B. Mengistie et al. / Open Journal of Preventive Medicine 3 (2013) 446-453
452
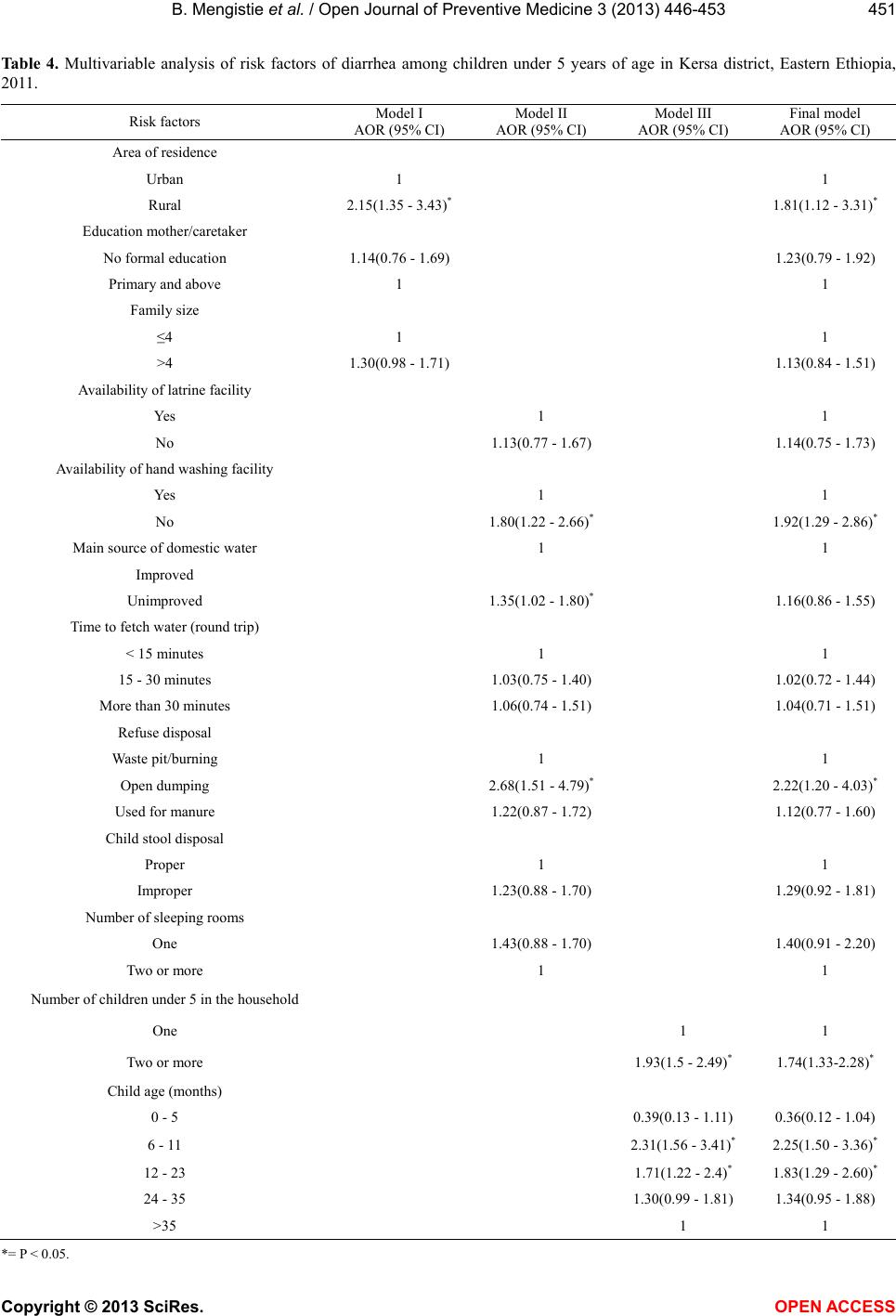
The importance of refuse in transmitting diarrhea
pathogens has been documented [21]. In our study, open
disposal of refuse around the house was an independent
risk factor for diarrhea. This is in agreement with other
studies conducted elsewhere [22,23]. The simple expla-
nation might be that inappropriate disposal of refuse pro-
vides breeding site for insects, which may carry diarrhea
pathogens from the refuse to water and food.
Studies showed the importance of hand washing in
reducing the occurrence of childhood diarrhea [24,25].
However, monitoring correct hand washing behavior at
critical times is challenging. Hygiene behavior related
observational studies showed wide discrepancy between
what people said and did and suggested that reported
hand washing behavior over estimate observed behavior
[26-28] and supported the availability of water and soap
in places of hand washing as indicator of hand washing
behavior [29]. In this study, there was a significant posi-
tive association between the availability of hand washing
facility with childhood diarrhea.
The study showed that diarrhea was significantly as-
sociated with children in the age groups 6 - 11 months
and 12 - 23 months compared to children aged above 35
months. This finding is in agreement with other studies
[5,9]. The peak prevalence of diarrhea at the age of 6 - 11
months can be explained by the introduction of contami-
nated weaning foods [30]. In addition, crawling starts at
this age and the risk of ingesting contaminated materials
may cause diarrhea. The risk of diarrhea decreases sub-
sequently after 6 - 11 months; this is probably because
the children begin to develop immunity to pathogens
after repeated exposure [31].
The odds of diarrhea were higher among rural children
than urban ones and this was consistent with the findings
in Uganda [11] and Egypt [19]. This could be attributed
to the fact that the lack of access to water and sanitation
facilities in the rural areas was more than in the urban
areas [32].
In this study, diarrhea was significantly associated
with the presence of two or more under five children in
the family. This is in agreement with a study done in
Pakistan [33]. Other study also indicated that number of
children born was a predictor of diarrhea among under
five children [34]. This might be due to the incapability
of the caregiver to care for a large number of children
[19]. It is possible to suggest that child birth spacing might
have a positive influence on prevention of diarrhea.
In conclusion, childhood diarrhea remains an impor-
tant health concern in the study community. Occurrence
of diarrhea could be decreased by interventions aimed to
improve sanitation, hygiene and child birth spacing.
5. ACKNOWLEDGEMENTS
The authors would like to thank Haramaya University for its finan-
cial support. We are also thankful for study participants, data collectors
and supervisors for their devotion and full participation.
REFERENCES
[1] Black, R.E., Morris, S.S. and Bryce. J. (2003) Where and
why are 10 million children dying every year? Lancet,
361, 2226-2234.
http://dx.doi.org/10.1016/S0140-6736(03)13779-8
[2] Fisher Walker, L.C., Perin, J., Aryee, J.M., Boschi-Pinto,
C. and Black, R.E. (2012) Diarrhea incidence in low- and
middle-income countries in 1990 and 2010: A systematic
review. BMC Public Health, 12.
http://dx.doi.org/10.1186/1471-2458-12-220
[3] UNICEF/WHO (2009) Diarrhoea: Why children are still
dying and what can be done. The United Nations Chil-
dren’s Fund/World Health Organization, Geneva.
[4] WHO (2007) Combating waterborne disease at the house-
hold level. International Network to Promote Household
Water Treatment and Safe Storage, World Health Organi-
zation, Geneva.
[5] Desalegn, M., Kumie, A. and Tefera, W. (2011) Predictors
of under-five childhood diarrhea: Mecha District, West
Gojjam, Ethiopia. Ethiopian Journal of Health Develop-
ment, 25, 174-232.
[6] Teklemariam, S., Getaneh, T. and Bekele, F. (2000) En-
vironmental determinants of diarrheal morbidity in under-
five children, Keffa-Sheka zone, south west Ethiopia.
Ethiopian Medical Journal, 38, 27-34.
[7] Mediratta, P.R., Feleke, A., Moulton, H.L., Yifru, S. and
Sack, B.R. (2010) Risk factors and case management of
acute diarrhoea in North Gondar zone, Ethiopia. Journal
of Health, Population and Nutrition, 28, 253-263.
[8] Mekasha, A. and Tesfahun, A. (2003) Determinants of
diarrhoeal diseases: A community based study in urban
south western Ethiopia. East African Medical Journal, 80,
77-82.
[9] Boadi, K.O. and Kuitunen, M. (2005) Childhood diar-
rheal morbidity in the Accra Metropolitan Area, Ghana:
Socio-economic, environmental and behavioral risk de-
terminants. Journal of Health & Population in Develop-
ing Countries. http://www.jhpdc.unc.edu/
[10] Siziya, S., Muula, A.S. and Rudatsikira, E. (2009) Diar-
rhoea and acute respiratory infections prevalence and risk
factors among under-five children in Iraq in 2000. Italian
Journal of Pediatrics, 35.
http://dx.doi.org/10.1186/1824-7288-35-8
[11] Bbaale, E. (2011) Determinants of diarrhoea and acute re-
spiratory infection among under-fives in Uganda. Aus-
tralasian Medical Journal, 4, 400-409.
http://dx.doi.org/10.4066/AMJ.2011.723
[12] Chopra, M., Mason, E., Borrazzo, J., Campbell, H., Ru-
dan, I., Liu, L., Black, R.E. and Bhutta, Z.A. (2013) End-
ing of preventable deaths from pneumonia and diarrhoea:
An achievable goal. The Lancet, 381, 1499-1506.
http://dx.doi.org/10.1016/S0140-6736(13)60319-0
[13] Kersa, D.H.O. (2011) Health service coverage. Kersa
Copyright © 2013 SciRes. OPEN A CCESS