V. V. GEORGE ET AL.
436
bleeding was encountered that required direct visualiza-
tion for control. However, our overall conversion rate
was in line with other reported experiences [11]. Addi-
tionally, we believe that conversion of the procedure
from a single-port approach should not be deemed a fail-
ure as much as it represents better judgment on the part
of the surgeon to change direction when the individual
scenario requires it.
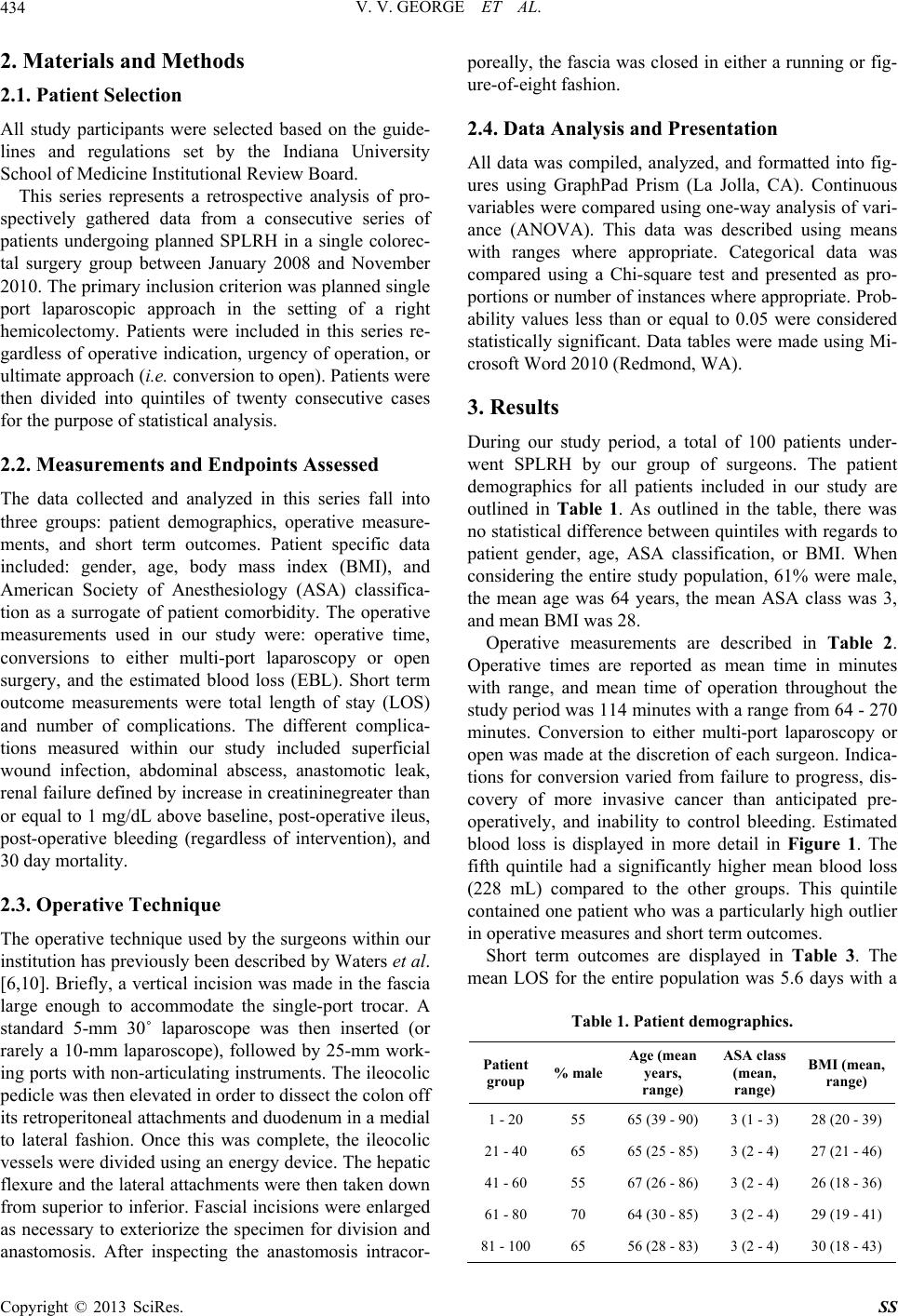
Measurement of blood loss during an operation can be
interpreted in various ways. A large amount of blood loss
to one surgeon may mean that the surgery was particu-
larly difficult and that it may be expected that the patient
has a higher risk of having a post-operative complication,
but another surgeon may see that same blood loss and
interpret it as poor performance of the operating surgeon .
With that in mind, there was no diff erence in mean blood
loss across the quintiles until the final group. As previ-
ously mentioned, this was due to on e particular patien t in
that group who had a significant blood loss due to injury
to the middle colic vein. Interestingly, as the series went
on, there was an increase in the range of blood loss.
Our short term outcomes with regard to length of stay
and peri-operative morbidity did not change through the
progression of cases. Rather, both remained consistent
with other reported series of both single-port and multi-
port laparoscopic colectomies [10,12-14]. This suggests
that the key to determining patient recovery may not lie
within the approach between single or multi-port laparo-
scopy, and instead hinders on the nature of the operation
itself and/or inherent patient factors. Importantly, the use
of the single-port approach did not negatively impact the
rates of post-operative morbidity.
When examining the data presented here, it is impor-
tant to take into account a few limitations of this study.
These cases were performed by multiple surgeons in a
group. However, one surgeon either performed or as-
sisted in the majority of the cases ex amined in this series,
and all of our surgeons have similar training, experience
with colorectal surgery, and method to performing a
SPLRH, reducing the inter-surgeon variability. We did
look at the data from a single surgeon’s perspective but
did not find significant difference between his and the
rest of the group’s measures. Another limitation is that
the role of residents and fellows cannot be quantified
within the data. However, as would be expected, there is
a graded role of involvement over time with experience
by both the trainee and staff surgeon.
The introduction of new surgical techniques requires
completing a number of procedures before becoming
proficient. With the increasing presence of single-port
laparoscopy within surgical practice, it is important to
understand how long it takes a surgeon to become facile
with this evolving approach. Prior studies have already
examined the learning curve for various single-port
laparoscopic operations [7-9], and have concluded that
the learning curve is fairly short for those already ex-
perienced in their field. However, this is the first report
examining the learning curve with regards to colorectal
surgery. Whether this approach will become a part of an
average colorectal surgeon’s practice has yet to be de-
termined, and further investigations to understand its
potential long term benefits an d hazards are needed.
5. Conclusion
The learning curve for SPLRH is short for colorectal
surgeons who already experienced with conventional lap-
aroscopic operations. Surgeons who desire to start offer-
ing their patients a single-port approach to right hemi-
colectomy can do so without significant increase in op-
erative time, length of stay, or per-operative morbidity.
Surgeons will need to become facile with SPLRH to keep
up with patients’ increasing awareness and desire for this
approach.
REFERENCES
[1] P. Bucher, F. Pugin and P. Morel, “Single Port Access
Laparoscopic Right Hemicolectomy,” International Jour-
nal of Colorectal Disease, Vol. 23, No. 10, 2008, pp.
1013-1016.
http://dx.doi.org/10.1007/s00384-008-0519-8
[2] A. N. Fader and P. F. Escobar, “Laparoendoscopic Sin-
gle-Site Surgery (LESS) in Gynecologic Oncology: Tech-
nique and Initial Report,” Gynecologic Oncology, Vol.
114, No. 2, 2009, pp. 157-161.
http://dx.doi.org/10.1016/j.ygyno.2009.05.020
[3] G. Navarra, E. Pozza, S. Occhionorelli, P. Carcoforo and
I. Donini, “One-Wound Laparoscopic Cholecystectomy,”
British Journal of Surgery, Vol. 84, No. 5, 1997, p. 695.
http://dx.doi.org/10.1002/bjs.1800840536
[4] L. E. Ponsky, E. E. Cherullo, M. Sawyer and D. Hartke,
“Single Access Site Laparoscopic Radical Nephrectomy:
Initial Clinical Experience,” Journal of Endourology, Vol.
22, No. 4, 2008, pp. 663-666.
http://dx.doi.org/10.1089/end.2007.0427
[5] A. A. Saber, T. H. El-Ghazaly and D. B. Minnick, “Sin-
gle Port Access Transumbilical Laparoscopic Roux-en-Y
Gastric Bypass Using the SILS Port: First Reported
Case,” Surgical Innovation, Vol. 16, No. 4, 2009, pp.
343-347. http://dx.doi.org/10.1177/1553350609354604
[6] J. A. Waters, B. M. Rapp, M. J. Guzman, A. L. Jester, D.
J. Selzer, B. W. Robb, B. J. Johansen, B. M. Tsai, D. C.
Maun and V. V. George, “Single-Port Laparoscopic Right
Hemicolectomy: The First 100 Resections,” Diseases of
the Colon & Rectum, Vol. 55, No. 2, 2012, pp. 134-139.
http://dx.doi.org/10.1097/DCR.0b013e31823c0ae4
[7] M. Gawart, S. Dupitron and R. Lutfi, “Laparoendoscopic
Single-Site Gastric Bands versus Standard Multiport Gas-
tric Bands: A Comparison of Technical Learning Curve
Measured by Surgical Time,” The American Journal of
Surgery, Vol. 203, No. 3, 2012, pp. 327-329.
Copyright © 2013 SciRes. SS