Laparoscopic Gastrectomy after the Age of Eighty: Still a Good Choice?
Copyright © 2013 SciRes. JCT
30
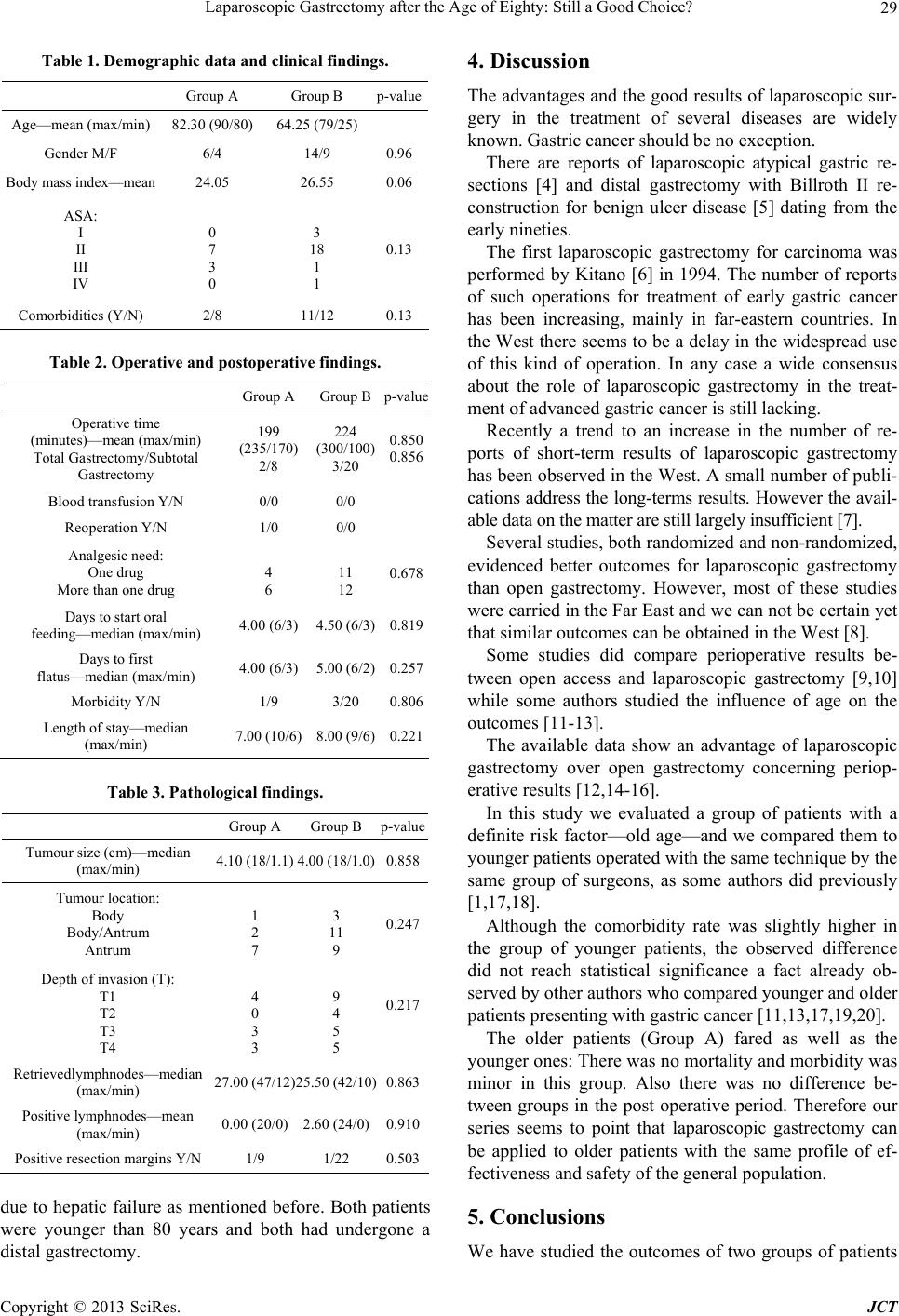
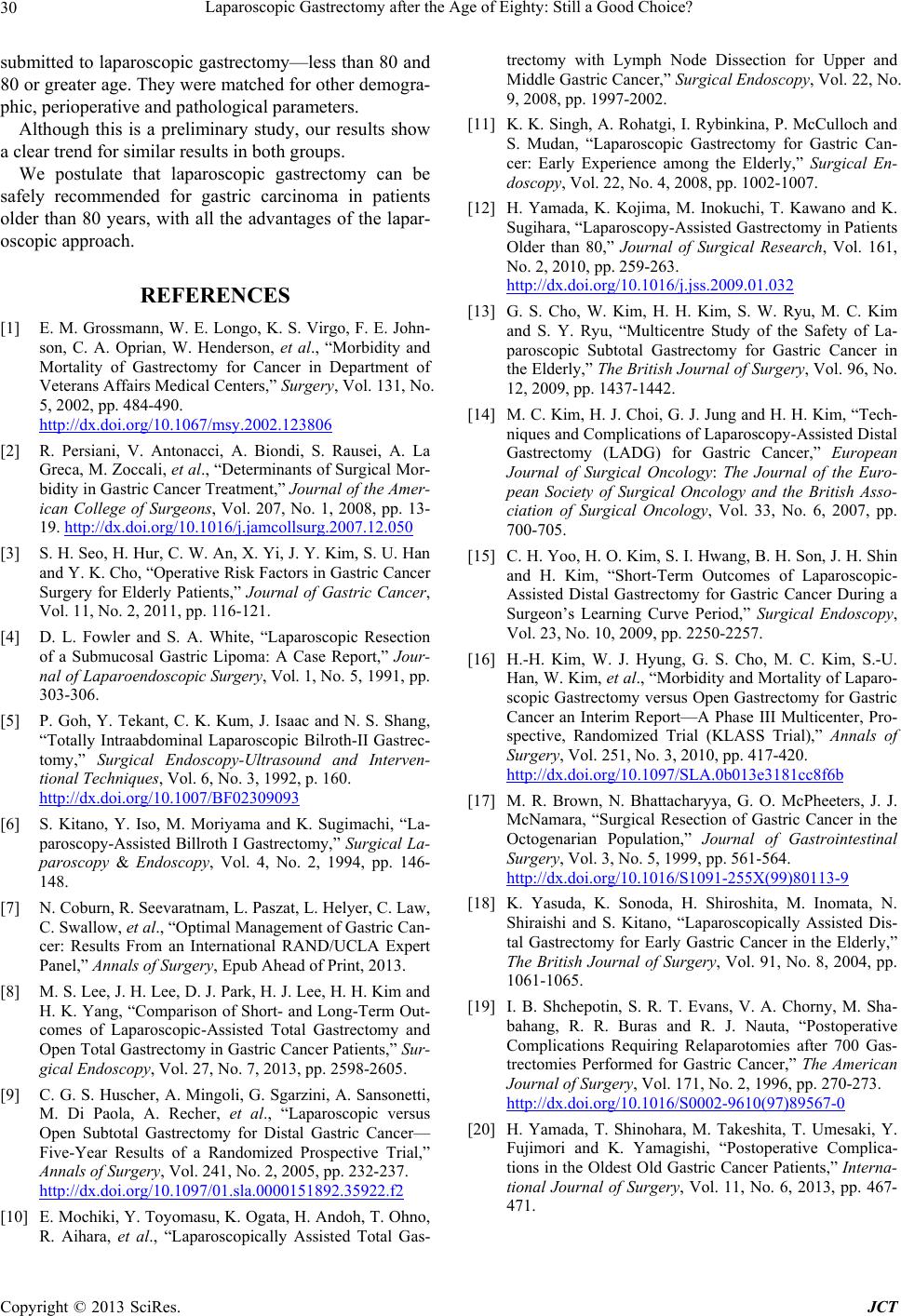
submitted to laparosco pic gastrectomy—less than 80 and
80 or greater age. They were matched for other demogra-
phic, perioperative and pathological parameters.
Although this is a preliminary study, our results show
a clear trend for similar results in both groups.
We postulate that laparoscopic gastrectomy can be
safely recommended for gastric carcinoma in patients
older than 80 years, with all the advantages of the lapar-
oscopic approach.
REFERENCES
[1] E. M. Grossmann, W. E. Longo, K. S. Virgo, F. E. John-
son, C. A. Oprian, W. Henderson, et al., “Morbidity and
Mortality of Gastrectomy for Cancer in Department of
Veterans Affairs Medical Centers,” Surgery, Vol. 131, No.
5, 2002, pp. 484-490.
http://dx.doi.org/10.1067/msy.2002.123806
[2] R. Persiani, V. Antonacci, A. Biondi, S. Rausei, A. La
Greca, M. Zoccali, et al., “Determinants of Surgical Mor-
bidity in Gastric Cancer Treatment,” Journal of the Amer-
ican College of Surgeons, Vol. 207, No. 1, 2008, pp. 13-
19. http://dx.doi.org/10.1016/j.jamcollsurg.2007.12.050
[3] S. H. Seo, H. Hur, C. W. An, X. Yi, J. Y. Kim, S. U. Han
and Y. K. Cho, “Operative Risk Factors in Gastric Cancer
Surgery for Elderly Patients,” Journal of Gastric Cancer,
Vol. 11, No. 2, 2011, pp. 116-121.
[4] D. L. Fowler and S. A. White, “Laparoscopic Resection
of a Submucosal Gastric Lipoma: A Case Report,” Jour-
nal of Laparoendoscopic Surgery, Vol. 1, No. 5, 1991, pp.
303-306.
[5] P. Goh, Y. Tekant, C. K. Kum, J. Isaac and N. S. Shang,
“Totally Intraabdominal Laparoscopic Bilroth-II Gastrec-
tomy,” Surgical Endoscopy-Ultrasound and Interven-
tional Techniques, Vol. 6, No. 3, 1992, p. 160.
http://dx.doi.org/10.1007/BF02309093
[6] S. Kitano, Y. Iso, M. Moriyama and K. Sugimachi, “La-
paroscopy-Assist ed Billroth I Gastrectomy,” Surgical La-
paroscopy & Endoscopy, Vol. 4, No. 2, 1994, pp. 146-
148.
[7] N. Coburn, R. Seevaratnam, L. Paszat, L. Helyer, C. Law,
C. Swallow, et al., “Optimal Management of Gastric Can-
cer: Results From an International RAND/UCLA Expert
Panel,” Annals of Surgery, Epub Ahead of Print, 2013.
[8] M. S. Lee, J. H. Lee, D. J. Park, H. J. Lee, H. H. Kim and
H. K. Yang, “Comparison of Short- and Long-Term Out-
comes of Laparoscopic-Assisted Total Gastrectomy and
Open Total Gastrectomy in Gastric Cancer Patients,” Sur-
gical Endoscopy, Vol. 27, No. 7, 2013, pp. 2598-2605.
[9] C. G. S. Huscher, A. Mingoli, G. Sgarzini, A. Sansonetti,
M. Di Paola, A. Recher, et al., “Laparoscopic versus
Open Subtotal Gastrectomy for Distal Gastric Cancer—
Five-Year Results of a Randomized Prospective Trial,”
Annals of Surgery, Vol. 241, No. 2, 2005, pp. 232-237.
http://dx.doi.org/10.1097/01.sla.0000151892.35922.f2
[10] E. Mochiki, Y. Toyomasu, K. Ogata, H. Andoh, T. Ohno,
R. Aihara, et al., “Laparoscopically Assisted Total Gas-
trectomy with Lymph Node Dissection for Upper and
Middle Gastric Cancer,” Surgical Endoscopy, Vol. 22, No.
9, 2008, pp. 1997-2002.
[11] K. K. Singh, A. Rohatgi, I. Rybinkina, P. McCulloch and
S. Mudan, “Laparoscopic Gastrectomy for Gastric Can-
cer: Early Experience among the Elderly,” Surgical En-
doscopy, Vol. 22, No. 4, 2008, pp. 1002-1007.
[12] H. Yamada, K. Kojima, M. Inokuchi, T. Kawano and K.
Sugihara, “Laparoscopy-Assisted Gastre ctomy in Patients
Older than 80,” Journal of Surgical Research, Vol. 161,
No. 2, 2010, pp. 259-263.
http://dx.doi.org/10.1016/j.jss.2009.01.032
[13] G. S. Cho, W. Kim, H. H. Kim, S. W. Ryu, M. C. Kim
and S. Y. Ryu, “Multicentre Study of the Safety of La-
paroscopic Subtotal Gastrectomy for Gastric Cancer in
the Elde rly,” The British Journal of Surgery, Vol. 96, No.
12, 2009, pp. 1437-1442.
[14] M. C. Kim, H. J. Choi, G. J. Jung and H. H. Kim, “Tech-
niques and Complications of Laparoscopy-Assiste d Distal
Gastrectomy (LADG) for Gastric Cancer,” European
Journal of Surgical Oncology: The Journal of the Euro-
pean Society of Surgical Oncology and the British Asso-
ciation of Surgical Oncology, Vol. 33, No. 6, 2007, pp.
700-705.
[15] C. H. Yoo, H. O. Kim, S. I. Hwang, B. H. Son, J. H. Shin
and H. Kim, “Short-Term Outcomes of Laparoscopic-
Assisted Distal Gastrectomy for Gastric Cancer During a
Surgeon’s Learning Curve Period,” Surgical Endoscopy,
Vol. 23, No. 10, 2009, pp. 2250-2257.
[16] H.-H. Kim, W. J. Hyung, G. S. Cho, M. C. Kim, S.-U.
Han, W. Kim, et al., “Morbidity and Mortality of Laparo-
scopic Gastrectomy versus Open Gastrectomy for Gastric
Cancer an Interim Report—A Phase III Multicenter, Pro-
spective, Randomized Trial (KLASS Trial),” Annals of
Surgery, Vol. 251, No. 3, 2010, pp. 417-420.
http://dx.doi.org/10.1097/SLA.0b013e3181cc8f6b
[17] M. R. Brown, N. Bhattacharyya, G. O. McPheeters, J. J.
McNamara, “Surgical Resection of Gastric Cancer in the
Octogenarian Population,” Journal of Gastrointestinal
Surgery, Vol. 3, No. 5, 1999, pp. 561-564.
http://dx.doi.org/10.1016/S1091-255X(99)80113-9
[18] K. Yasuda, K. Sonoda, H. Shiroshita, M. Inomata, N.
Shiraishi and S. Kitano, “Laparoscopically Assisted Dis-
tal Gastrectomy for Early Gastric Cancer in the Elderly,”
The British Journal of Surgery, Vol. 91, No. 8, 2004, pp.
1061-1065.
[19] I. B. Shchepotin, S. R. T. Evans, V. A. Chorny, M. Sha-
bahang, R. R. Buras and R. J. Nauta, “Postoperative
Complications Requiring Relaparotomies after 700 Gas-
trectomies Performed for Gastric Cancer,” The American
Journal of Surgery, Vol. 171, No. 2, 1996, pp. 270-273.
http://dx.doi.org/10.1016/S0002-9610(97)89567-0
[20] H. Yamada, T. Shinohara, M. Takeshita, T. Umesaki, Y.
Fujimori and K. Yamagishi, “Postoperative Complica-
tions in the Oldest Old Gastric Cancer Patients,” Interna-
tional Journal of Surgery, Vol. 11, No. 6, 2013, pp. 467-
471.