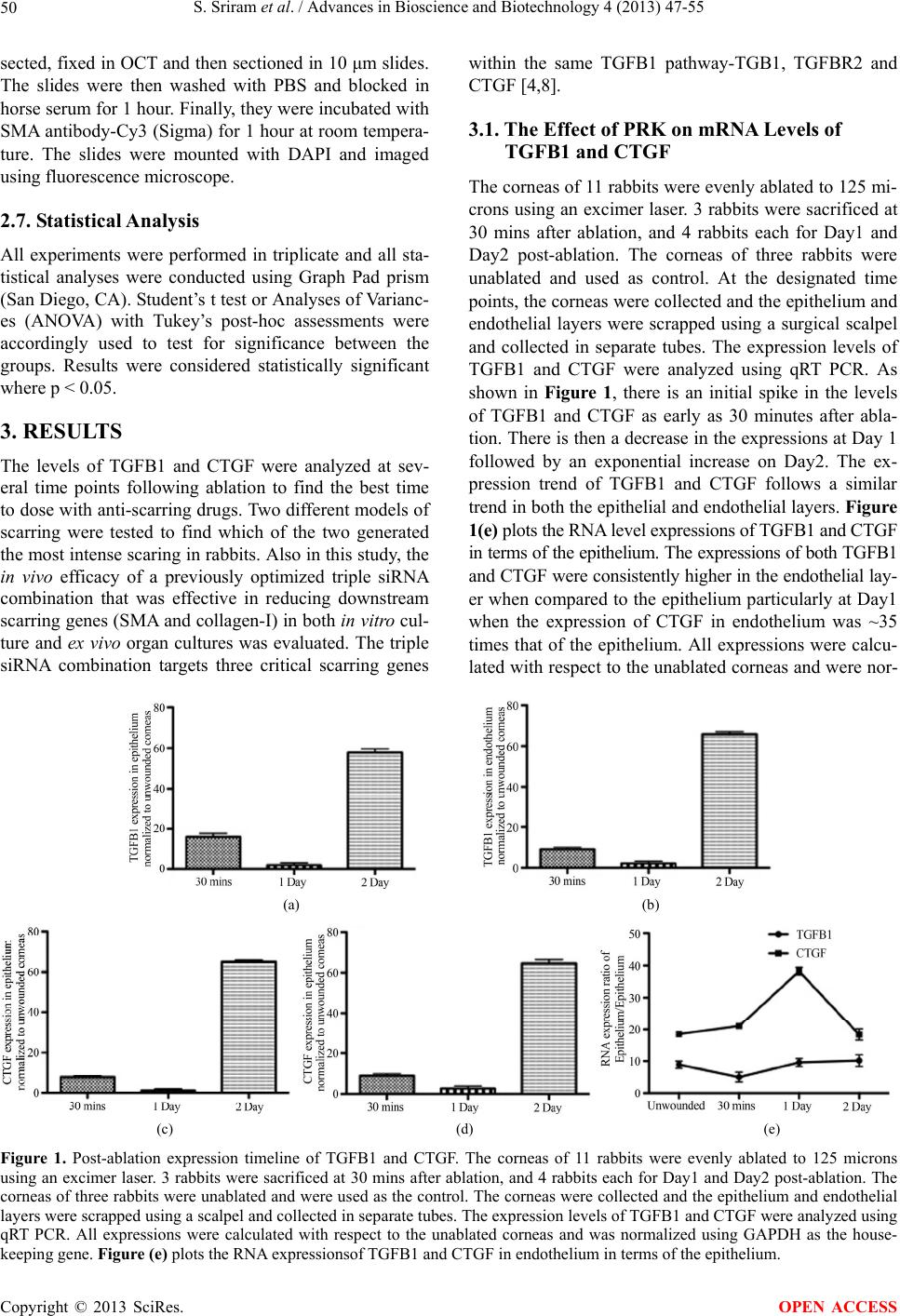
S. Sriram et al. / Advances in Bioscience and Biotechnology 4 (2013) 47-55
48
sion. The TGF-β system, has emerged as a key compo-
nent of the fibrogenic response to wounding by regulat-
ing the transformation of quiescent corneal keratocytes
into activated fibroblasts that synthesize ECM and into
myofibroblasts that contract corneal matrix (Chen et al.
2000; Jester, Petroll, and Cavanagh 1999). These myofi-
broblasts are filled with alpha smooth muscle actin (SMA)
that forms microfilaments that are the major source of
light scattering in corneal scars [1]. CTGF acting as a
downstream mediator of TGFB1, down regulates synthe-
sis of corneal crystallin proteins in quiescent keratocytes
and up regulates synthesis of collagen. Thus, the exces-
sive scattering of light that is clinically described as cor-
neal scar and haze results from the combination of colla-
gen laid down in irregular pattern in the wound and opa-
que activated fibroblasts and myofibroblasts that no lon-
ger synthesize the corneal crystallin proteins that keep
their cytoplasm transparent.
We have previously shown the effect of PRK on CTGF
levels in rat and mouse corneas and found that CTGF
was present in all cell layers of the cornea. The levels of
CTGF were found to continually rise from the time of
wounding up through 28 days post wounding [1]. How-
ever, in order to completely understand the role of TGFB1
in tissues repair and scarring, it is essential to understand
the timing and site of the synthesis of these growth fac-
tors so that the appropriate cell layer is targeted for nu-
cleic acid therapies. The experiments in this study are ex-
pected to reveal when and where TGFB1 and CTGF are
synthesized after a corneal injury so that the best mode
of action for an anti-fibrotic therapy can be chosen.
There currently are no FDA approved drugs that selec-
tively reduce the expression of genes causing corneal
scarring and haze. At present, the methods used to de-
crease corneal haze are topically applied steroids or anti-
metabolite drugs that target the cells capacity to respond
to signaling. Mitomycin C is used during some ocular sur-
geries, but it may have very damaging side effects, such
as epithelial defects, stromal melting, endothelial damage,
and conjunctival thinning [2]. Hence, there is a need to
develop a targeted approach that can nullify the specific
molecular pathways that give rise to a scar.
It is however difficult to achieve significant therapeu-
tic effect by employing a one-target, one-drug paradigm
on such a complex, multi-factorial signaling pathway.
Hence, using a multi-target approach can interrupt or act
on the complex signaling network at multiple points, and
affect the cell in ways that an individual component can-
not [3]. In this study, we have tested a siRNA triple com-
bination targeting TGFB1, TGFBR2 and CTGF. This tri-
ple siRNA combination was shown to be effective in re-
ducing the expression of target (TGFB1, TGFBR2 and
CTGF) and downstream mediators like Collagen-I and
α-Smooth Muscle Actin (SMA) in both in vitro cell cul-
ture system and ex vivo organ cultures [4].
Additionally, it is important to deliver these siRNA
combinations to the corneal layer where there is high lo-
calization of the target growth factors after wounding. Al-
though most of the targeted anti-fibrotic approaches tar-
get the stromal fibroblasts due to the eventual presence
of myofibroblasts in this region, there has not been any
research on the post-wounding localization ofTGFB1 and
CTGF in the epithelium and the endothelium. A delivery
method that targets the corneal layer with maximum post-
wounding growth factor localization is critical for an ef-
fective therapy.
Delivery of drugs to the cornea is a major challenge,
as the mechanical barriers that protect the cornea (multi-
layered epithelium, tight junctions) constrain ocular drug
delivery [5]. The principal properties governing corneal
drug absorption are its lipophilicity, partition coefficient
and molecular size [6]. Nanocarriers are the potential solu-
tion for targeted ocular drug delivery as they have been
shown to be non-immunogenic, have relatively low toxi-
city, be resistant to protein/serum absorption and be sta-
ble in an enzymatic environment [7]. We have previously
showed the high efficacy of the nanoparticle kit used in
this study in delivering fluorescently labeled siRNA to all
layers of the cornea including the endothelium in an ex
vivo organ culture model [8].
The overall goal of this study is to test and deliver a
previously optimized effective triple siRNA combination
to the appropriate corneal layer with high post wounding
localization of TGFB1 and CTGFso that there is a maxi-
mal reduction of scar formation in rabbits.
2. METHODS
2.1. Laser Ablation of Rabbits
Adult New Zealand Rabbits free of disease were used and
treated according to ARVO Statement for the Use of Ani-
mals in Ophthalmic and Vision Research. Excimer abla-
tion and collection of corneas was performed as previ-
ously described [9]. Briefly, rabbits were anesthetized
with isoflurane inhalation, and proparacaine eye drops
provided topical anesthesia. Laser ablations were perform-
ed to both eyes of each rabbit with a Summit SVS exici-
mer laser that is committed to animal vision research. In
this study, two different approaches were tested to obtain
the most intense scarring in the rabbits. In the first ap-
proach, using the laser in phototherapeutic keratectomy
mode, the central 6 mm diameter area of the cornea was
ablated at a dose of 160 mJ/cm2 to an initial depth of 80
microns to remove the epithelium and then the final 45
microns were ablated by placing a mesh over the cornea
to make an uneven ablation. In the second approach, us-
ing the same laser parameters, the central 6 mm diameter
area of the cornea was ablated to an even depth of 155
Copyright © 2013 SciRes. OPEN ACCESS