M. SALVI ET AL. 475
Arthroscopy was performed using the standard anter-
olateral and anteromedial portals and revealed no menis-
cus anomalies or tears and no cartilage damage of the
lateral femoral condyle, sulcus and patellae.
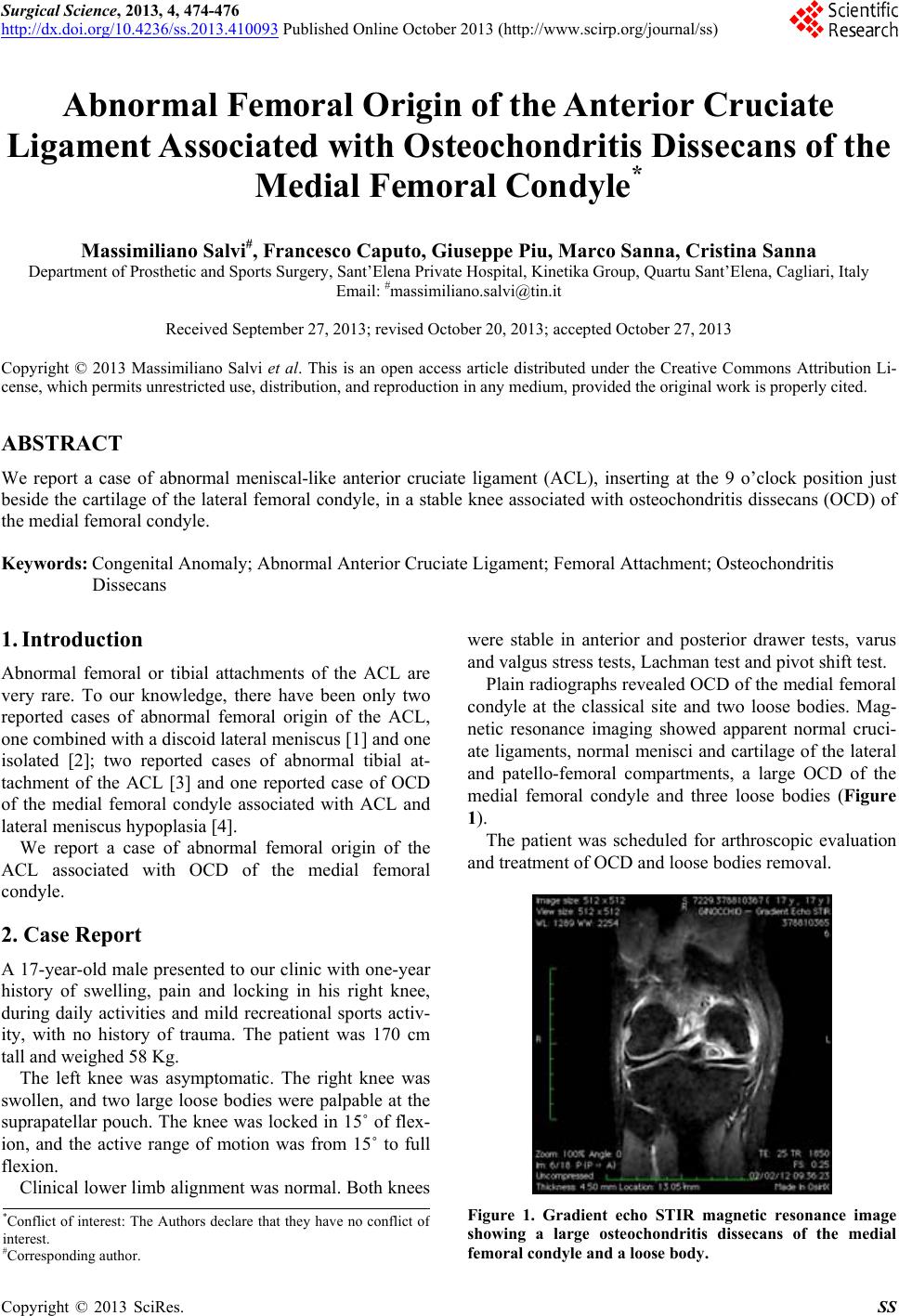
A large (2 × 4 cm) OCD of the medial femoral condyle
and five loose bodies, two of which were locatedin the
posteromedial compartment, were found.
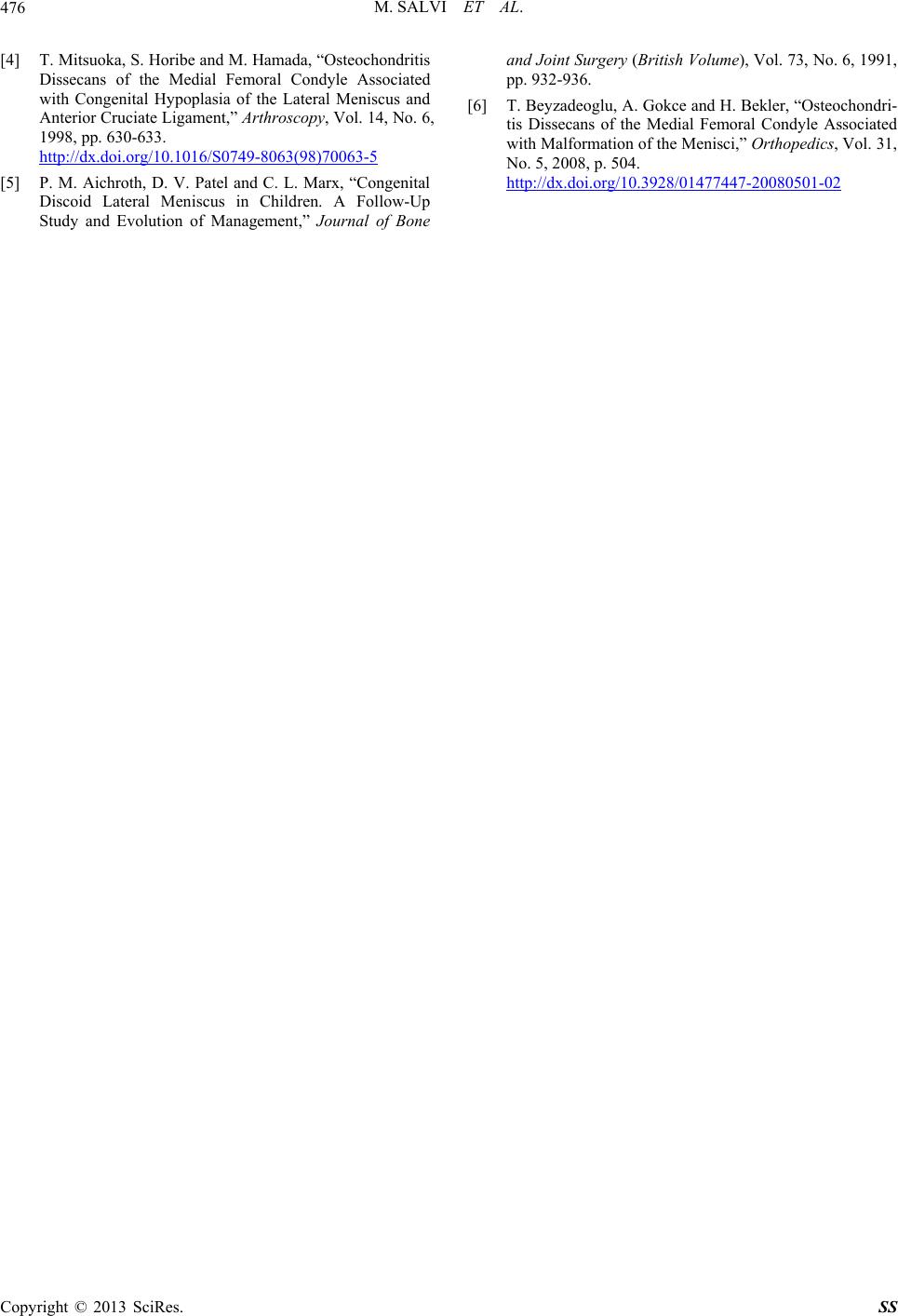
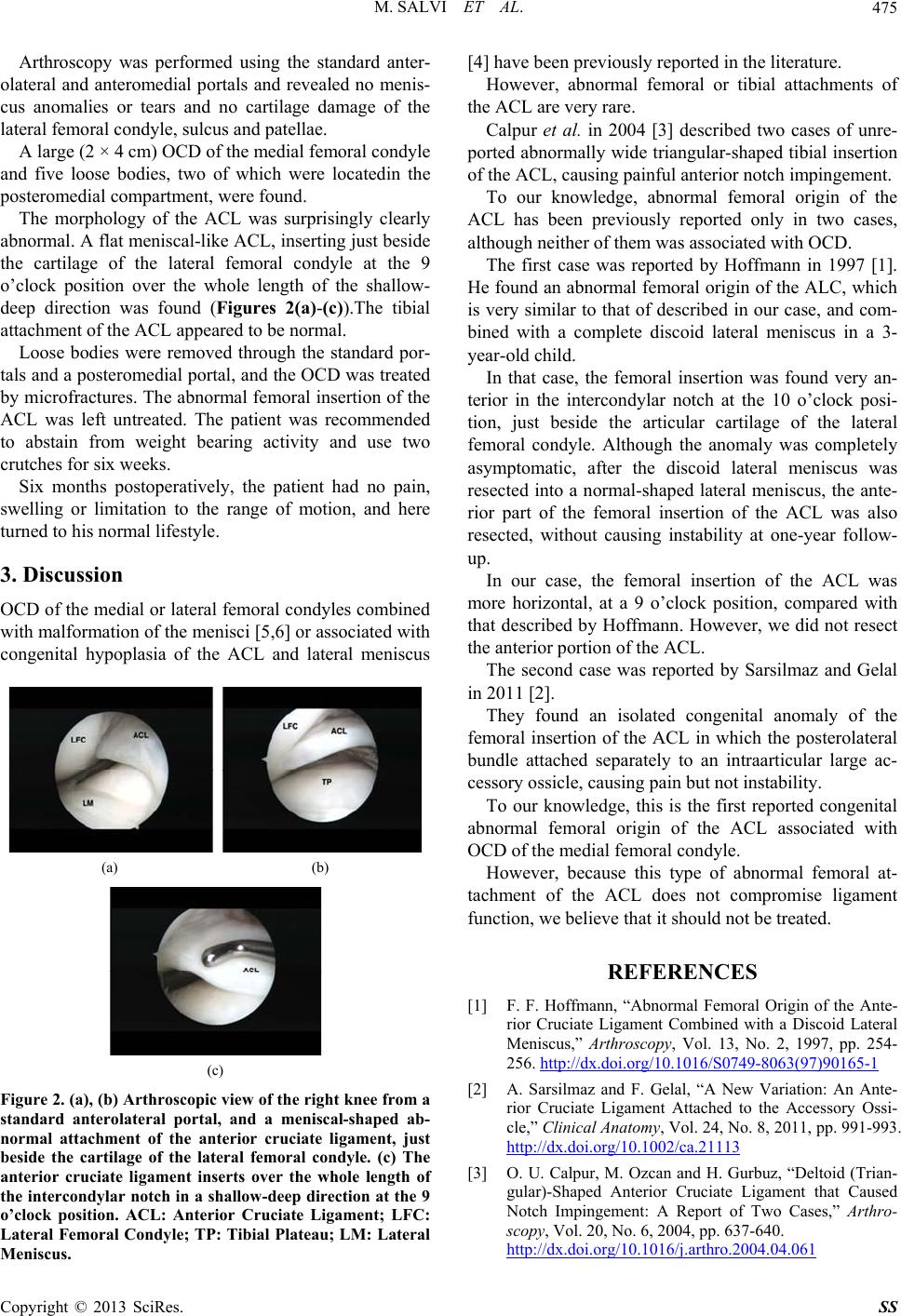
The morphology of the ACL was surprisingly clearly
abnormal. A flat meniscal-like ACL, inserting just beside
the cartilage of the lateral femoral condyle at the 9
o’clock position over the whole length of the shallow-
deep direction was found (Figures 2(a)-(c)).The tibial
attachment of the ACL appeared to be normal.
Loose bodies were removed through the standard por-
tals and a posteromedial portal, and the OCD was treated
by microfractures. The abnormal femoral insertion of the
ACL was left untreated. The patient was recommended
to abstain from weight bearing activity and use two
crutches for six weeks.
Six months postoperatively, the patient had no pain,
swelling or limitation to the range of motion, and here
turned to his normal lifestyle.
3. Discussion
OCD of the medial or lateral femoral condyles combined
with malformation of the menisci [5,6] or associated with
congenital hypoplasia of the ACL and lateral meniscus
(a) (b)
(c)
Figure 2. (a), (b) Arthroscopic view of the right knee from a
standard anterolateral portal, and a meniscal-shaped ab-
normal attachment of the anterior cruciate ligament, just
beside the cartilage of the lateral femoral condyle. (c) The
anterior cruciate ligament inserts over the whole length of
the intercondylar notch in a shallow-deep direction at the 9
o’clock position. ACL: Anterior Cruciate Ligament; LFC:
Lateral Femoral Condyle; TP: Tibial Plateau; LM: Lateral
Meniscus.
[4] have been previously reported in the literatu re.
However, abnormal femoral or tibial attachments of
the ACL are very rare.
Calpur et al. in 2004 [3] described two cases of unre-
ported abnormally wide triangu lar-shaped tibial insertion
of the ACL, causing painful anterior notch impingement.
To our knowledge, abnormal femoral origin of the
ACL has been previously reported only in two cases,
although neither of them was associated with OCD.
The first case was reported by Hoffmann in 1997 [1].
He found an abnormal femoral origin of the ALC, which
is very similar to that of described in our case, and com-
bined with a complete discoid lateral meniscus in a 3-
year-old child.
In that case, the femoral insertion was found very an-
terior in the intercondylar notch at the 10 o’clock posi-
tion, just beside the articular cartilage of the lateral
femoral condyle. Although the anomaly was completely
asymptomatic, after the discoid lateral meniscus was
resected into a normal-shaped lateral meniscus, the ante-
rior part of the femoral insertion of the ACL was also
resected, without causing instability at one-year follow-
up.
In our case, the femoral insertion of the ACL was
more horizontal, at a 9 o’clock position, compared with
that described by Hoffmann. However, we did not resect
the anterior portion of the ACL.
The second case was reported by Sarsilmaz and Gelal
in 2011 [2].
They found an isolated congenital anomaly of the
femoral insertion of the ACL in which the posterolateral
bundle attached separately to an intraarticular large ac-
cessory ossicle, causing pain but not instability.
To our knowledge, this is the first reported congenital
abnormal femoral origin of the ACL associated with
OCD of the medial femoral condyle.
However, because this type of abnormal femoral at-
tachment of the ACL does not compromise ligament
function, we be li e ve that it should not be trea te d.
REFERENCES
[1] F. F. Hoffmann, “Abnormal Femoral Origin of the Ante-
rior Cruciate Ligament Combined with a Discoid Lateral
Meniscus,” Arthroscopy, Vol. 13, No. 2, 1997, pp. 254-
256. http://dx.doi.org/10.1016/S0749-8063(97)90165-1
[2] A. Sarsilmaz and F. Gelal, “A New Variation: An Ante-
rior Cruciate Ligament Attached to the Accessory Ossi-
cle,” Clinical Anatomy, Vol. 24, No. 8, 2011, pp. 991-993.
http://dx.doi.org/10.1002/ca.21113
[3] O. U. Calpur, M. Ozcan and H. Gurbuz, “Deltoid (Trian-
gular)-Shaped Anterior Cruciate Ligament that Caused
Notch Impingement: A Report of Two Cases,” Arthro-
scopy, Vol. 20, No. 6, 2004, pp. 637-640.
http://dx.doi.org/10.1016/j.arthro.2004.04.061
Copyright © 2013 SciRes. SS