E. PETKOVA ET AL. 11
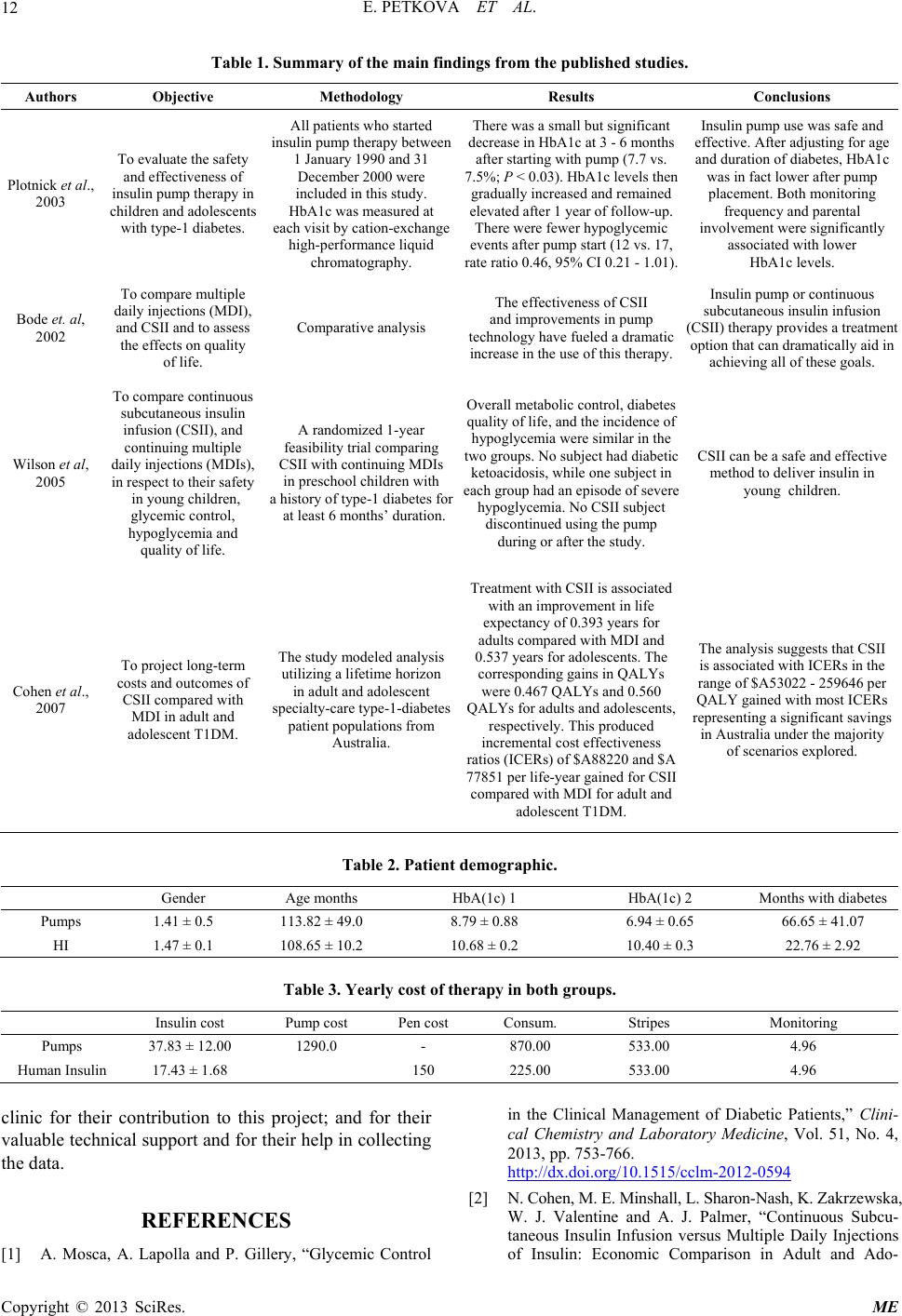
cacy, safety and/or cost-effectiveness of CSII usage in
the pediatric population—Table 1. The number of ob-
served patients varied from 19 to 95. All of these studies
measured the decrease in HbA1C, and some, in addition ,
focused on patients’ demographic characteristics, glucose
level, hypoglycemia, and quality of life. All of the stud-
ies conclude that CSII is safe and effective, leading to
greater decreases in HbA1c levels, allowing for im-
proved quality of life, decreased hypoglycemic events
and improved child and parent adherence as shown in
Table 1.
The published studies define the HbA1c level as the
widely accepted measure of diabetes control in pediatric
practice. Positive therapeutic results after CSII introduc-
tion that might lead to better long-term outcomes are ob-
served.
3.2. Results of the Study
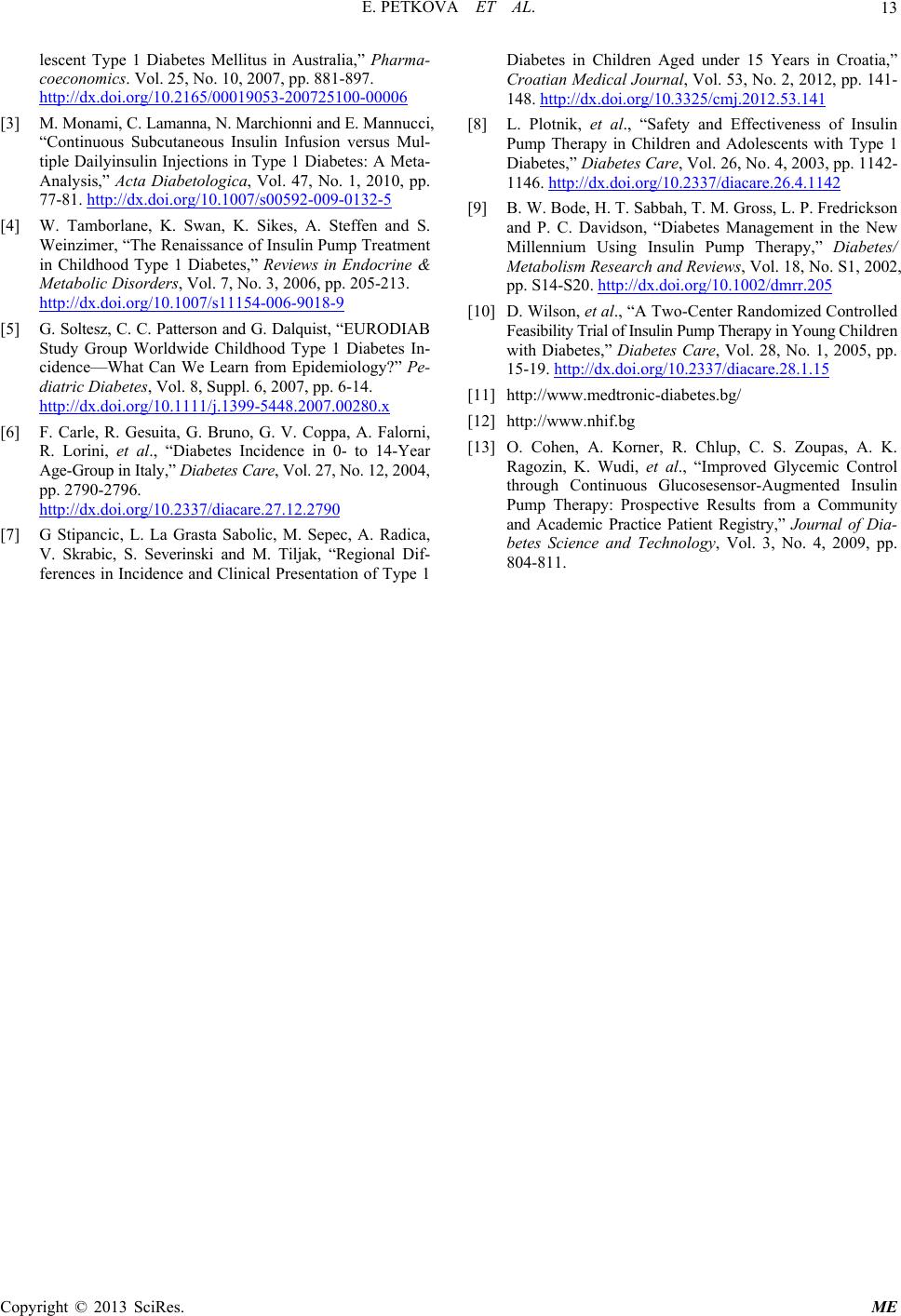
The University pediatric clinic has been introducing CSII
on the request of the parents, with only 30 children hav-
ing applied so far. From 1999 to 2011, 17 children with
diabetes type-1 were observed (mean age 113.82 months
in the active group and 112.41 in the control group). The
duration of diabetes was a little lower in the control
group—Table 2. The average improvement of HbA (1c)
in the active group after the CSII introduction is 1.85,
while after the application of human insulin—0.28 (Table
2).
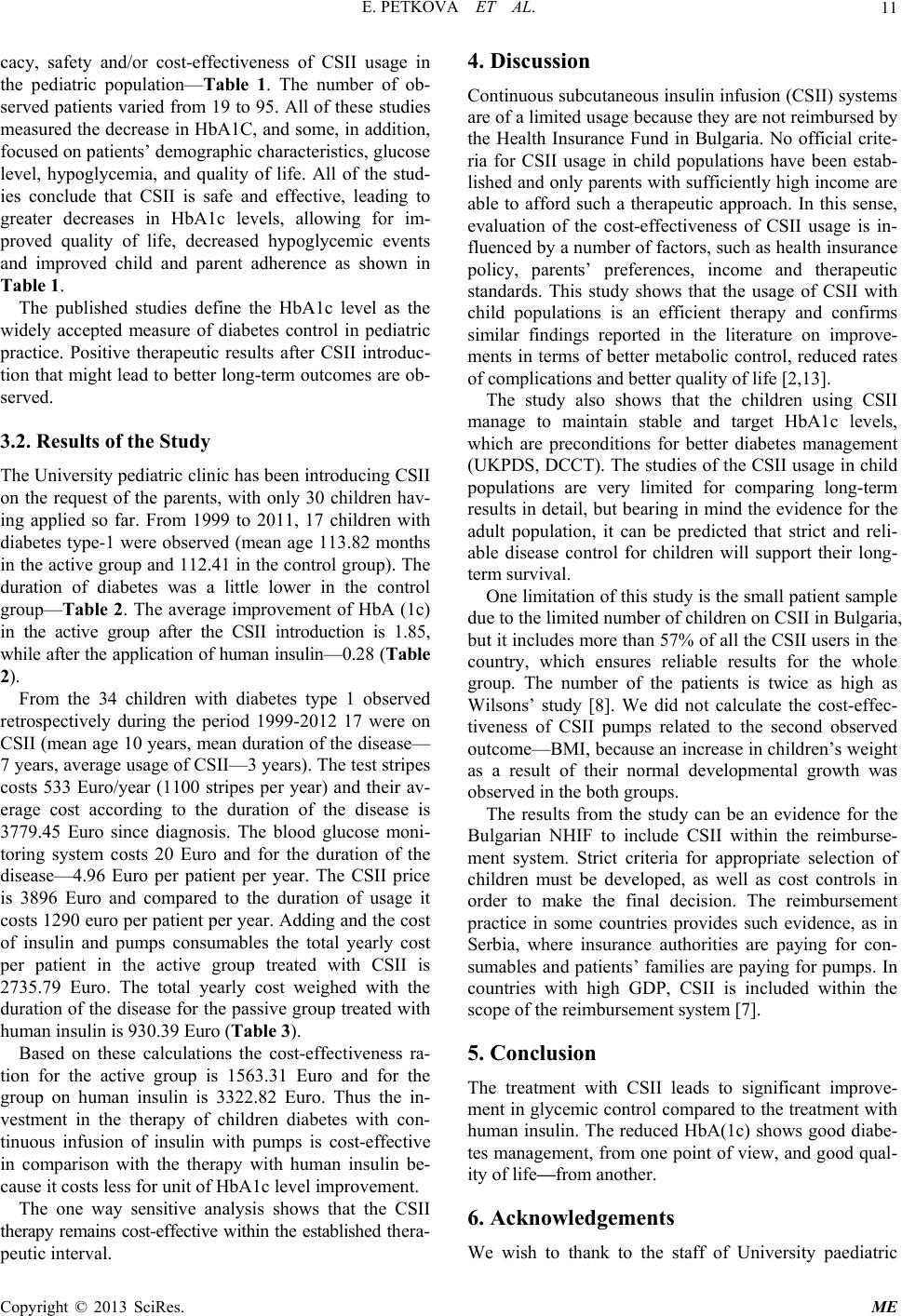
From the 34 children with diabetes type 1 observed
retrospectively during the period 1999-2012 17 were on
CSII (mean age 10 years, mean duration of the disease—
7 years, average usage of CSII—3 years). The test stripes
costs 533 Euro/year (1100 stripes per year) and their av-
erage cost according to the duration of the disease is
3779.45 Euro since diagnosis. The blood glucose moni-
toring system costs 20 Euro and for the duration of the
disease—4.96 Euro per patient per year. The CSII price
is 3896 Euro and compared to the duration of usage it
costs 1290 euro pe r patient per year. Adding and the cost
of insulin and pumps consumables the total yearly cost
per patient in the active group treated with CSII is
2735.79 Euro. The total yearly cost weighed with the
duration of the disease for the passive group treated with
human insulin is 930.39 Euro (Table 3).
Based on these calculations the cost-effectiveness ra-
tion for the active group is 1563.31 Euro and for the
group on human insulin is 3322.82 Euro. Thus the in-
vestment in the therapy of children diabetes with con-
tinuous infusion of insulin with pumps is cost-effective
in comparison with the therapy with human insulin be-
cause it costs less for unit of HbA1c level improvement.
The one way sensitive analysis shows that the CSII
therapy remains cost-effective within the established thera-
peutic interval.
4. Discussion
Continuous subcutaneous insulin infusion (CSII) systems
are of a limited usage because they are not reimbursed by
the Health Insurance Fund in Bulgaria. No official crite-
ria for CSII usage in child populations have been estab-
lished and only parents with sufficiently high income are
able to afford such a therapeutic approach. In this sense,
evaluation of the cost-effectiveness of CSII usage is in-
fluenced by a number of factors, such as health insurance
policy, parents’ preferences, income and therapeutic
standards. This study shows that the usage of CSII with
child populations is an efficient therapy and confirms
similar findings reported in the literature on improve-
ments in terms of better metabolic control, reduced rates
of complications and better quality of life [2,13].
The study also shows that the children using CSII
manage to maintain stable and target HbA1c levels,
which are preconditions for better diabetes management
(UKPDS, DCCT). The studies of the CSII usage in child
populations are very limited for comparing long-term
results in detail, but bearing in mind the evidence for the
adult population, it can be predicted that strict and reli-
able disease control for children will support their long-
term survival.
One limitation of this study is the small pati ent sample
due to the limited number of child ren on CSII in Bulg aria,
but it includes more than 57% of all the CSII users in the
country, which ensures reliable results for the whole
group. The number of the patients is twice as high as
Wilsons’ study [8]. We did not calculate the cost-effec-
tiveness of CSII pumps related to the second observed
outco me—BM I, bec ause an incre ase in child ren’s weight
as a result of their normal developmental growth was
observed in the both groups.
The results from the study can be an evidence for the
Bulgarian NHIF to include CSII within the reimburse-
ment system. Strict criteria for appropriate selection of
children must be developed, as well as cost controls in
order to make the final decision. The reimbursement
practice in some countries provides such evidence, as in
Serbia, where insurance authorities are paying for con-
sumables and patients’ families are paying for pumps. In
countries with high GDP, CSII is included within the
scope of the reimbursement system [7].
5. Conclusion
The treatment with CSII leads to significant improve-
ment in glycemic control compared to the treatment with
human insulin. The reduced HbA(1c) shows good diabe-
tes management, fr om one point of view, and good qual-
ity of life—from another.
6. Acknowledgements
We wish to thank to the staff of University paediatric
Copyright © 2013 SciRes. ME