 Vol.3, No.1, 43-48 (2011) Health doi:10.4236/health.2011.31009 Copyright © 2011 SciRes. Openly accessible at http://www.scir p.org/journal/HEALTH/ Unbalanced biotransformation metabolism and oxidative stress status: implications for deficient fatty acid oxidation Catharina M. Mels*, Francois H. Van der Westhuizen, Pieter J. Pretorius, Elardus Erasmus Centre for Human Metabonomics, North-West University, Potchefstroom, South Africa; *Corresponding Author: 12076341@nwu.ac.za Received 11 November 2010; revised 18 November 2010; accepted 19 November 2010. ABSTRACT The concept of accumulating xenobiotics within the human body as a health risk is well known. However, these compounds can also be endo- genous, as in the case of inborn errors of me- tabolism, and lead to some of the same symp- toms as seen in xenobiotic intoxication. Bio- transformation of both exogenous and endo- genous toxic compounds is an important func- tion of the li v er, and the critical balan ce between these systems is of fundamental importance for cellular health. We propose a novel model, to describe the critical balance between Phase I and Phase II biotransformation and how a dis- turbance in this balance will increase the oxida- tive stress status, with resulting pathological consequences. We further used deficient fatty acid oxidation to verify the proposed model, as deficient fatty acid oxidation is associated with the accumulation of characteristic metabolites. These accumulating metabolites undergo both Phase I and Phase II biotransformation reac- tions, with resulting depletion of biotransforma- tion substrates and co-factors. Depletion of these important biomolecules is capable of disturbing the balance between Phase I and Phase II reactions, and disturbance of this bal- ance will increase oxidative stress status. The value of the proposed model is illustrated by its application to a clinical case investigated in our laboratory. In this case the possibility of defi- cient fatty acid oxidation only became evident once the critical balance between Phase I and Phase II biotransformation was restored with oral replenishment of biotransformation sub- strates. In addi tion to biochemical im provement, there was also significant clinical improvement. The significance of this model lies within the treatment possibilities, as the assessment of biotransformation metabolism and oxidative stress status can lead to the development of nutritional treatment strategies to correct im- balances. This in turn may reduce the chances of, or delay the onset of certain disease states. Keywords: Biotransformation Metabolism; Detoxification; Fatty Acid Oxidation; Oxidative Stress Status 1. INTRODUCTION The indispensable role of the liver in the biotransfor- mation or detoxification of a variety of exogenous and endogenous compounds is accomplished by two groups of enzymatic modifications known as Phase I and Phase II biotransformation metabolism. Phase I reactions ex- pose functional groups to form reactive sites, which im- prove water solubility of the compound itself, or allow Phase II reactions to ensue when the products of Phase I biotransformation are conjugated with endogenous hy- drophilic compounds to enhance their excretion [1-3]. However, during Phase I functionalization the resultant reactive molecule can in certain cases be more toxic than the parent compound, and effective neutralization of these noxious compounds is important in preventing covalent binding of the reactive metabolites to proteins, lipids and nucleic acids [2,3]. Maintaining the balance between Phase I and Phase II reactions is therefore of paramount importance, and un- der normal circumstances these enzymes function ade- quately to minimize inefficient detoxification and poten- tial induced intracellular damage. However, an over- loaded or unbalanced system negatively affects the oxidative stress status, with serious health compromi sing consequences [ 3,4]. The metabolic processes that are fundamental for maintaining normal cell structure and fun ction are highly regulated enzyme catalyzed processes. Defects in these enzyme systems, whether induced or inherited, have  C. M. Mels et al. / Health 3 (2011) 43-48 Copyright © 2011 SciRes. Openly accessible at http: //www.scirp.org/journal/HEALTH/ significant consequences in man, i.e. the accumulation of toxic substrates upstream of the enzyme defect, distur- bances in metabolic intermediates downstream of the enzyme defect, and the formation of intermediates by alternative biochemical pathways [5]. On a clinical level these biochemical aberrations will give rise to various pathological conditions including acute life-threatening encephalopathy, hyperammonemia, metabolic acidosis, hypoglycemia, jaundice and liver dysfunction [6]. This can ultimately lead to the development of chronic dis- eases and eventual death. Biotransformation metabolism is a well studied dis- cipline within the pharmaceutical industry, and the con- cept of accumulating xenobiotics within the human body as a health risk is well known. However, the accumula- tion of endogenous compounds in the case of inborn errors of metabolism and its pathological consequences is typically not explicitly associated with unbalanced biotransformation metabolism. Explaining the development of the phenotypic cha- racteristics of metabolic diseases is a formidable chal- lenge. To this end we propose a model to help explain the pathological outcomes of induced and inborn errors of metabolism. This model entails that unbalanced bio- transformation metabolism due to depletion of Phase II substrates and co-factors can be the first linkage in a chain of events with severe pathological outcomes. It is vital for scientific advan cement and clinical applications that the phenomenon of unbalanced biotransformation metabolism be considered as a primary cause of meta- bolic aberrations manifesting as increased oxidative stress status. The proposed unbalanced biotransforma- tion metabolism model will be illustrated using d efective β-oxidation of fatty acids, and its value will be demon- strated by its application in the development of individu- alized treatment protocols for patients suffering from induced and/or inborn errors of metabolism. 2. THE UNBALANC ED BIOTRANSFORMATION METABOLISM MODEL In the unbalanced biotransformation metabolism model, a hypothesis is proposed to describe the critical balance between Phase I and Phase II biotransformation and how a disturbance in this balance will increase the oxidative stress status, with resulting pathological con- sequences. A defect in, or inhibition of any one of the many enzymes involved in cellular metabolism results in the accumulation of specific metabolites that need to be removed from the body either via alternative pathways or by Phase I and Phase II biotransformation metabolism. Phase I biotransformation of accumulating metabolites and alternative pathways, both result in additional for- mation of reactive oxygen species (ROS). Induced Phase I biotransformation w ill furthermore increase the burden on Phase II conjugation and the increased demand on the latter could lead to the depletion of conjugation sub- strates and co-factors. Depletion of these biomolecules will disturb the critical balance between Phase I and Phase II biotransformation, which will further increase the oxidative stress status, ultimately leading to the dep- letion of the endogenous antioxidant capability, further affecting Phase II conjugation. Increased circulating ROS will cause oxidative damage to macromolecules such as lipids, proteins, and nucleic acids, and some of these adducts will contribute to the depletion of endo- genous antioxidants. If these reactive adducts are not neutralized effectively they can diffuse to different sites and intensify the effects of oxidative damage by de- creasing respiratory chain activity. This model therefore proposes that unbalanced biotransformation metabolism form an additional “vicious cycle” for increased oxida- tive stress status which originates from inefficient bio- transformation. 3. REGULATION OF THE CRITICAL BALANCE BETWEEN PHASE I AND PHASE II BIOTRANSFORMATION METABOLISM Biotransformation metabolism is under homeostatic regulation to control the detoxification of xenobiotics and their metabolites. This homeostatic system includes both negative feedback control as well as feedforward processes. In Phase I negative feedback control, xeno- biotics activate a range of receptors to induce Phase I enzymes [7]. In most cases Phase I activity prepares the arena for Phase II conjugation to take place, because the Phase I intermediate metabolites activate transcription factors to induce synthesis of Phase II conjugation en- zymes, also by means of negative feedback control [2 ,3]. However, many Phase II enzymes are also upregulated directly by the parent xenobiotic, which entails feedfor- ward control by the reactive metabolites formed during Phase I. This reduces the response time for the biotrans- formation system to adapt and remove harmful Phase I intermediates more rapidly. However, there are also oth- er factors involved in this process, such as nutrient con- centration control [7]. Phase I biotransformation requires little nutritional support, whereas Phase II requires vari- ous co-factors and substrates, which must be replenished by dietary sources [2,3]. Therefore, although biotrans- formation metabolism is under homeostatic regulation which includes both negative feedback and feedforward control, depletion of Phase II substrates and co-factors 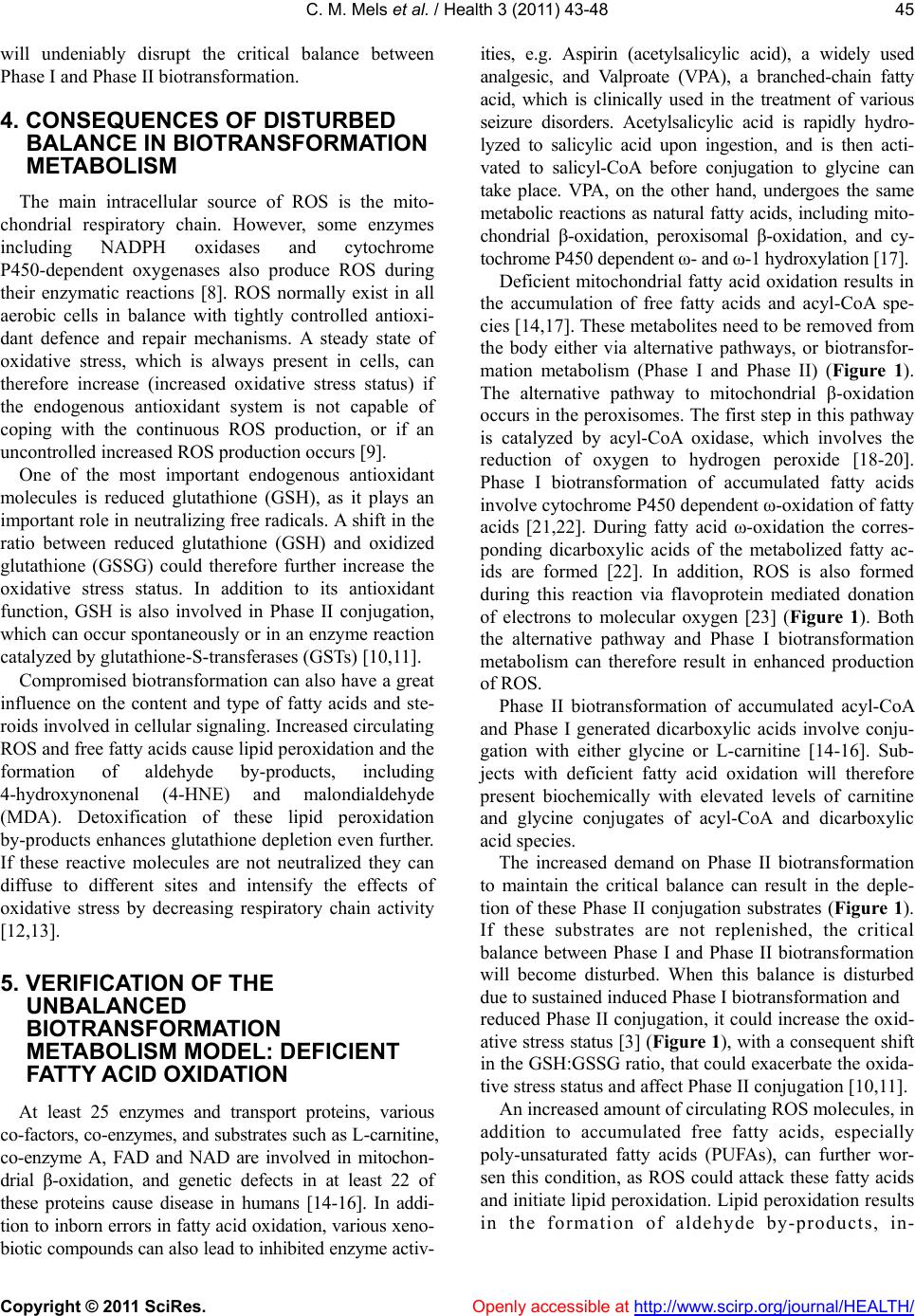 C. M. Mels et al. / H ealth 3 (2011) 43-48 Copyright © 2011 SciRes. Openly accessible at http:/ /www.scir p.org/journal/HEALTH/ will undeniably disrupt the critical balance between Phase I and Phase II biotransformation. 4. CONSEQUENCES OF DISTURBED BALANCE IN BIOTRANSFORMATION METABOLISM The main intracellular source of ROS is the mito- chondrial respiratory chain. However, some enzymes including NADPH oxidases and cytochrome P450-dependent oxygenases also produce ROS during their enzymatic reactions [8]. ROS normally exist in all aerobic cells in balance with tightly controlled antioxi- dant defence and repair mechanisms. A steady state of oxidative stress, which is always present in cells, can therefore increase (increased oxidative stress status) if the endogenous antioxidant system is not capable of coping with the continuous ROS production, or if an uncontrolled increased ROS production occurs [9]. One of the most important endogenous antioxidant molecules is reduced glutathione (GSH), as it plays an important role in neutralizing free radicals. A shift in the ratio between reduced glutathione (GSH) and oxidized glutathione (GSSG) could therefore further increase the oxidative stress status. In addition to its antioxidant function, GSH is also involved in Phase II conjugation, which can occur spontaneously or in an enzyme reaction catalyzed by glutathione-S-transferases (GSTs) [10,11]. Compromised biotransformation can also have a great influence on the content and type of fatty acids and ste- roids involved in cellular signaling. Increased circulating ROS and free fatty acids cause lipid peroxidation and the formation of aldehyde by-products, including 4-hydroxynonenal (4-HNE) and malondialdehyde (MDA). Detoxification of these lipid peroxidation by-products enhances glutathione depletion even further. If these reactive molecules are not neutralized they can diffuse to different sites and intensify the effects of oxidative stress by decreasing respiratory chain activity [12,13]. 5. VERIFICATION OF THE UNBALANCED BIOTRANSFORM ATION METABOLISM MODEL: DEFICIENT FATTY ACID O XIDATION At least 25 enzymes and transport proteins, various co-factors, co-enzymes, and sub strates such as L -carnitine, co-enzyme A, FAD and NAD are involved in mitochon- drial β-oxidation, and genetic defects in at least 22 of these proteins cause disease in humans [14-16]. In addi- tion to inborn errors in fatty acid oxidation, various xeno- biotic compounds can also lead to inhibited enzyme activ- ities, e.g. Aspirin (acetylsalicylic acid), a widely used analgesic, and Valproate (VPA), a branched-chain fatty acid, which is clinically used in the treatment of various seizure disorders. Acetylsalicylic acid is rapidly hydro- lyzed to salicylic acid upon ingestion, and is then acti- vated to salicyl-CoA before conjugation to glycine can take place. VPA, on the other hand, undergoes the same metabolic reactions as natural fatty acids, including mito- chondrial β-oxidation, peroxisomal β-oxidation, and cy- tochrome P450 dependent ω- and ω-1 hy drox yla tion [17]. Deficient mitochondrial fatty acid oxidation results in the accumulation of free fatty acids and acyl-CoA spe- cies [14,17]. These metabolites need to be removed from the body either via alternative pathways, or biotransfor- mation metabolism (Phase I and Phase II) (Figure 1). The alternative pathway to mitochondrial β-oxidation occurs in the peroxisomes. The first step in this pathway is catalyzed by acyl-CoA oxidase, which involves the reduction of oxygen to hydrogen peroxide [18-20]. Phase I biotransformation of accumulated fatty acids involve cytochrome P450 dependent ω-oxidation of fatty acids [21,22]. During fatty acid ω-oxidation the corres- ponding dicarboxylic acids of the metabolized fatty ac- ids are formed [22]. In addition, ROS is also formed during this reaction via flavoprotein mediated donation of electrons to molecular oxygen [23] (Figu re 1). Both the alternative pathway and Phase I biotransformation metabolism can therefore result in enhanced production of ROS. Phase II biotransformation of accumulated acyl-CoA and Phase I generated dicarboxylic acids involve conju- gation with either glycine or L-carnitine [14-16]. Sub- jects with deficient fatty acid oxidation will therefore present biochemically with elevated levels of carnitine and glycine conjugates of acyl-CoA and dicarboxylic acid species. The increased demand on Phase II biotransformation to maintain the critical balance can result in the deple- tion of these Phase II conjugation substrates (Figure 1). If these substrates are not replenished, the critical balance between Phase I and Phase II biotransformation will become disturbed. When this balance is disturbed due to sustained induced Phase I biotransformation and reduced Phas e II conjugation, it cou ld increase the oxid- ative stress status [3] (Figu re 1), with a consequent shift in the GSH:GSSG ratio, that could exacerbate the oxida- tive stress status and affect Phase II conjugat ion [10,11]. An increased amount of circulating ROS molecules, in addition to accumulated free fatty acids, especially poly-unsaturated fatty acids (PUFAs), can further wor- sen this condition, as ROS could attack these fatty acids and initiate lipid peroxidation. Lipid peroxidation results in the formation of aldehyde by-products, in-  C. M. Mels et al. / Health 3 (2011) 43-48 Copyright © 2011 SciRes. Openly accessible at http: //www.scirp.org/journal/HEALTH/ Figure 1. Disturbance in the critical balance between Phase I and Phase II biotransformation metabolism by deficient fatty acid oxidation can ultimately lead to an increased oxidative stress status, which is the underlying mechanism for the development of various pathologies. cluding 4-hydroxynonenal (4-HNE) and malondialde hyde (MDA) [12,13]. Increased presence and distribu- tion of these peroxidized lipid metabolites could fur- thermore lead to mitochondrial instability, as phospholi- pids are an indispensable constituent in mitochondrial membranes for the functional assembly of the respirato- ry chain. The incorporation of these lipid derivatives into mitochondria could therefore lead to decreased respira- tory chain activity, with resulting increased oxidative stress status [13]. Moreover, it has recently been demonstrated that two of the accumulating free fatty acids in MCAD deficiency (octanoate and decanoate) lead to increased oxidative stress status [24], and the uncoupling of oxidative phos- phorylation [25] in rat brain tissue. Unbalanced bio- transformation metabolism and the consequent increase in oxidative stress status are therefore a possible cause in the development of certain neurological consequences in these kinds of deficiencies. In addition to an increased oxidative stress status, the disturbed biotransformation balance can also generate the pathological condition known as co-enzyme A (CoA) sequestration, toxicity and redistribution (CASTOR) [26]. This phenomenon has been demonstrated in both inborn fatty acid oxidation deficiencies and xenobiotic induced fatty acid oxidation deficiencies [17,26]. The accumulation of acyl-CoA intermediates will lead to decreased availability of free CoA and acetyl-CoA mo- lecules, and changes in these levels can disrupt various metabolic pathways. These metabolic pathways include the Krebs cycle, ureagenesis, biotransformation path- ways as well as the mitochondrial redox state. It could also lead to further deficiencies in downstream products within these metabolic pathways [26]. Taken together, defective fatty acid oxidation and its concomitant bio- chemical characteristics clearly verify the proposed un- balance d bi otransfor mation metabolism model. 6. IN VIVO APPLICATION OF THE UNBALANCED BIOTRANSFORMATION METABOLISM MODEL The value of the proposed model is illustrated by its application to a clinical case investigated in our labora- tory. A non-smoking female Caucasian, 57 years of age presented with chronic fatigue, coughing, dyspnoea, pain and anorexia and was diagnosed with metastatic small cell carcinoma of the lung. The cancer also metastasized to the liver although liver function tests were within the reference range. After the diagnosis she was started on a chemo combination therapy, called CAV, which consists of Cyclophosphamide, Doxorubicin and Vincristine for six repeated cycles over a period of twenty weeks. For the whole assessment time she continued with a pre- scribed medication regimen consisting of: Epilim (so- dium valproate), Lamicton (Lamotrigine), Leponex (Clozapine) and Simvastin (Simvastatin, ascorbic acid and butylated hydroxyanisole). Four weeks before the end of chemotherapy, the sub- ject suffered from severe fatigue and the first biotrans- formation and oxidative stress status assessments were done. This assessment was performed by challenging Phase I and Phase II biotransformation reactions with appropriate pr ob e substrates. Caffeine was used as a probe substrate for CYP1A2 activity (Phase I), and paraceta mol and aspirin as probe substrates for glucuronide conjuga- tion, sulfate conjugation, glutathione conjugation and glycine conjugation (Phase II) [3]. In addition to this, the total acylcarnitine profile and oxidative stress status pa- rameters including the ferric reducing antioxidant power (FRAP assay), the ROS assay, measurement of hydroxyl radical markers like catechol and 2,3-dihydroxybenzoic acid (2,3-DHBA) as well as the determination of total glutathione were also included in this assessment. From the results obtained during th e initial assessment, it was evident that the biotransfo rmation metabolism and antioxidant defense systems of this subject were func- tioning below normal. The activity of Phase I (CYP1A2) measured as the caffeine clearance value, as well as all the measured end products for the different Phase II conjugation reactions were also in the lower part of the reference range, with glycine conj ugation being very low. The measured concentration of free carnitine was just within the reference range. The total glutathione (GSH  C. M. Mels et al. / H ealth 3 (2011) 43-48 Copyright © 2011 SciRes. Openly accessible at http:/ /www.scir p.org/journal/HEALTH/ and GSSG) concentration was low, with ROS levels and 2,3-DHBA levels being exceptionally high. The results of this initial assessment were used to de- velop an individualized nutritional supplementation pro- tocol in which various compounds that can be divided into different classes including antioxidants, mitochon- drial support supplementation and biotransformation substrates and co-factors were employed. After the in- troduction of this individualized nutritional treatment strategy, several follow-up investigations were per- formed over a period of 7 months to monitor both bio- chemical and clinical characteristics. Shortly after the introduction of the nutritional sup- plementation treatment, the Phase I activity was mar- kedly elevated, which could lead to the formation of more free radicals. However, after a few weeks the Phase I activity stabilized at levels well within the ref- erence range. All the Phase II reactions also improved, with considerable improvement in glucuronide, sulfate and glutathione conjugation. Although the glycine con- jugation also improved, values remained just below or just within the reference range. In addition to this the total available glutathione and the serum FRAP also in- creased with concomitant decreased ROS and 2,3-DHBA concentrations. The amount of free carnitine increased substantially after only eight w eeks of starting the supplementation regimen. However, the ratio be- tween acylcarnitines and free carnitine was slightly ele- vated. After careful investigation of the total acylcarni- tine profile, the source of the elevated ratio between acylcarnitines and free carnitine in these assessments was due to increased levels of medium-chain acylcarni- tines and medium- chain dicarboxylcarnitines, including hexanoylcarnitine, octanoylcarnitine, adipylcarnitine and suberylcarnitine. It is evident in this case that the biotransformation and antioxidant defense systems were initially markedly compromised. The identification of the accumulated metabolites usually seen in fatty acid o xidation deficien- cies is the most significant observation in this regard. Initial concentrations of Phase II substrates were so dep- leted that these metabolites were only observed after oral replenishment of the main conjugation substrate. Once the critical balance between Phase I and Phase II bio- transformation was restored, the oxidative stress status decreased to levels within the reference range. In addi- tion to the biochemical improvement, the subject also showed a significa nt clinical improvement, and although these results are only preliminary, it supports the value of the proposed unbalanced biotransformation metabol- is m mo del. 7. CONCLUSION The significance in testing this model lies within the treatment possibilities, no t only for inborn errors of fatty acid metabolism, but also for induced fatty acid oxida- tion deficiencies. It can furthermore also be significant in various metabolic aberrations manifesting as in- creased oxidative stress status. If the disturbance in this critical balance is indeed the first link in a chain of reac- tions to follow, which ultimately lead to pathological conditions like cancer, the assessment of these reactions is of immense importance. This kind of assessment can lead to the development of individualized treatment pro- tocols to replenish important substrates and co-factors needed for the safe elimination of accumulated toxic compounds. 8. ACKNOWLEDGEMENTS This work has been funded by BioPAD, Program 1: Metabolome anal- ysis (Subprogram 1.3). We would like to thank Dr J. L. Duminy at Wilmed Park Oncology Cen tre, Klerksdorp, South Africa for the clini- cal evaluation and input in the case involved. REFERENCES [1] Grant, D.M. (1991) Detoxification pathways in the liver. Journal of Inherited Metabolic Disease, 14, 421-430. doi:10.1007/BF01797915 [2] Liska, D.J. (1998) The detoxification enzyme systems. Alternative Medicine Review, 3, 187-198. [3] Liska, D., Lyon, M. and Jones, D.S. (2006) Detoxi fication and biotransformation imbalances. Explore, 2, 122-140. doi:10.1208/aapsj0903031 [4] Lampe, J.W. (2007) Diet, genetic polymorphisms, detox- ification, and health risks. Alternative Therapies in Health and Medicine, 13, S108-111. [5] Newman, M. (2004) Urinary organic acid analysis: A powerful clinical tool. Townsend Letters for Doctors and Patients, 255, 80-90. [6] Vangala, S. and Tonelli, A. (2007) Biomarkers, metabo- nomics, and drug development: Can inborn errors of me- tabolism help in understanding drug toxicity? The AAPS Journal, 9, E284-297. doi:10.1208/aapsj0903031 [7] Zhang, Q., Jingbo, P., Woods, C.G. and Andersen, M.E. (2009) Phase I to II cross-induction of xenobiotic meta- bolizing enzymes: A feedforward control mechanism for potential hormetic responses. Toxicology and Applied Pharmacology, 237, 345-356. doi:10.1016/j.taap.2009.04.005 [8] Turrens, J.F. (2003) Mitochondrial formation of reactive oxygen species. The Journal of Pysiology, 552, 335-344. doi:10.1113/jphysiol.2003.049478 [9] Cutler, R.G., Plummer, J., Chowdhury, K. and Heward, C. (2005) Oxidative stress profiling. Part II. Theory, tech- nology, a nd practice. Annals of the New York Academy of Sciences, 1055, 136-158. doi:10.1196/annals.1323.031 [10] Townsend, D.M., Tew, K.D. and Tapiero, H. (2003) The importance of glutathione in human disease. Biomedicine  C. M. Mels et al. / Health 3 (2011) 43-48 Copyright © 2011 SciRes. Openly accessible at http: //www.scirp.org/journal/HEALTH/ & Pharmacotherapy, 57, 145-155. doi:10.1016/S0753-3322(03)00043-X [11] Kidd, P.M. (1997) Glutathione: Systemic protectant against oxidative and free radical damage. Alternative Medicine Review, 2, 155-176. [12] Pamplona, R. (2008) Membrane phospholipids, lipoxida- tive damage and molecular integrity: A causal role in ag- ing and longevity. Biochimica et Biophysica Acta, 1777, 1249-1262. doi:10.1016/j.bbabio.2008.07.003 [13] Catala, A. (2009) Lipid peroxidation of membrane phos- pholipids generates hydroxy-alkenals and oxidized phospholipids active in physiological and/or pathological conditions. Chemistry and Physics of Lipids, 157, 1-11. doi:10.1016/j.chemphyslip.2008.09.004 [14] Sim, K. G.; Hammond, J. and Wilcken, B. (2002) Strate- gies for the diagnosis of mitochondrial fatty acid β-oxidation disorders. Clinica Chimica Acta, 323, 37-58. doi:10.1016/S0009-8981(02)00182-1 [15] Vockley, J.; Whiteman, D. A. H. (2002) Defects of mito- chondrial β-oxidation: A growing group of disorders. Neuromuscular Disorders, 12, 235 -246. doi:10.1016/S0960-8966(01)00308-X [16] Kompare, M. and Rizzo, W.B. (2008) Mitochondrial fatty-acid oxidation disorders. Seminars in Pediatric Neurology, 15, 140-149. doi:10.1016/j.spen.2008.05.008 [17] Fromenty, B. and Pessayre, D. (1995) Inhibition of mi- tochondrial beta-oxidation as a mechanism of hepatotox- icity. Pharmacology & Therapeutics, 67, 101-154. doi:10.1016/0163-7258(95)00012-6 [18] Cooper, T. G.; Beevers, H. (1969) β-Oxidation in glyox- ysomes from castor bean endosperm. Journal of Biolog- ical Chemistry , 244, 3514-3520. [19] Inestrosa, N.C., Bronfman, M. and Leighton, F. (1979) Detection of peroxisomal fatty acyl-coenzyme A oxidase activity. Biochemical Journal, 182, 779-788. [20] Foerster, E., Fahrenkemper, T., Rabe, U., Graf, P. and Sies, H. (1981) Peroxisomal fatty acid oxidation as de- tected by H2O2 production in intact perfused rat liver. Biochemical Journal, 196, 705-712. [21] Johnson, E.F., Palmer, C.N.A., Griffin, K.J. and Hsu, M. (1996) Role of the peroxisome proliferator-activated re- ceptor in cytochrome P450 4A gene regulation. The Journal of the Federation of American Societies for Ex- perimental Biology, 10, 1241-1248. [22] Hardwick, J.P. (2008) Cytochrome P450 omega hydrox- ylase (CYP4) function in fatty acid metabolism and me- tabolic disease. Biochemical Pharmacology, 75, 2263- 2275. doi:10.1016/j.bcp.2008.03.004 [23] Hayashi, S., Yasui, H. and Sakurai, H. (2005) Essential role of singlet oxygen species in cytochrome P450-dependant substrate oxygenation by rat liver mi- crosomes. Drug Metabolism and Pharmacokinetics, 20, 14-23. doi:10.2133/dmpk.20.14 [24] Schuck, P.F.; Ferreira, G.C., Moura, A.P., Busanello, E.N . B., Tonin, A.M., Dutra-Filho, C.S. and Wajner, M. (2009) Medium-chain fatty acids accumulating in MCAD defi- ciency elicit lipid and protein oxidative damage and de- crease non-enzymatic antioxidant defenses in rat brain. Neurochemistry International, 54, 519-525. doi:10.1016/j.neuint.2009.02.009 [25] Schuck, P.F., Ferreira, G.C., Tonin, A.M., Viegas, C.M., Busanello, E.N.B., Moura, A.P., Zanatta, A., Klamt, F. and Wajner, M. (2009) Evidence that the major metabo- lites accumulating in medium-chain acyl-CoA dehydro- genase deficiency disturb mitochondrial energy homeos- tasis in rat brain. Brain Research, 1296, 117-126. doi:10.1016/j.brainres.2009.08.053 [26] Mitchell, G.A., Gauthier, N., Lesimple, A., Wang, S.P., Mamer, O. and Qureshi, I. (2008) Hereditary and ac- quired diseases of acyl-coenzyme a metabolism. Mole- cular Genetics and Metabolism, 94, 4-15. doi:10.1016/j.ymgme.2007.12.005
|