Paper Menu >>
Journal Menu >>
 Engineering, 2012, 5, 146-149 doi:10.4236/eng.2012.410B038 Published Online October 2012 (http://www.SciRP.org/journal/eng) Copyright © 2012 SciRes. ENG Investigation of Bone Ratios for Prenatal Fetal Assessment in Taiwanese Population Feng-Yi Yang, Yi -Li Lin Department of Biomedical Imaging an d Radiological Sciences , School of Bi om edical Science and Engineering, Nati onal Yang-Ming University Email: fyyang@ym.edu.tw, daniel310546@gmail.com Received 2012 ABSTRACT The purpose of this study is to calculate the ratios of fetal limb bone to nasal bone length (NBL) obtained by transabdominal ultra- sound between 19 and 28 weeks of gestation. Cross-section al data were obtained from 1408 women with singleton pregnancies who underwent an advanced prenatal ultrasound examination from August 2006 to September 2008. The single measurement plane of fetal limb bones was on the longest section of each structure with appropriate image magnification. To assess repeatability of the intraob server, two r epeated measu rements wer e obt ained in 44 fetuses. The ratio of fetuses with bi parietal diameter (BP D)/N BL was compared with those of fetal limb bones/NBL. The mean ratio was found between fetal NBL measurements and BPD (7.240), hu- merus length (HL) (4.807), radius length (RL) (4.157), ulna length (UL) (4.502), femur length (FL) (5.131), tibia length (TL) (4.528), and fibula length (FiL) (4.507). The reference ranges of fetal long bone length/NBL ratios for the second trimester was established by transabdominal sonography. There were no significant increases in these ratios with gestational age, es pecially the HL/NBL ratio. Keywords: Nasal Bone Length; Limb Bone; Ratio; Second Trimester; Ultrasound 1. Introduction In aneuploid chromosomes, Down syndrome has a high inci- dence rate in newborns [1]. The methods of screening for chromosome anomalies, excluding amniocentesis, rely on ma- ternal age and maternal serum biochemical markers. Recently, fetal genetic ultrasound screening has been proposed as an ad- ditional screening tool for aneuploidy [2]. Down syndrome fetuses usually have facial abnormalities, with especially an absent fetal nasal bone (NB) or NB hypoplasia due to delayed NB ossification, which have been observed as a fetal sono- graphic soft marker of Down syndrome [3]. Recent reports suggested that evaluation of the fetal NB might help to identify fetuses at risk of Down syndrome. It has been reported that about 65% of Down syndrome fetuses have absent or short NB in fetal NB screening at the first and second trimesters [4]. Only 1~2% of normal karyotype fetuses have been ob served [5-7]. Down syndrome and absent or hypoplastic fetal NB show similar evidence of high sensitivity, high speci- ficity, and low false-positive rate for Down syndrome screening by fetal NB examination [8-11]. Published data have shown that when comparing Down Syn- drome fetuses with euploid fetuses, Down Syndrome fetuses were more frequently associated with NB hypoplasia [12-15]. Reviewing several past studies, in addition to discussing the relationship between nasal bone length (NBL) and gestational age or biparietal diameter (BP D), the BPD/NB L ratio ≥ 10 and ≥ 11 were proposed for the definitions of nasal bone hypoplasia in the second tri mester [ 13,15-19]. The fetal NB assessment is a very important part of prenatal fetal examination. It is a useful diagnostic and screening tool for Down syndrome. The purpose of this study was to investi- gate the distributions of fetal limb bones length with respect to NBL and to compare the differences of ratios between fetal BPD/NBL an d fetal limb bone/NBL. 2. Methodology 2.1. Subjects The cross-sectional fetal long bone measurements were carried out with 1408 pregnancies as a part of advanced prenatal ultra- sound examination from August 2006 to September 2008. The gestational age of the fetuses was calculated from the accurate estimated date of confinement obtained from patients. If the estimated date of confinement was uncertain, the difference between the ultrasonically estimated gestational age and deter- mined gestational age was assumed t o be less than 10 days [20]. The exclusion criteria included previous history of chromosome abnormalities, fetal structural anomalies, and maternal compli- cations. 2.2. Ultrasound The fetal NBL was measured in the strict sagittal view of the fetal head under appropriate image magnification (Figure 1) [5,21]. independent document. Please do not revise any of the current designations. In order to avoid false finding that the NB was either absent or shortened, the angle of the fetal nose was maintained be- tween 45° and 135° [12,22]. The BPD was measured on the transverse axial section of the fetal head – which included the midline falx and the thalami symmetrically positioned on either side o f the falx – from the outer edge of the nearer parietal bone to the inner edge of the more distant parietal bone whilst visua- 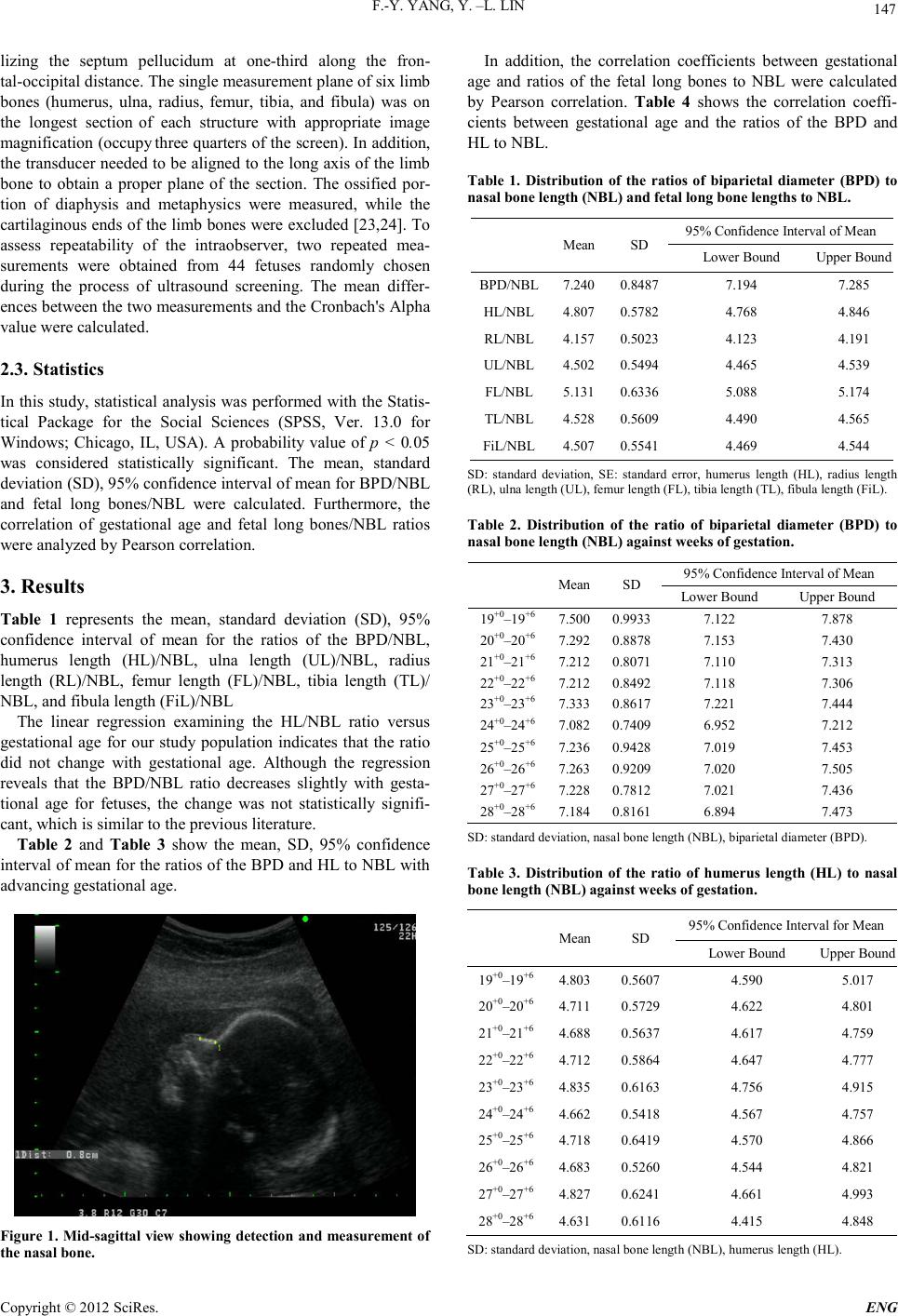 F.-Y. YANG, Y. –L. LIN Copyright © 2012 SciRes. ENG 147 lizing the septum pellucidum at one-third along the fron- tal-occipit al dist ance. Th e single measu re ment pl ane of six li mb bones (humerus, ulna, radius, femur, tibia, and fibula) was on the longest section of each structure with appropriate image magnificat ion (occup y three quarters of th e screen). In addition, the transducer needed to be aligned to the long axis of the limb bone to obtain a proper plane of the section. The ossified por- tion of diaphysis and metaphysics were measured, while the cartilagin ous ends o f the limb bones were excluded [23,24]. To assess repeatability of the intraobserver, two repeated mea- surements were obtained from 44 fetuses randomly chosen during the process of ultrasound screening. The mean differ- ences between the two measurements and the Cronbach's Alpha value were calculated. 2.3. Statistics In this study, statistical analysis was performed with the Statis- tical Package for the Social Sciences (SPSS, Ver. 13.0 for Windows; Chicago, IL, USA). A probability value of p < 0.05 was considered statistically significant. The mean, standard deviation (SD), 95% confid ence in terval o f mean for BP D/NBL and fetal long bones/NBL were calculated. Furthermore, the correlation of gestational age and fetal long bones/NBL ratios were analyzed by Pearson correlation. 3. Results Table 1 represents the mean, standard deviation (SD), 95% confidence interval of mean for the ratios of the BPD/NBL, humerus length (HL)/NBL, ulna length (UL)/NBL, radius length (RL)/NBL, femur length (FL)/NBL, tibia length (TL)/ NBL, and fibula length (FiL)/NBL The linear regression examining the HL/NBL ratio versus gestational age for our study population indicates that the ratio did not change with gestational age. Although the regression reveals that the BPD/NBL ratio decreases slightly with gesta- tional age for fetuses, the change was not statistically signifi- cant, which is similar to the previous literature. Table 2 and Table 3 show the mean, SD, 95% confidence interval of mean for the ratios of the BPD and HL to NBL with advancing gestational age. Figure 1. Mid-sagi ttal view showing detection and measurement of the nasal bone. In addition, the correlation coefficients between gestational age and ratios of the fetal long bones to NBL were calculated by Pearson correlation. Table 4 shows the correlation coeffi- cients between gestational age and the ratios of the BPD and HL to NBL. Table 1. Distribution of the ratios of biparietal diameter (BPD) to nasal bone le ngth (NBL ) and fetal long bone lengths to NBL. Mean SD 95% Confidence Interval of Mean Lower Bound Upper Bound BPD/NBL 7.240 0.8487 7.194 7.285 HL/NBL 4.807 0.5782 4.768 4.846 RL/NBL 4.157 0.5023 4.123 4.191 UL/NBL 4.502 0.5494 4.465 4.539 FL/N B L 5.131 0.6336 5.088 5.174 TL/NBL 4.528 0.5609 4.490 4.565 FiL/NBL 4.507 0.5541 4.469 4.544 SD: standard deviation, SE: standard error, humerus length (HL), radius length (RL), ulna length (UL), femur lengt h (FL) , t i bia length (TL) , f i bula length (FiL) . Table 2. Distribution of the ratio of biparietal diameter (BPD) to nasal bone length (NBL) against wee ks of gestation. Mean SD 95% Confidence Interval of Mean Lower Bound Upper Bound 19+0–19+6 7.500 0.9933 7.122 7.878 20+0–20+6 7.292 0.8878 7.153 7.430 21+0–21+6 7.212 0.8071 7.110 7.313 22+0–22+6 7.212 0.8492 7.118 7.306 23+0–23+6 7.333 0.8617 7.221 7.444 24 +0 –24 +6 7.082 0.7409 6.952 7.212 25+0–25+6 7.236 0.9428 7.019 7.453 26+0–26+6 7.263 0.9209 7.020 7.505 27+0–27+6 7.228 0.7812 7.021 7.436 28+0–28+6 7.184 0.8161 6.894 7.473 SD: s tanda rd deviation, nas al bone length (NBL), biparie tal diamet er (BPD). Table 3. Distribution of the ratio of humerus length (HL) to nasal bone length (NBL ) against weeks of gestation. Mean SD 95% Confidence Interval for Mean Lower Bound Upper Bound 19+0–19+6 4.803 0.5607 4.590 5.017 20+0–20+6 4.711 0.5729 4.622 4.801 21+0–21+6 4.688 0.5637 4.617 4.759 22+0–22+6 4.712 0.5864 4.647 4.777 23+0–23+6 4.835 0.6163 4.756 4.915 24+0–24+6 4.662 0.5418 4.567 4.757 25+0–25+6 4.718 0.6419 4.570 4.866 26+0–26+6 4.683 0.5260 4.544 4.821 27+0–27+6 4.827 0.6241 4.661 4.993 28+0–28+6 4.631 0.6116 4.415 4.848 SD: s tanda rd deviation, nasal bone length ( NBL ) , h ume r us le ng t h ( H L ).  F.-Y. YANG, Y. –L. LIN Copyright © 2012 SciRes. ENG 148 Table 4. Pearson correlation coefficients of gestational age with ratios of the BPD/NBL and HL/ NBL . GA BPD/NBL HL/NBL GA 1 -.031 .001 gestational age (GA, ) na s al bo ne leng t h (NB L ), bipar iet al diame t er (BPD) , hume rus length (H L ) The study of intraobserver variability showed mean differ- ences bet ween the two measurements ranging from −0.0591 to 0.1682 and Cronbach's Alpha value ranging from 0.997 to 0.999. 4. Discussion The present study provides the ratios of fetal limb bones to NBL with reference range from 19 to 28 weeks of gestation in normal Taiwanese fetuses. Each woman contributed one set of measurements taken during advanced prenatal ultrasound ex- amination and assessment. No significant change in the BPD/NBL ratio, HL/NBL ratio, UL/NBL ratio, and RL/NBL ratio with gestational age were demonstrated in our population (Pearson correlation coefficient < 0.05). According to previous published studies, the BPD/NBL ratio was first described in 2005. A total of 136 fetuses were eva- luated for the association between the BPD/NBL ratio and tri- somy 21 in the second-trimester [19]. In many subsequent stu- dies, assessments of the NBL/BPD ratio were done in the second trimester. In recent studies, the optimal threshold values for the BPD/NBL ratio were investigated for detection of tri- somy 21. The ultrasound measurements were done in 239 women with a singleton pregnancy at 15-20 weeks of gestation at Massa- chusetts General Hospital, USA. The receiver operating cha- racteristic curve for the BPD/NBL ratio showed that using a cutoff value of 9 or greater resulted in 100% of fetuses with Down syndrome and 22% of euploid fetuses. If the cutoff value were raised to 10 or greater, then 81% of fetuses with Down syndrome and 11% of euploid fetuses would be identified. If the cutoff value was 11 or greater, 69% of fetuses with Down syndrome would be identified, compared with 5% of euploid fetuses [17]. This was consistent with the others in the litera- ture. In this study, we calculated not only the fetal BPD/NBL ratio but also ratios of the fetal limb bones to NBL between 19 and 28 weeks. Be sides, the fetal b iometry and limb bones length in our study were compared with previously reported measure- ments from other populations [25,26]. The biometry, limb bones length, and fetal weight were all in the normal range. Moreover, the HL/NBL ratio did not change with gestational age. The Pearson product-moment correlat ion co efficient o f the HL/NBL with gestational age was lower than those of ratios with gestational age. The NB hypoplasia or absence is an important marker for Down syndrome. The combination of other makers with the NB assessment was associated with an improvement in detecting the risk of Down syndrome [27]. Thu s, th ere is a need to est ab- lish the specific evalu ated formulas by NBL with different me- thods. In this pilot study, our data have established the reference ra- tio of the fetal limb bones to NBL in normal singleton Taiwa- nese fetuses. To our knowledge, this is the first prospective study to evaluate the ratios of the fetal limb bones to NBL in the second trimester. Our data also show that the HL/NBL ratio does not change with advancing gestational age. Comparing with the lower limb, it is usually easier to visualize the upper limb. The humerus is the easiest of the upper limb bones to define with ultrasound, as it has less freedom of movement than the forearm. We determined that the HL/NBL ratio was supe- rior to that of BPD or other limb bones ratios. Additional veri- fication for detecting the risk of chromosomal aneuploidy is required before this approach can be applied in a clinical setting. This study points out a better clinical approach for evaluating fetuses with skeletal anomalies or risk of aneuploid chromo- somes in the general population. 5. Acknowledgements This study was supported by grants from the National Science Council of Taiwan (no. NSC 100-2321-B-010-010 and NSC 99-2321-B-010-017), Cheng Hsin General Hospital Foundation (no. 100F117CY25), Veterans General Hospitals University System of Taiwan Joint Research Program (#VGHUST100- G1-3 -3 and V100E6-007), Yen Tjing Ling Medical Foundation (grant CI-100-17), Department of Health of Taiwan (DOH101- TD-PB-111-TM012) REFERENCES [1] Bell, R., J. Rankin, and L.J. Donaldson, Down's syndrome: oc- curren ce and out come in th e north of Engla nd, 1985 -99. P aedi atr Perinat Epidemiol, 2003. 17(1): p. 33-9. [2] Van den Hof, M.C. and R.D. Wilson, Fetal soft markers in ob- stetric ultrasound. J Obstet Gynaecol Can, 2005. 27(6): p. 592-636. [3] Stempfle, N., et al., Skeletal abnormalities in fetuses with Down's syndrome: a radiographic post-mortem study. Pediatr Radio l, 19 9 9. 2 9( 9 ) : p. 682-8. [4] Nicolaides, K.H., Nuchal translucency and other first-trimester sonographic markers of chromosomal abnormalities. Am J Ob- stet Gyne col, 2004. 191 ( 1) : p. 45 -67. [5] Cicero, S., et al., Absence of nasal bone in fetuses with trisomy 21 at 11-14 weeks of gestation: an observational study. Lancet, 2001. 358(9294): p. 1665-7. [6] Viora, E., et al., Ultrasound evaluation of fetal nasal bone at 11 to 14 weeks i n a c ons ecu t iv e seri es of 1 90 6 fet u s es. Pr enat Di a gn, 2003. 23(10): p . 784-7. [7] Ramos-Corpas, D., J.C. Santiago, and F. Montoya, Ultrasono- graphi c evaluation of fetal nasal bon e in a low-risk population at 11-13 + 6 gestational weeks. Prenat Diagn, 2006. 26(2): p. 112-7. [8] Monni, G., et al., Nuchal translucency and nasal bone for trisomy 21 sc r een in g: sin g le cen t er experience. Cr o at Med J, 2005. 4 6(5) : p. 786-91. [9] Bunduk i, V., et al., Fetal nasal bone length: reference ran ge and clinical application in ultrasound screening for trisomy 21. Ul- trasound Obstet Gynecol, 2003. 21(2): p. 156-60. [10] Otano, L., et al., Association between first trimester absence of fetal nasal bone on ultrasound and Down syndrome. Prenat Di- agn, 2 002. 22(10) : p. 93 0-2.  F.-Y. YANG, Y. –L. LIN Copyright © 2012 SciRes. ENG 149 [11] Cicero, S., et al., Integrated ultrasound and biochemical screen- ing for trisomy 21 using fetal nuchal translucency, absent fetal nasal b on e, f ree b et a-h C G a n d P AP P -A at 11 to 14 weeks. Prenat Diagn, 2003. 23(4): p. 306 -10. [12] Cusick, W., et al., Fetal nasal bone length in euploid and aneup- loid fetuses between 11 and 20 weeks' gestation: a prospective stud y. J Ultrasound Med, 2004. 23(10): p. 1327-33. [13] Viora, E., et al., Fetal nasal bone and trisomy 21 in the second trimester. Prenat Diagn, 2005. 25(6): p. 511-5. [14] Vi ntzil eos, A., C. Walt ers, and L. Yeo, Abs ent nasa l bone in th e prenatal detection of fetuses with trisomy 21 in a high-risk pop- ulat ion. O bste t Gyneco l , 2003 . 1 0 1( 5 Pt 1): p. 9 05-8. [15] Odibo, A.O., et al., The association between fetal nasal bone hypoplasia and aneuploidy. Obstet Gynecol, 2004. 104(6): p. 1229-33. [16] Kanagawa, T., et al., Mid-secon d trimester m easuremen t of fet al nasal bone length in the Japanese population. J Obstet Gynaecol Res, 2006. 32(4) : p. 403-7. [17] Bromley, B., et al., Fetal nose bone length: a marker for Down syndrome in the second trimester. J Ultrasound Med, 2002. 21(12 ) : p. 1 387-94. [18] Naraphut, B., et al., Nasal bone hypoplas ia i n tri som y 21 a t 1 5 to 24 weeks' gestation in A high risk Thai population. J Med Assoc Thai, 2006. 89(7): p. 911-7. [19] Tran, L.T., et al., Second-trimester biparietal diameter/nasal bone length ratio is an independent predictor of trisomy 21. J Ultra- sound Med, 2005. 24(6): p. 805-10. [20] Shohat, T. and O. Romano-Zelekha, Ultrasonographic measure- ments of fetal femur length and biparietal diameter in an Israeli popula tion. Isr Med Assoc J, 2001. 3(3) : p. 166-8. [21] Cicero, S., et al., Fetal nasal bone length in ch romosomally nor- mal and abnormal fetuses at 11-14 weeks of gestation. J Matern Fet al Neonatal Me d , 20 02. 1 1( 6) : p. 4 00-2. [22] Sonek, J.D. and K.H. Nicolaides, Prenatal ultrasonographic diagnosis of nasal bone abnormalities in three fetuses with Down syndrome. Am J Obstet Gynecol, 2002. 186(1): p. 139-41. [23] Goldstein, R.B., R.A. Filly, and G. Simpson, Pitfalls in femur length measurements. J Ultrasound Med, 1987. 6(4): p. 203-7. [24] De Biasio, P., et al., Reference values for fetal limb biometry at 10-14 weeks of gestation. Ultrasound Obstet Gynecol, 2002. 19(6): p. 588-91. [25] M erz, E. and S. Wellek , [N ormal fet al growth profi le--a uni form model for calculating normal curves for current head and abdo- men parameters and long limb bones]. Ultraschall Med, 1996. 17(4): p. 153-62. [26] Salomon, L.J., J.P. Bernard, and Y. Ville, Estimation of fetal weight: reference range at 20-36 weeks' gestation and compari- son with actual birth-weight reference range. Ultrasound Obstet Gyne col, 2007 . 29(5) : p. 55 0-5. [27] Odibo, A.O., et al., Evaluating the efficiency of using second-trimester nasal bone hypoplasia as a single or a combined marker for fetal aneuploidy. J Ultrasound Med, 2006. 25(4): p. 437-41; quiz 443. |