P. K. Goel et al. / World Journal of Cardiovascular Diseases 3 (2013) 448-453
452
1) The issue of arterial dominance—The circulation
needs to be first classified into right dominant (average),
right dominant (super), left dominant (PDA from LCX)
and co-dominant (PDA from RCA but PLVs from LCX)
instead of right/left dominant alone. The average right
dominant RCA has been given the weight of a RCA with
PDA and one major PLV while standard left dominant
system has entire LV supply from left circulation alone
and none from RCA while a co-dominant circulation, has
a RCA with myocardial weightage of only PDA from the
RCA and rest of the LV supply is accomplished from Cx.
A right super-dominant system is given the myocardial
weight of PDA plus ≥2 PLVs for RCA and only one or
two OMs from Cx as the case may be.
2) Similarly, a type I, II or III LAD can be pre classi-
fied and the score of the entire left tree is proportionately
increased or decreased based on the length of the LAD in
the system.
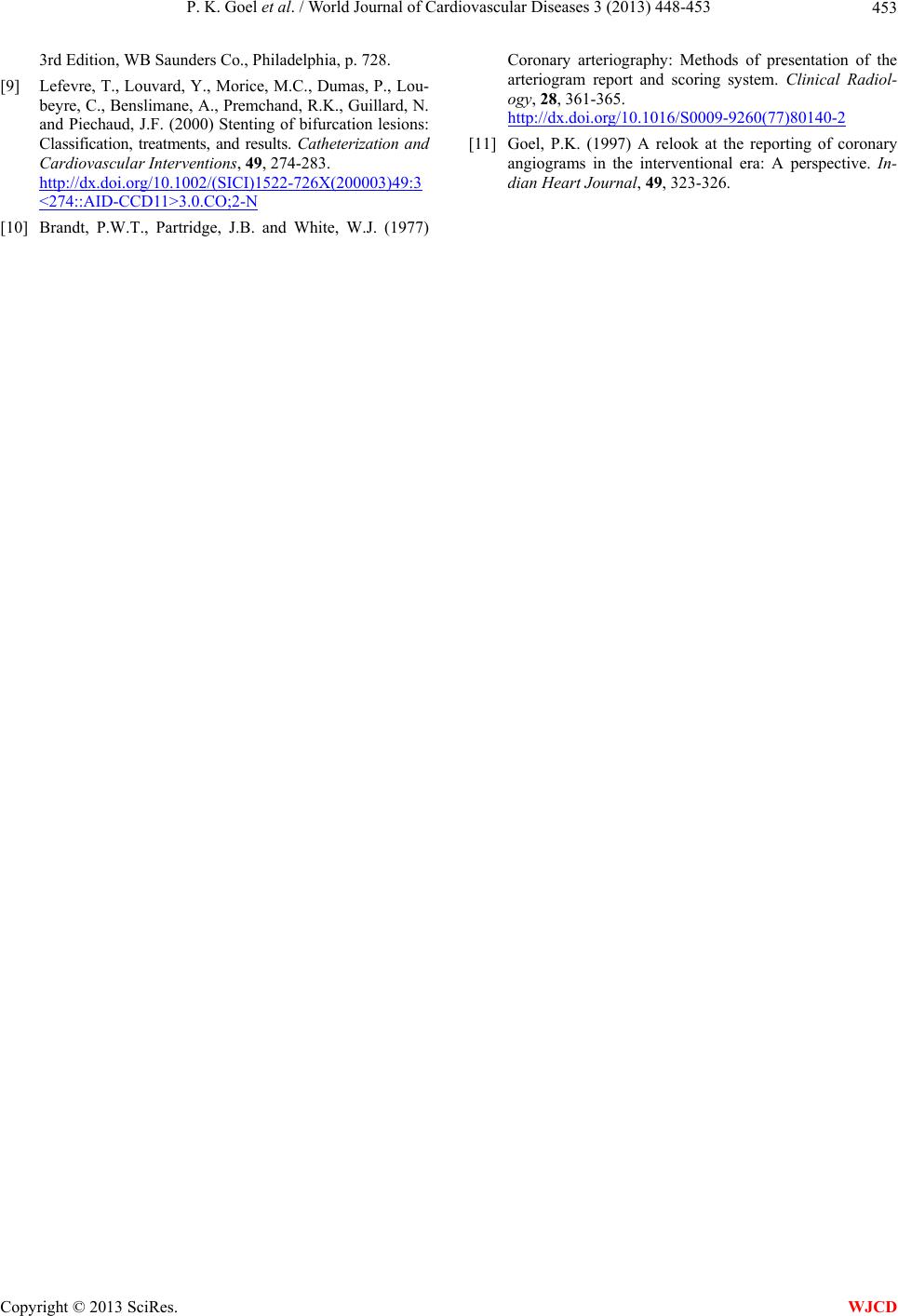
3) The total myocardial score in the Syntax system is
six with 5.0 (84% of LV) to LCA and 1.0 (16%) to PDA
while in the Greenlane system it being 15, the different
coronary segments get a proportionate score as a division
of 15. A conceptual division of myocardial score for dif-
ferent vessel segments based on the type of circulation
(Right dominant (average)/Right dominant (super)/left
dominant/co-dominant) and type I/II/III LAD is shown in
table attached in detail (Table 1 ). As an example an av-
erage RCA would contribute a score of 3.5/15 with 2/15
from PDA and 1.5/15 from PLV, which makes about 23%
of the LV myocardium as against 16% in the syntax sys-
tem and so on.
4) The Greenlane scoring system which was formu-
lated during the non interventional era of cardiology
gives a simple understanding to intervene in any vessel
when it has a myocardial value of 1.5 which in a way is a
vessel supplying 10% of the entire LV myocardial supply
and seems logically more correct than sticking to the 1.5
mm calibre criteria which has its own limitation as ex-
plained in the text above. This accounts for revasculari-
sation of PLV/OMs/Dx done based on the size of vessel
which in individual operator’s mind accounts for a myo-
cardial value of 1.5 or 10% of the entire supply of the
myocardium irrespective of its anatomical diameter.
5) A complexity factor based on LV function also can
be added which is the bottom line of all revasculariza-
tion procedural outcomes.
4. CONCLUSION
We have tried to express a viewpoint on possible
fallacies or limitations inherent in the syntax score and
present an outline of a modified remedial system and
strongly feel that a combination of the modified Green-
lane system of myocardial segment weight age as sug-
gested by us with assessment of lesion complexity as per
the syntax protocol could possibly give a complexity as-
sessment of the coronary anatomy which would be more
realistic, practical and even more precise than the current
syntax score without loss of ease for use. It would how-
ever need a large prospective study similar to the syntax
trial to adjudicate the same and such a score would then
be very close to actual decision making on PCI vs CABG
in an individual patient with multivessel disease.
REFERENCES
[1] Hannan, E.L., Wu, C., Walford, G., et al. (2008) Drug-
eluting stents vs. coronary-artery bypass grafting in mul-
tivessel coronary disease. New England Journal of Medi-
cine, 358, 331-341.
http://dx.doi.org/10.1056/NEJMoa071804
[2] Sianos, G., Morel, M.A., Kappetein, A.P., Morice, M.C.,
Colombo, A., Dawkins, K., van den Brand, M., Van
Dyck, N., Russell, M.E., Mohr, F.W. and Serruys, P.W.
(2005) The SYNTAX Score: An angiographic tool grad-
ing the complexity of coronary artery disease. EuroInter-
vention, 1, 219-227.
[3] Kappetein, A.P., Feldman, T.E., Colombo, A., et al.
(2011) Comparison of coronary bypass surgery with
drug-eluting stenting for the treatment of left main and/or
three-vessel disease: 30-year follow-up of the SYNTAX
trial. European Heart Journal, 32, 2125-2134.
http://dx.doi.org/10.1093/eurheartj/ehr213
[4] Garg, S., Sarno, G., Garcia-Garcia, H.M., et al. (2010) A
new tool for the risk stratification of patients with com-
plex coronary artery disease: The clinical SYNTAX score.
Circ. Cardiovascular Interventions, 3, 317-326.
http://dx.doi.org/10.1161/CIRCINTERVENTIONS.109.9
14051
[5] Serruys, P.W., Unger, F., van Hout, B.A., van den Brand,
M.J., van Herwerden, L.A., van Es, G.A., Bonnier, J.J.,
Simon, R., Cremer, J., Colombo, A., Santoli, C., Van-
dormael, M., Marshall, P.R., Madonna, O., Firth, B.G.,
Breeman, A., Morel, M.A. and Hugenholtz, P.G. (1999)
The ARTS study (Arterial Revascularization Therapies
Study). Seminars in Interventional Cardiology, 4, 209-
219.
[6] Leaman, D.M., Brower, R.W., Meester, G.T., Serruys, P.
and van den Brand, M. (1981) Coronary artery athero-
sclerosis: Severity of the disease, severity of angina pec-
toris and compromised left ventricular function. Circula-
tion, 63, 285-299.
http://dx.doi.org/10.1161/01.CIR.63.2.285
[7] Hamburger, J.N., Serruys, P.W., Scabra-Gomes, R.,
Simon, R., Koolen, J.J., Fleck, E., Mathey, D., Sievert, H.,
Rutsch, W., Buchwald, A., Marco, J., Al-Kasab, S.M.,
Pizulli, L., Hamm, C., Corcos, T., Reifart, N., Hanrath, P.
and Taeymans, Y. (1997) Recanalization of total coro-
nary occlusions using a laser guidewire (the European
TOTAL Surveillance Study). American Journal of Car-
diology, 80, 1419-1423.
http://dx.doi.org/10.1016/S0002-9149(97)00704-2
[8] Topol, E.J. (1998) Textbook of interventional cardiology,
Copyright © 2013 SciRes. WJCD