L. Zhang et al. / Case Reports in Clinical Medicine 2 (201 3) 386-389
Copyright © 2013 SciRes. OPEN ACCESS
388
gins were free of tumor.
3. DISCUSSION
Although many large randomized trials with the la-
paroscopic approach in colon cancer had demonstrated
equivalent oncologic efficacy with similar overall sur-
vival, disease-free survival and local and distant recur-
rences [10-12], the relevant data of large randomized
trials with the laparoscopic approach in rectal cohort is
scarce, hampering its widely accepted.
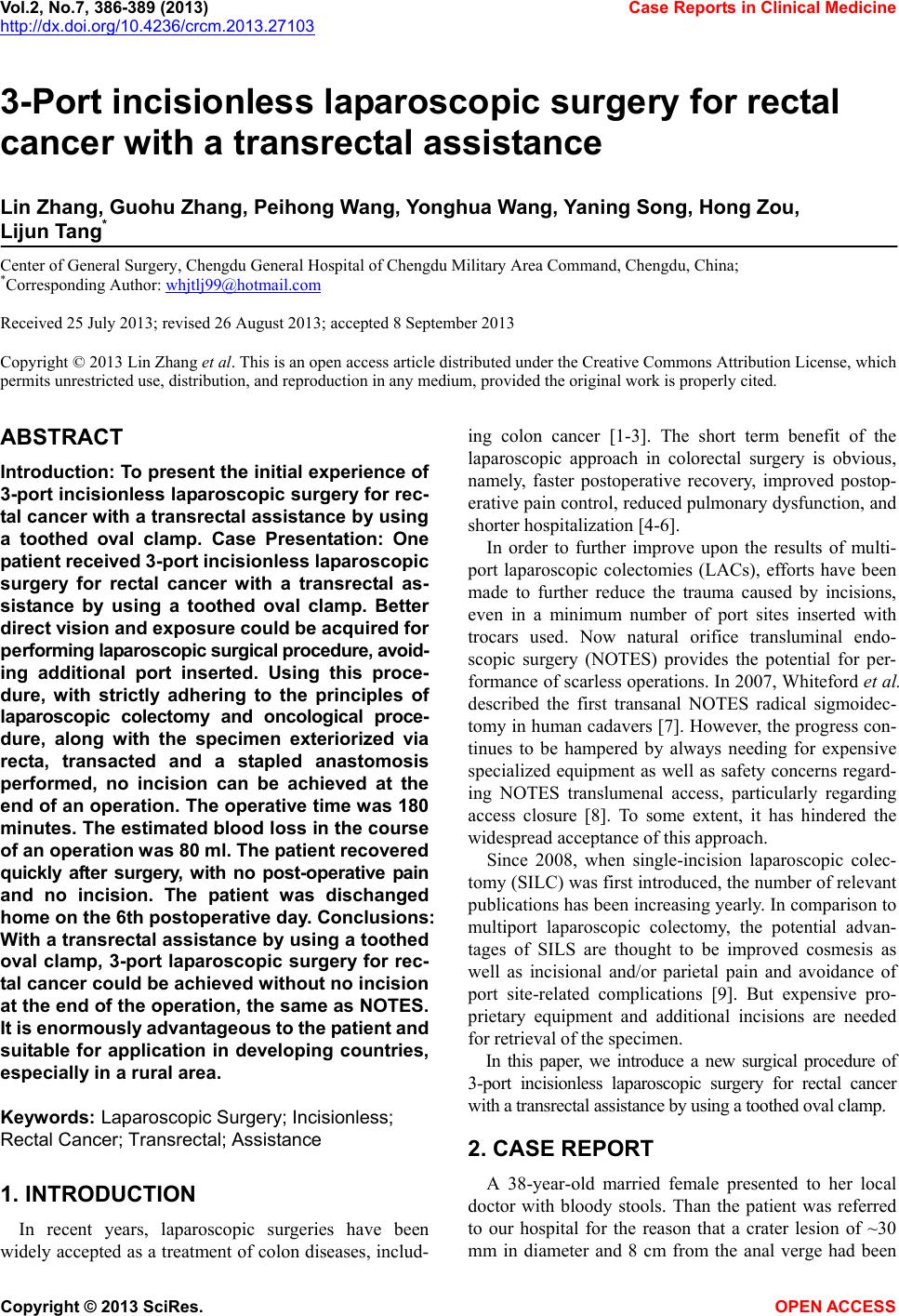
Overall laparoscopic rectal resection for malign ancy is
technically more demanding in that concerns about nerve
preservation, complete total mesorectal excision, and
adequate lymph node yield are still unsettled in this set-
ting. But the remarkable magnified view provided by the
monitor of laparoscopic operation system has become
more advantageous and fascinating and enables safe and
accurate manipulation at sites such as the deep pelvic
floor, lower bladder, posterior surface of the prostate and
anal region, where visualization is difficult to achieve
during open surgery and manipulation is usually carried
out under nearly blind conditions [13].
In order to further improve upon the results of LACs,
efforts have been made to further reduce the trauma
caused by incisions, even in a minimum number of port
site inserted with trocars used. This results in a paradox.
on one hand, both operator and patient persue scarless or
minor insicions; on the other hand, with reduction num-
ber of port site, exposure of operating site should be
more difficult for performing adequately surgical proce-
dure. So we put forward a useful laparoscopic assisting
approach with a transrectal assistance by using toothed
oval clamp.
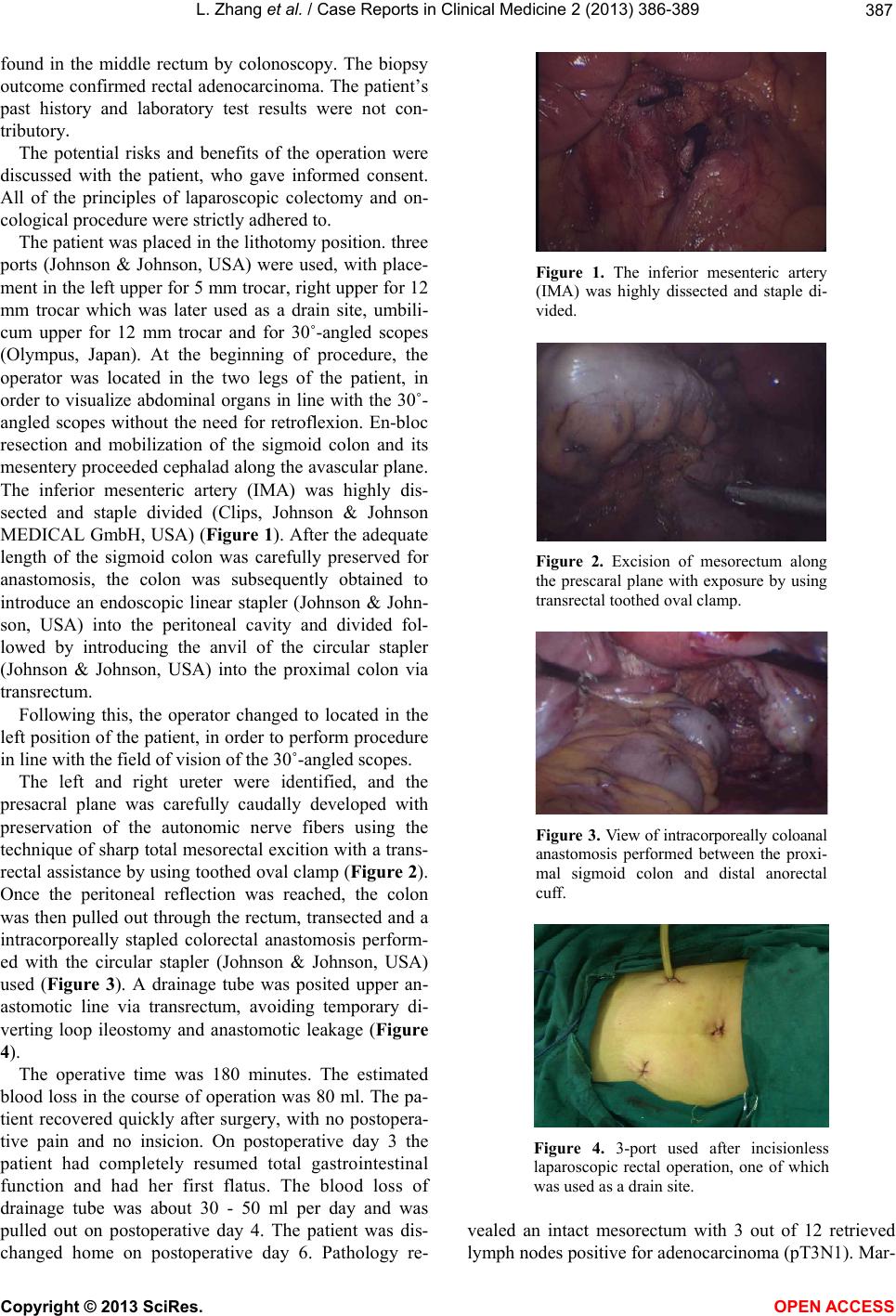
In our opinion, a new transrectal laparoscopic assisting
approach offers multiple advantages: 1) with respect to
laparoscopic surgery for rectal cancer,the sharp angle of
the sacral promontory and narrow pelvis hindered the
proximal dissection of rectal wall and its attached mes-
entery. To overcome those anatomic constraints, expo-
sure turned out to be more important. Based on our early
experience, with a transrectal assistance by using toothed
oval clamp performed by second assistant, operator
could acquire better direct vision and exposure for per-
forming laparoscopic surgical procedure, avoiding addi-
tional port inserted; 2) Patients, both male and female,
independent of age and body shape, usually dislike scars,
not only for cosmetic reasons but because scars indicate
they have undergone treatment before. This resulted in
NOTES, eliminating the incision through the abdominal
wall and using natural orifices,meeting the aspirations of
the patients and su rgeons [14]. But in the level of LACs,
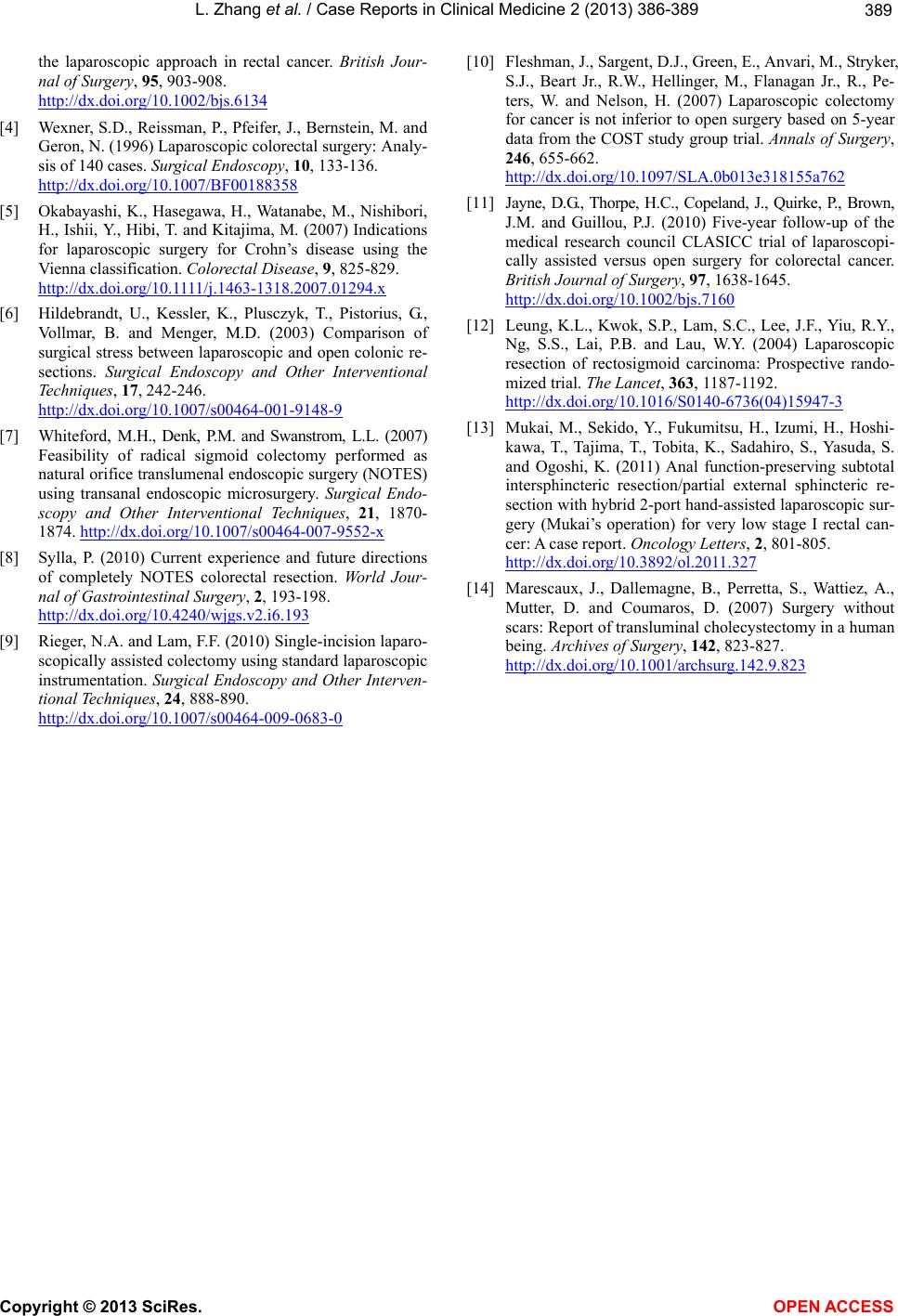
minor incision always needed. Using our above-men-
tioned procedure, along with the specimen exteriorized
via transrectal, transacted and a stapled anastomosis per-
formed, incisionless can be achieved at the end of opera-
tion, same as NOTES; 3) Our new transrectal laparo-
scopic assisting device is much cheaper than instrument
of other minimally invasive surgeries in that it is a sim-
ple device whose cost is approximately 50 USD. So it is
suitable for application in developing countries, espe-
cially in a rural area.
Nevertheless,we have to refer some caveats emerged
in our initially experience with this technique. Firstly,
strict selection of patients for this approach include tho se
with biopsy proven resectable rectal malignancy located
4 - 12 cm from anal verge who are otherwise eligible to
undergo standard open or laparoscopic low anterior re-
section with temporary diverting stoma. Meanwhile tu-
mors must be preoperatively staged as node negative, T1,
T2 or T3 based on pelvic MRI with no evidence of me-
tastasis on staging CT scans. Secondly, lesions of eligi-
ble patients which causing no more than 50% stenosis of
the lumen, as well as better mechanical bowel prepara-
tion, could ensure a satisfied operation outcome, avoid-
ing temporary diverting loop ileostomy and anastomotic
leakage.
4. CONCLUSION
On the basis of our preliminary experience, we believe
that with a transrectal assistance by using a toothed oval
clamp, 3-port laparoscopic surgery for rectal cancer can
be done without an incision at the end of the operation,
same as NOTES. With this useful technique, made from
commonly used and relatively inexpensive surgical equip-
ment, avoiding long and complex learning curves, op-
erator could acquire much more exposure, assistance
during performing surgical procedure. Above all, it is
suitable for application in developing countries, espe-
cially in a rural area.
REFERENCES
[1] Bonjer, H.J., Hop, W.C., Nelson, H., Sargent, D.J., Lacy,
A.M., Castells, A., Guillou, P.J., Thorpe, H., Brown, J.,
Delgado, S., Kuhrij, E., Haglind, E. and Påhlman, L.
(2007) Transatlantic laparoscopically assisted vs open co-
lectomy trials study group. Laparoscopically assisted vs
open colectomy for colon cancer: A meta-analysis. Ar-
chives of Surgery, 142, 298-303.
http://dx.doi.org/10.1001/archsurg.142.3.298
[2] Nelson, H., Sargent, D.J., Wieand, H.S., Fleshman, J.,
Anvari, M., Stryker, S.J., Beart Jr., R.W., Hellinger, M.,
Flanagan Jr., R., Peters, W. and Ota, D. (2004) A com-
parison of laparoscopically assisted and open colectomy
for colon cancer. The New England Journal of Medicine,
350, 2050-2059.
http://dx.doi.org/10.1056/NEJMoa032651
[3] Laurent, C., Leblanc, F., Bretagnol, F., Capdepont, M.
and Rullier, E. (2008) Long-term wound advantages of