Open Journal of Stomatology, 2013, 3, 344-346 OJST
http://dx.doi.org/10.4236/ojst.2013.37058 Published Online October 2013 (http://www.scirp.org/journal/ojst/)
One stage reconstruction of large lower lip carcinoma,
with local flaps
Mergime Prekazi Loxha1, Fellanza Gjinolli1, Osman Sejfija1, Aida Rexhepi2, Zana Agani3
1Department o f Maxillofacial Surgery, Uni v ersity Clinical Center of Kosova, Prishtina, Kosova
2University Clinical Dentistry Center of Kosova, Prishtina, Kosova
3Department o f Oral Surgery, University Clinical Dentistry Center of Kosova, Prishtina, Kosova
Email: mergimeloxha@gmail.com
Received 29 July 2013; revised 29 August 2013; accepted 15 September 2013
Copyright © 2013 Mergime Prekazi Loxha-maxillofacial et al. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
ABSTRACT
Squamous cell carcinoma (SCC) of the lower lip is a
frequently diagnosed malignant pathology in the
maxillofacial region. It is a slow-growing cancer, and
can be diagnosed and treated easily and effectively;
however, early treatment is important because its
mortality rate is 10% - 30%. Reconstruction for a
large lower lip defect is surgically challenging, espe-
cially reconstruction with local flaps. Here, we pre-
sent a 52-year-old male with a large T3 SCC, which
started 13 years before this treatment and involved
nearly all of his lower lip, oral commissure and upper
lip. It was reconstructed by local flaps with good aes-
thetic and functional results. The lip was recon-
structed with a combination of a Karapandzic flap on
one side and a contralateral Webster cheek advance-
ment, using a functional neck dissection on the tumor
side and supraomohyoid neck dissection contralater-
ally. Histopathology results of the neck were negative
for metastasis. We were satisfied with the aesthetic
and functional results of the neck.
Keywords: Lower Lip Reconstruction; Local Flap ; Lip
Cancer; Metastasis
1. INTRODUCTION
Squamous cell carcinoma (SCC) of the lower lip is one
of the most frequently diagnosed malignant pathologies
in the maxillofacial region. After skin cancer, lip cancer
is the second most frequent cancer in the maxillofacial
region [1,2]. Those with T1 and T2 lesions have better
prognoses [3]. As lower lip SCC is slow-growing, it can
be diagnosed and treated easily and effectively; however,
its early treatment is important because its mortality rate
is 10% - 30%.
The recommended protocol regarding clinically nega-
tive necks of patients with lower T1/T2 carcinomas is
“wait and see” [4]. However, the treatment protocol for
patients with T3/T4 carcinomas is tumor excision with
neck dissection, as metastases are more likely. Precise
diagnosis of malignant pathologies in the maxillofacial
region, and evaluation of possible metastasis in suscepti-
ble lymph nodes of the neck are critical in choosing the
best treatment for those patients and predicting their
prognoses [5-7]. Reconstruction of a large lower lip de-
fect is surgically challenging, particularly in maintaining
oral competence and preventing sialorrhea [8,9]. Few
cases of SCC that involved both lips and oral commis-
sure reconstructed with local flaps have been reported.
2. CASE PRESENTATION
A 52-year-old man came to our department with a large
tumor that involved almost all of his lower lip, right oral
commissure and part of his right upper lip. He reported
the tumor to have started 13 years previously as a small
lesion on his right lower lip, which had slowly enlarged.
He reported no symptoms such as pain, or hemorrhage.
He had not visited a physician, but had used an ointment
made by an “alternative doctor” for a short period of
time 4 years before. As the mass began to grow more
quickly six months previously, he decided to visit our
department.
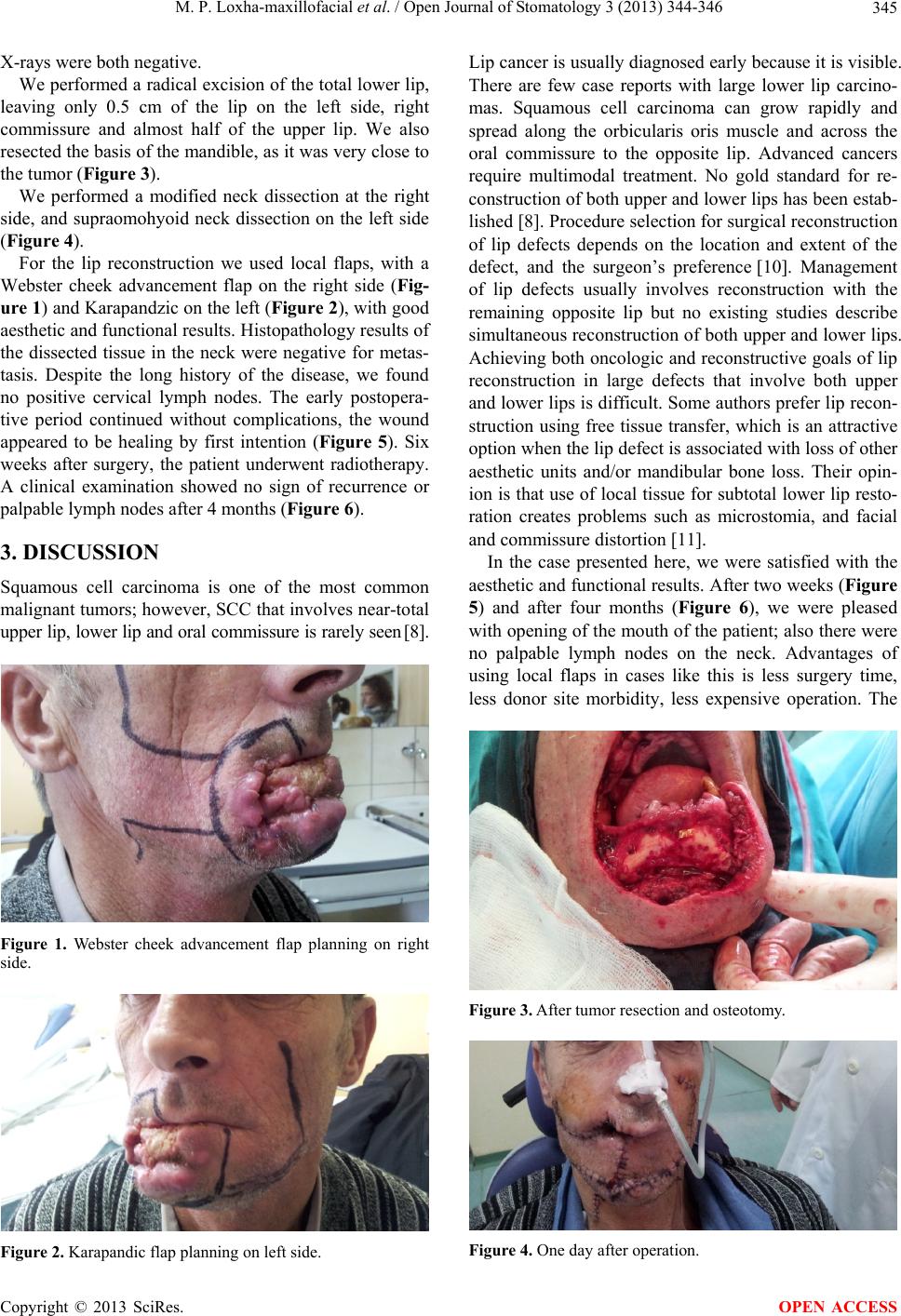
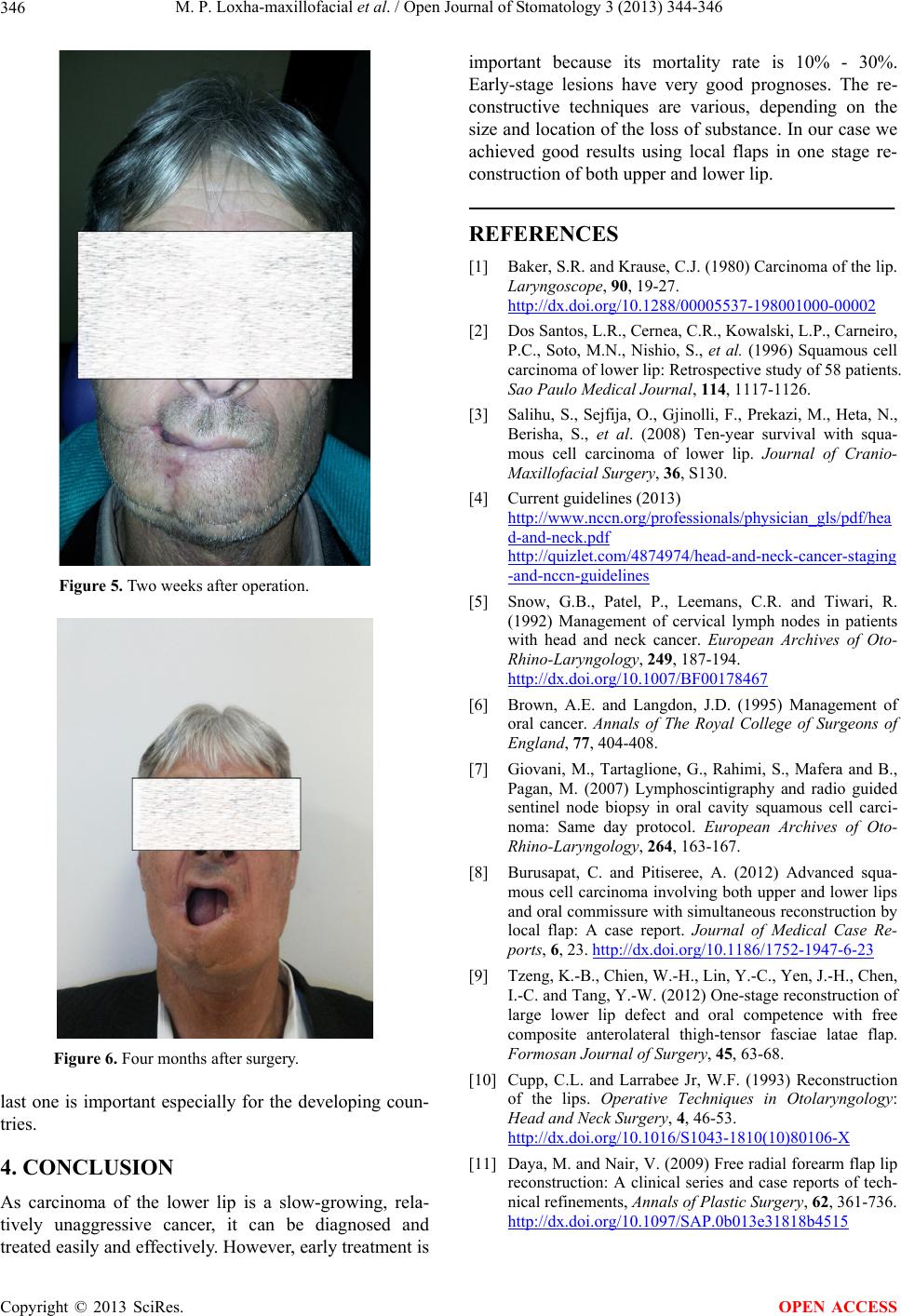
At admittance, physical examination showed a large
T3 lip mass that involved nearly all of his lower lip, right
oral commissure and part of his right upper lip (Figure 1
and 2). Regional lymph nodes were not palpable.
Results of an incisional biopsy showed SCC, Grade I.
A neck ultrasound showed a positive lymph node (17
mm × 7.5 mm) in the right submandibular region. We
did not biopsy the lymph nodes seen in ultrasound.
Panoramix results for bone involvement and native lung
OPEN ACCESS