Combined Carbon Dioxide Laser Lateral Canthotomy and Femtosecond Laser-Assisted Cataract Surgery 131
Catalys™ Precision Laser System (Optimedica, Santa
Clara, CA, USA) combined with either cold-steel or laser
lateral canthotomy with the Nidek Unipulse CO2 laser
(Nidek, Fremont, CA, USA) between September 2012
and July 2013. Demographic data (age, sex, race), use of
anticoagulants, indications for lateral canthotomy (expo-
sure resistant factors [ERF’s]), and occurrence of post-
operative complications (infection, bleeding, non-healing
and scarring of lateral canthus, lower eyelid ectropion
and formation of conjunctival cysts and cataract surgery
complications i.e. ruptured anterior or posterior capsules,
dropped nucleus intraoperatively or hypotony, shallow/
flat anterior chamber, distorted pupil, intraocular lens
dislocation, vitreous herniation, loss of nuclear or cortical
materials into the vitreous, retinal detachment and endo-
phthalmitis) were noted for each patient. The minimum
lower eyelid length required (MR LEL) for femtosecond
laser docking with patient interface-Liquid Optic™ In-
terface (LOI) (Optimedica, Santa Clara, CA, USA) was
also determined. Cold-steel and laser lateral canthoto-
mies were compared with respect to successful comple-
tion of femtosecond laser-assisted cataract surgery. Sta-
tistical significance was assessed using the two-tailed
Fisher Exact Test.
Surgical Technique
The patient was placed on the Catalys™ Precision Laser
System operating table (Optimedica, Santa Clara, CA,
USA). The Liquid Optic™ Interface (Optimedica, Santa
Clara, CA, USA) was fitted on the eye. If the Liquid Op-
tic™ Interface could not be fitted or successful docking
could not be achieved, then the patient was prepared for
lateral canthotomy. Successful docking was defined as
achieving a suction level accepted by the Catalys™ Pre-
cision Laser System and maintained throughout the pro-
cedure. The lower eyelid length was measured and
marked with a fine tip Devon™ marking pen (Covidien,
Mansfield, MA, USA). A photograph of the lateral can-
thus of the operative eye was taken using the Nikon
7100D camera (Nikon, Melville, NY, USA). Application
of the topical anesthetic EMLA cream (APP, Lake Zu-
rich, IL, USA) to the lateral canthus of the operative eye
followed by injection of 0.5 cc of 2% Lidocaine with
1:100,000 epinephrine local anesthetic solution (Hospira,
Lake Forest, IL, USA) into the lateral canthus of the op-
erative eye was performed. The patient’s lateral canthus
of the operative eye was prepped with 5% Betadine solu-
tion. For non-laser lateral canthotomy a hemostat was
placed over the lateral canthus for 5 minutes to control
hemostasis. Tenotomy scissors were used to make an
incision into the lateral canthal commissure to achieve
the minimum lower eyelid length required for femtosec-
ond laser docking of the interface eyepiece. Pressure was
applied to the lateral canthus to control hemostasis. For
laser lateral canthotomy a non-reflective metal forceps
(Oculoplastik, Montreal, Quebec, Canada) was used to
protect the eye during laser lateral canthotomy. The lat-
eral canthal commissure was incised with the Nidek
Unipulse CO2 laser set at 5 watts in Unipulse mode level
III (mid-level between coagulation and cutting modes) to
achieve the minimum lower eyelid length required for
femtosecond laser docking. For laser lateral canthotomy
pressure to the lateral canthus was not performed. For
both cold-steel and laser lateral canthotomies no wound
closure was performed. FLACS was then performed on
all patients starting with the fitting of the LOI. The de-
tails of FLACS technique was previously described [1,2].
3. Results
An adequate exposure for fitting and successful femto-
second laser docking with the Liquid Optic™ Interface
required a minimum lower eyelid length of 32 mm.
Thirty-four eyelids (from 26 patients) were identified to
receive lateral canthotomy because of fitting failure or
loss of suction; eight patients had bilateral combined
lateral canthotomy and cataract surgery performed on
different days. The patient ages ranged from 45 to 93
years. Nineteen patients were female and seven were
male. Twenty-two were Asians and four were Caucasians.
Six patients were on anticoagulants (two on warfarin,
four on aspirin). Of these six patients, seven eyelids had
lateral canthotomy (1 eyelid with cold-steel and 6 with
laser). Post-operative follow up for all patients ranged
from 3 to 12 months.
The following exposure resistant factors were identi-
fied: small palpebral fissure (32 eyelids), excessive
squeezing (1 eyelid), excessive eye movements-nystag-
mus (2 eyes), excessive body movements (1 eye), ab-
normal eyelid-dermatochalasis (23 eyelids), entropion (1
eyelid), and abnormal conjunctiva-pingueculum (2 eyes).
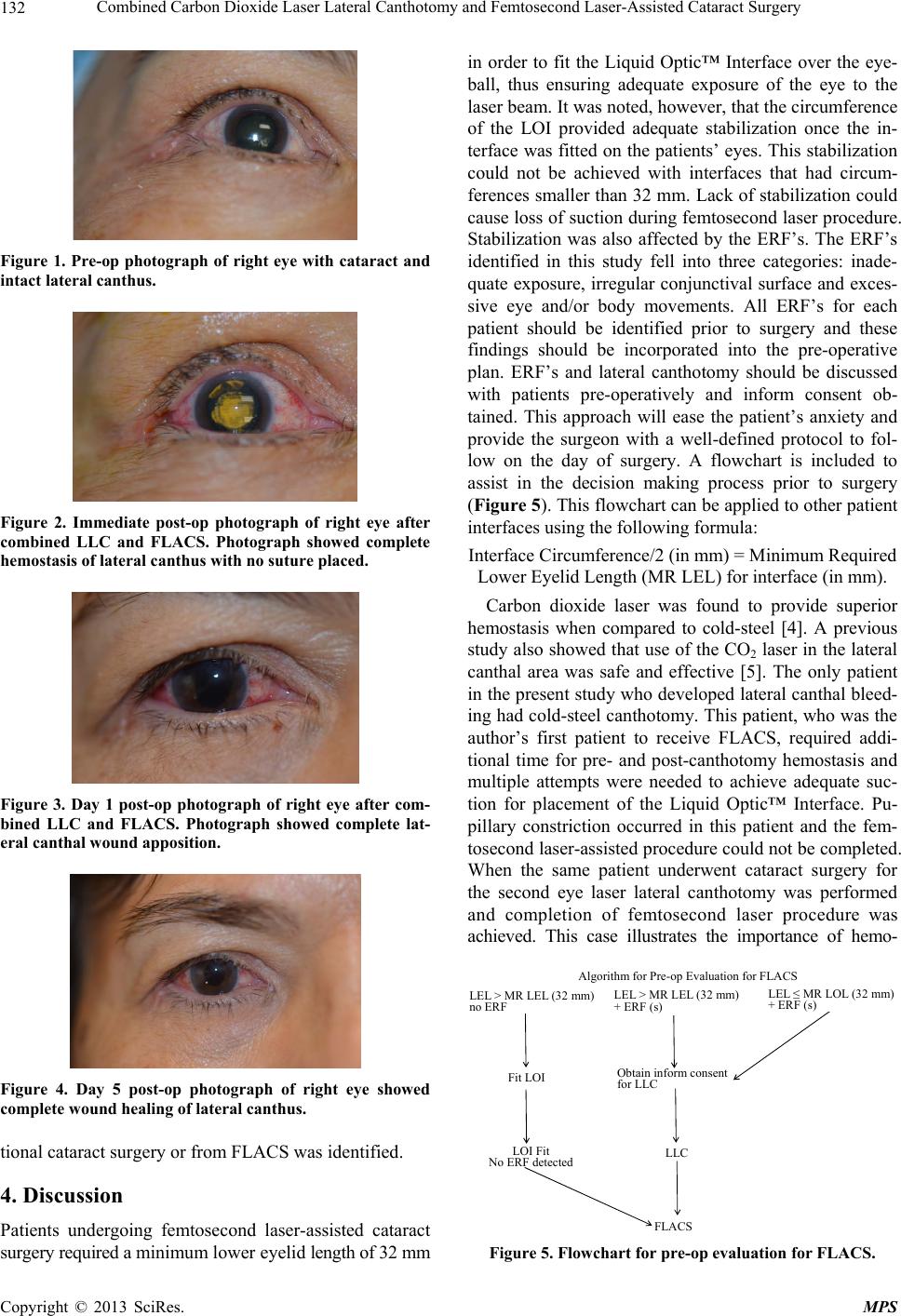
No infection, non-healing or scarring of lateral canthal
wound, conjunctival cysts, or ectropion was noted in this
study (Figures 1-4). One case of lateral canthal bleeding
occurred after cold-steel lateral canthotomy in a 93 year-
old Asian female patient who was taking anticoagulant
(warfarin) at the time of surgery. Docking was successful
in this patient but femtosecond laser procedure was not
completed because of pupillary constriction after several
docking attempts. Conventional cataract surgery, how-
ever, was performed. When this patient underwent cata-
ract surgery for the second eye laser lateral canthotomy
was performed; no canthal bleeding was noted and fem-
tosecond laser-assisted cataract surgery was completed
without complication. Comparison of cold-steel versus
laser lateral canthotomy showed that all eyes that had
laser lateral canthotomy had completion of femtosecond
laser procedure. Two-tailed Fisher Exact Test showed a
p-value of 0.0294. No complication either from conven-
Copyright © 2013 SciRes. MPS