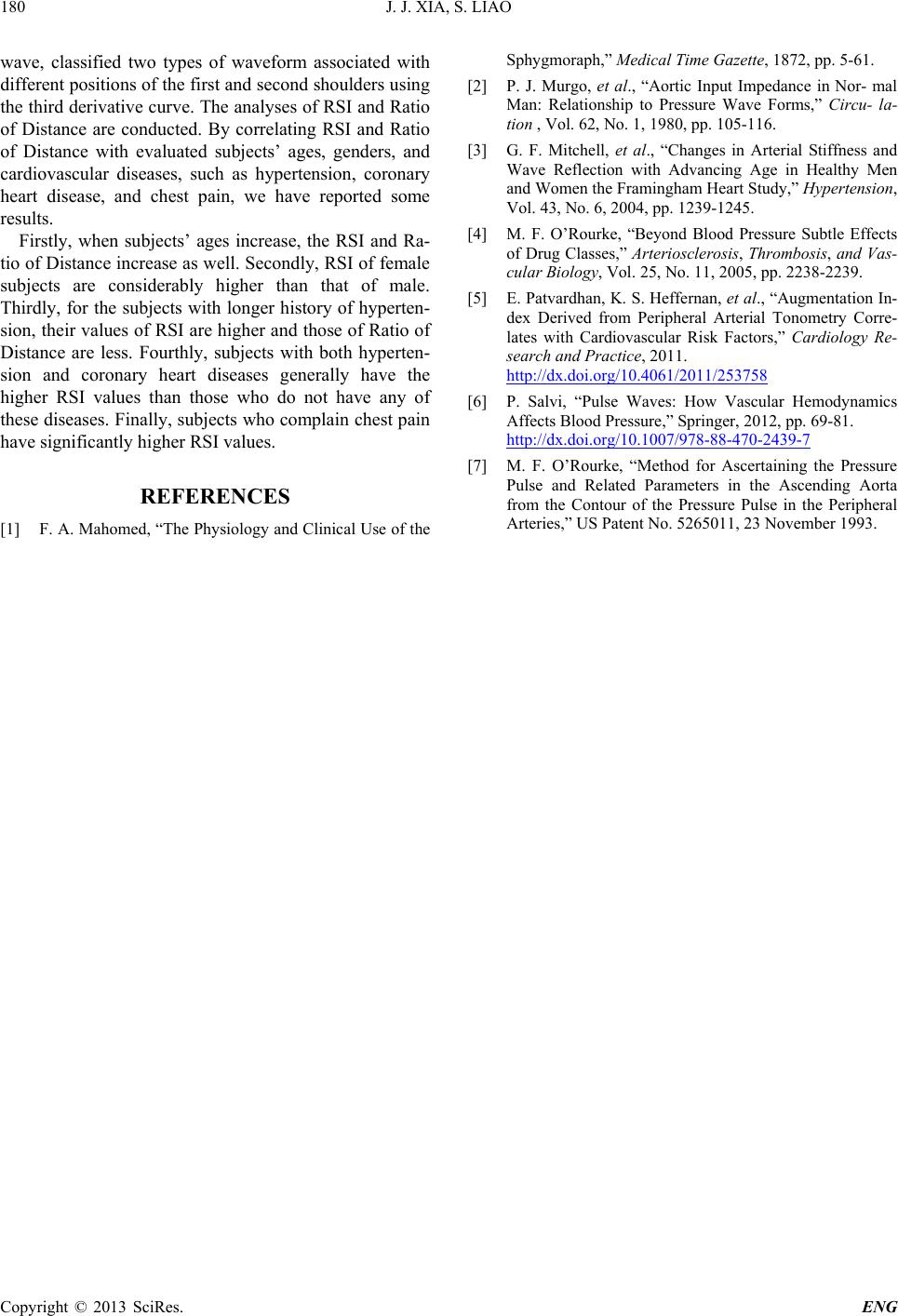
is HKG-07C, shown as Figure 1. The data were col-