H. El-Garem et al. / Open Journal of Gastroenterology 3 (2013) 289-294 293
Another study reported that urinary trypsinogen-2 had
a 94% sensitivity for diagnosing acute pancreatitis [6],
Hedstrom et al., (1996) [15] also reported that the level
of trypsinogen-2 correlated with the severity of acute
pancreatitis.
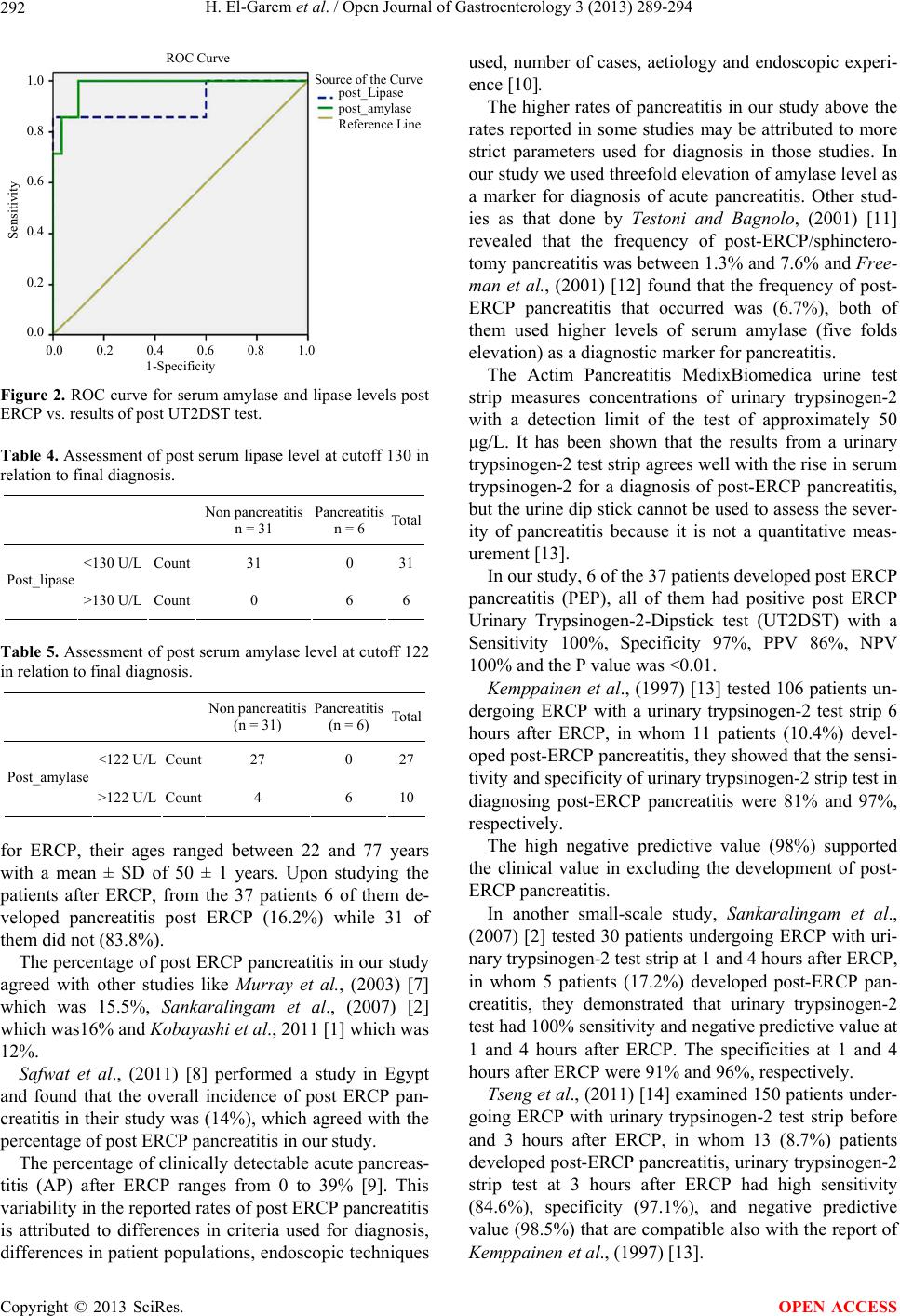
Serum levels of amylase and lipase were examined at
6 hours after ERCP procedure in our study. We found
that the elevations of serum lipase have high negative
and positive predictive values which were both (100%),
the negative predictive value for the serum amylase was
(100%) but the positive predictive value was (60%)
which was lower than that of urinary trypsinogen-2 strip
test (86%), and there was a significant difference be-
tween levels of post ERCP amylase and lipase in both
groups.
Tseng et al., (2011) [14] examined the serum levels of
amylase and lipase at 3 hours after ERCP procedure and
found that the elevations of serum amylase or lipase (3 or
5 times normal) have high negative predictive values
(94.8% - 99.1%); however, their positive predictive va-
lues (36.4% - 42.9%) were markedly lower than that of
urinary trypsinogen-2 strip test (73.3%).
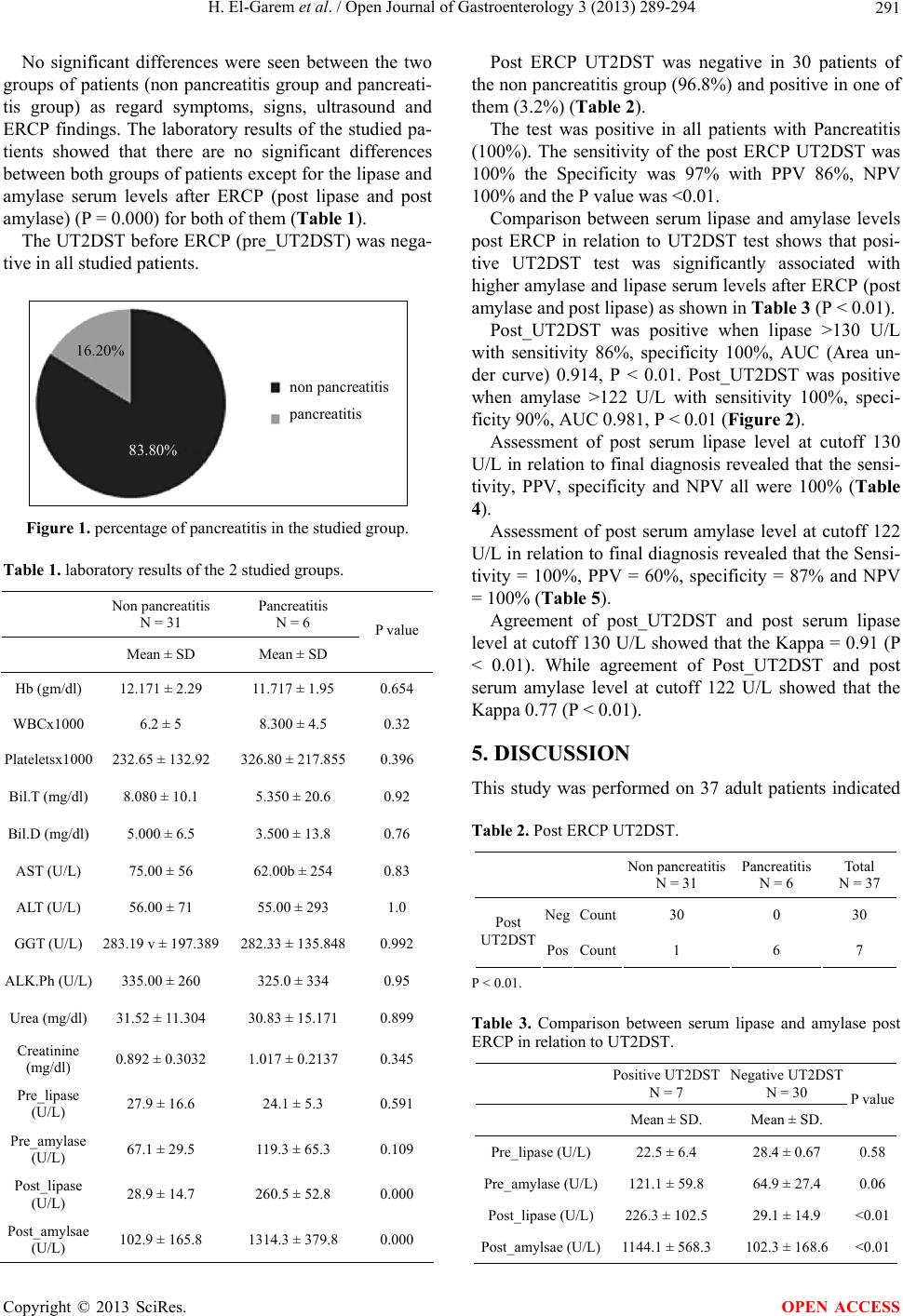
Our data showed a significantly higher mean level of
serum amylase 6 hours after ERCP in the pancreatitis
group (1314.3 ± 379.8 U/L) relative to the non pancreati-
tis group (102.9 ± 165.8 U/L) which agreed with the
Kobayashi et al., (2011) [1] study which showed that the
mean level of amylase 2 hours after ERCP in the pan-
creatitis group was (969.6 ± 220.4 U/L) relative to the
healthy group which was (120.4 ± 13.5 U/L).
However, in our study 4 of 31 cases of non-pancrea-
titis showed elevated serum levels of the amylase. In pre-
vious reports, post-ERCP levels of pancreatic enzymes in
cases with non pancreatitis peaked 6 hours after ERCP,
Kobayashi et al., 2011 [1] found that 14 of 60 cases of
non pancreatitis group showed greater than 3-fold eleva-
tion in amylase levels.
This may be due to the mechanics of the endoscopy
procedure which can cause enzymes to be reabsorbed
from the digestive tract via several mechanisms, salivary
gland stimulation associated with the insertion of a
mouthpiece or endoscope, insertion of a scope into the
gastrointestinal tract or introduction of air into the gas-
trointestinal tract [1].
Post-ERCP hyperamylasemia is reported by many au-
thors to be extremely common reaching up to 70% [16,
17].
The finding of post ERCP hyperamylasemia may be
attributed to other maneuvers used during ERCP as ma-
nipulation of the papilla during difficult cannulation,
pancreatic duct cannulation or injection, precut sphinc-
terotomy, balloon dilatation and extraction of large stones.
The mechanical trauma to the papilla or pancreatic
sphincter during instrumentation may cause transient
obstruction of outflow of pancreatic juice. Also, subject-
ing the pancreatic duct to a sudden increase in pressure
may be the cause of post ERCP hyperamylasemia. Pas-
sage of common bile duct stones is also known to cause
hyperamylasemia [18].
In conclusion, the urinary trypsinogen-2 dipstick test
can be used as an easy and rapid test for early diagnosis
of post-ERCP pancreatitis with high sensitivity and
specificity and can help clinicians to provide intensive
care and possible medical treatment as early as possible.
REFERENCES
[1] Kobayashi, K., Sasaki, T., Serikawa, M., Inoue, M.,
Itsuki, H. and Chayama, K. (2011) Assessment of trypsi-
nogen-2 levels as an early diagnostic marker for post en-
doscopic retrograde cholangio-pancreatography pancrea-
titis. Pancreas, 40, 1206-1210.
http://dx.doi.org/10.1097/MPA.0b013e318223d362
[2] Sankaralingam, S., Wesen, C., Barawi, M., Galera, R. and
Lloyd, L. (2007) Use of the urinary trypsinogen-2 dip
stick test in early diagnosis of pancreatitis after endo-
scopic retrograde cholangiopancreatography. Surgical En-
doscopy, 21, 1312-1315.
http://dx.doi.org/10.1007/s00464-006-9099-2
[3] Chen, C.C., Wang, S.S., Lu, R.H., Lu, C.C., Chang, F.Y.
and Lee, S.D. (2003) The early changes of serum proin-
flammatory and anti-inflammatory cytokines after endo-
scopic retrograde cholangiopancreatography. Pancreas,
26, 375-380.
http://dx.doi.org/10.1097/00006676-200305000-00011
[4] Ito, K., Fujita, N., Noda, Y., Kobayashi, G., Horaguchi, J.,
Takasawa, O. and Obana, T. (2007) Relationship between
post-ERCP pancreatitis and the change of serum amylase
level after the procedure. World Journal of Gastroen-
terology, 13, 3855-3860.
[5] Chang, K., Lu, W., Zhang, K., Jia, S., Li, F., Wang, F.,
Deng, S. and Chen, M. (2012) Rapid urinary trypsino-
gen-2 test in the early diagnosis of acute pancreatitis: A
meta-analysis. Clinical Biochemistry, 45, 1051-1056.
http://dx.doi.org/10.1016/j.clinbiochem.2012.04.028
[6] Kemppainen, E.A., Hedström, J.I., Puolakkainen, P.A.,
Sainio, V.S., Haapiainen, R.K., Perhoniemi, V., Osman,
S., Kivilaakso, E.O. and Stenman, U.H. (1997) Rapid
measurement of urinary trypsinogen-2 as a screening test
for acute pancreatitis. New England Journal of Medicine,
336, 1788-1793.
http://dx.doi.org/10.1056/NEJM199706193362504
[7] Murray, B., Carter, R., Imrie, C., Evans, S. and O’Suil-
leabhain, C. (2003) Diclofenac reduces the incidence of
acute pancreatitis after endoscopic retrograde cholangio-
pancreatography. Gastroenterology, 124, 1786-1791.
http://dx.doi.org/10.1016/S0016-5085(03)00384-6
[8] Safwat, W., Anas, A., Abdel Raouf, E., Abdel Aziz, A.
and Abu EL-Ezz, M. (2011) Incidence of pancreatitis in
failed versus successful ERCP and the possible benefit of
pancreatic duct stenting in high risk cases. Prospective
randomized study. New York Science Journal, 4, 29-32.
Copyright © 2013 SciRes. OPEN ACCESS