H. Mohammadi et al. / J. Biomedical Science and Engineering 4 (2011) 46-50
Copyright © 2011 SciRes. JBiSE
49
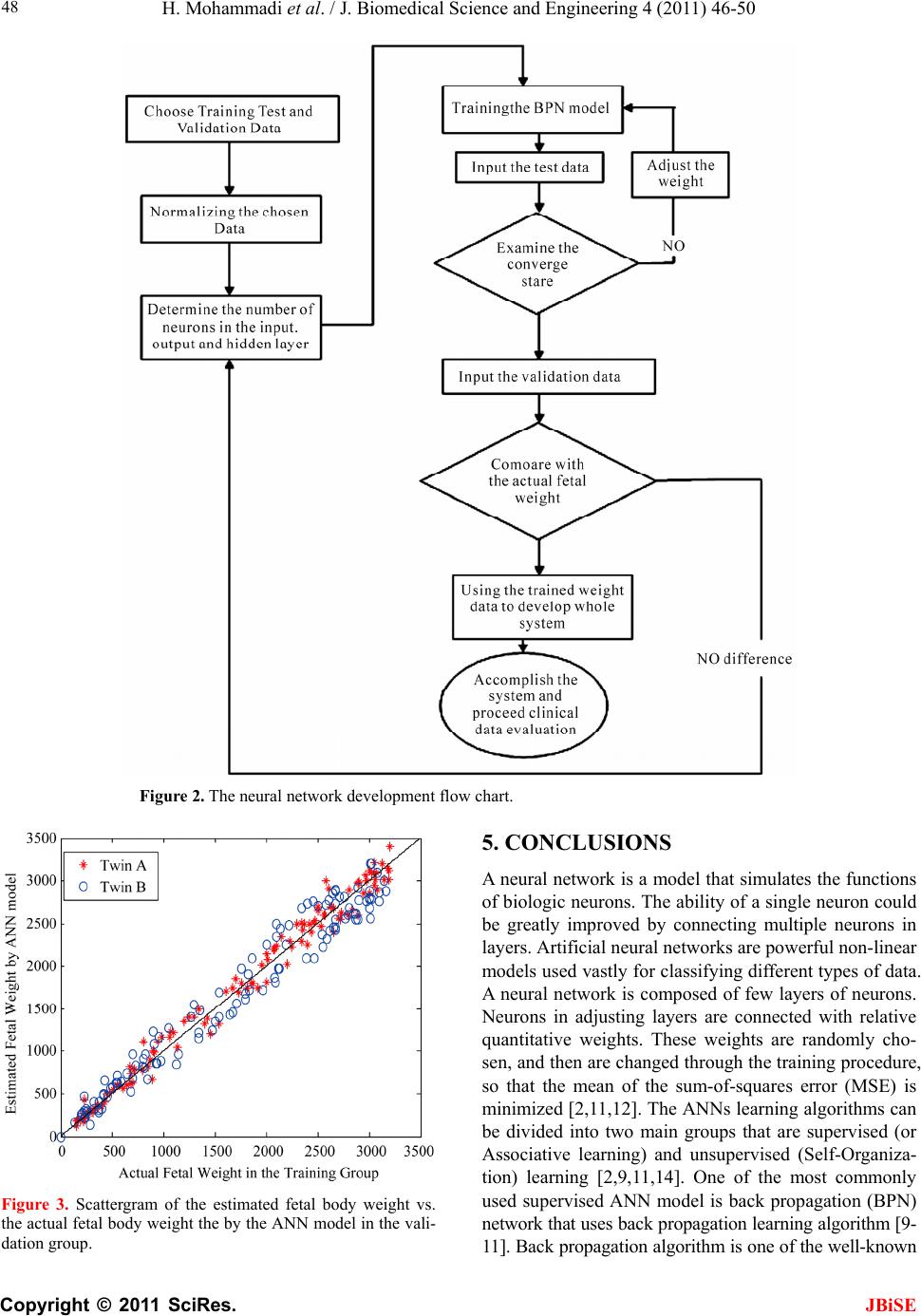
algorithms in neural networks. The back propagation
neural network is essentially a network of simple proc-
essing elements working together to produce a complex
output [11]. These elements or nodes are arranged into
different layers: input, middle and output. The output
from a back propagation neural network is computed
using a procedure known as the forward pass [2,8-11,15]:
1) The input layer propagates a particular input vector’s
components to each node in the middle layer. 2) Middle
layer nodes compute output values, which become inputs
to the nodes of the output layer. 3) The output layer
nodes compute the network output for the particular in-
put vector. The forward pass produces an output vector
for a given input vector based on the current state of the
network weights. Since the network weights are initial-
ized to random values, it is u nlikely that reasonable out-
puts will result before training . The weights are adjusted
to reduce the error by propagating the output error
backward through the network [2,9,15]. In this study, we
used the BPN algorithm to develop the ANN and prove
our hypothesis that BPD, AC and AD wi t hin A NN model
could reduce errors between estimated fetal weight and
actual fetal weight. The subjects in our series were a
group of women with healthy singleton fetus with
documentation of US examination with, BPD, AC and
AD. Some may wonder at our choice of the three input
parameters, thinking that they are not well justified. The
three dimensional variables are reasonable because of
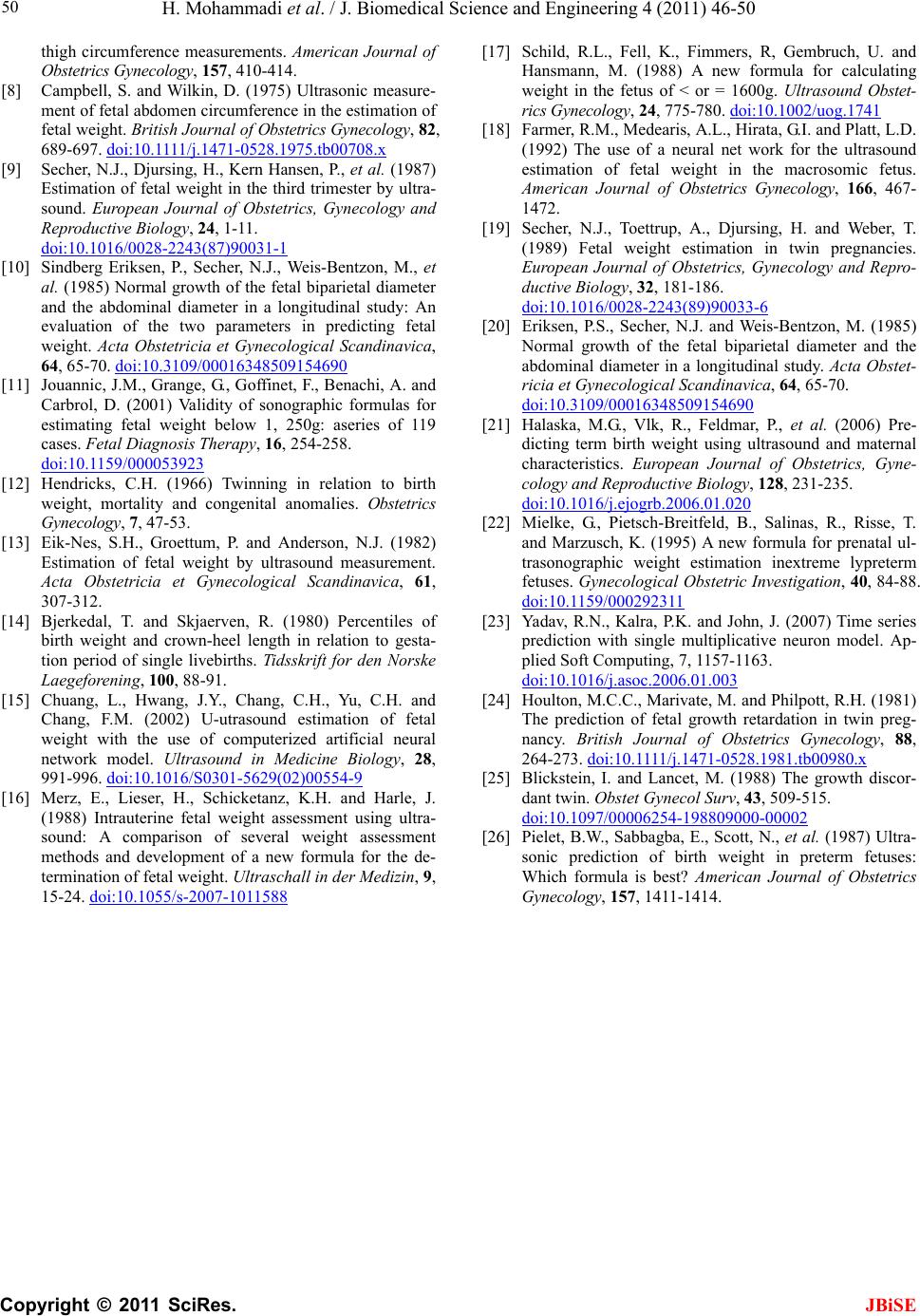
the previous literature [9]. Also, the overall, high corre-
lation between AC, AD, BPD and twin’s EFW were 0.81,
0.87 and 0.84, respectively, which shows the important
effect of these parameters on twin’s weight. In our study,
the definition of an anomaly was for any fetus with a
major structural anomaly that could be diagnosed prena-
tally, such as holoprosencephaly, omphalocele, cystic
hygroma, etc. These were excluded from the study. We
might include some fetuses with rare and nonstructural
anomalies that could only be diagnosed postnatally by
genetic screening or metabolic methods, in which the
prenatal ultrasonic examination cannot demonstrate any
structural abnormality. However, we believe that this
point makes only little impact on the stud y because these
nonstructural anomalies are too rare [9].
In our study, the mean absolute error (AE) and the
mean absolute percent error (APE) between estimated
fetal weight and actual fetal weight were 162.71 g and
7.81%, respectively. The fetuses in weight range of
(>2500 g) are the lowest accurate fetal weight estimation
in validation group (AE = 269 g, APE= 10.51%), we
think that, as the fetus grows are more quick at the last
trimester and we considered babies within 3 days of de-
livery, it might be one part of the error in this weight
range is related to fetus grows within this estimation of
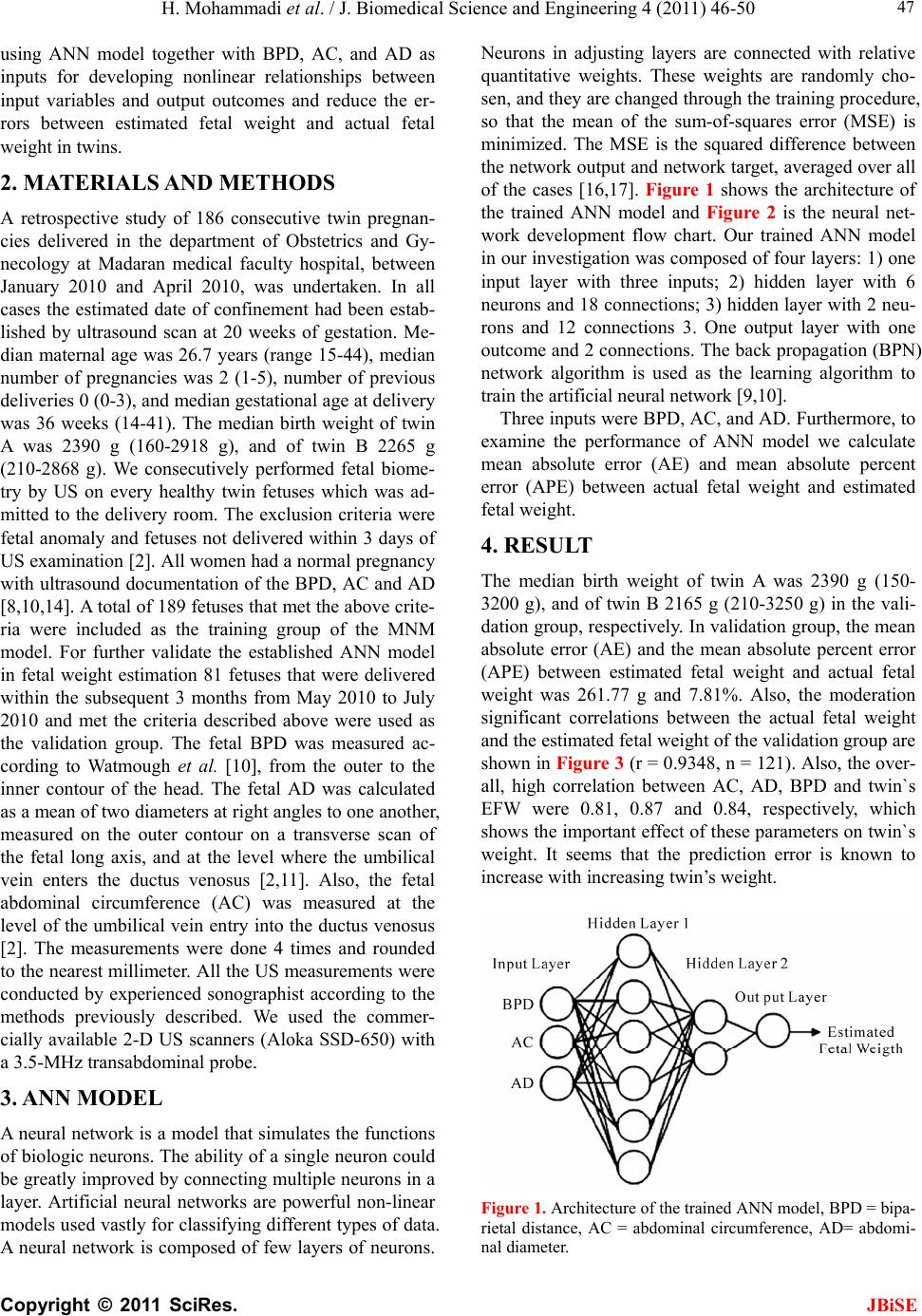
fetal weight. In th is ANN model we have 4 layers; input
layer, two median layers and output layer. We have three
input variables AC, AD and BPD. In all cases the esti-
mated date of confinement had been established by ul-
trasound scan at 20 weeks of gestation. Median maternal
age was 26.7 years (range 15-44), median number of
pregnancies was 2 (1-5), number of previous deliveries 0
(0-3), and median gestational age at delivery was 36
weeks (14-41). The median birth weight of twin A was
2390 g (160-29 18 g) , an d of tw in B 2 265 g (210 -2868 g)
in the training group. Also, the median birth weight of
twin A was 2190 g (150-3200 g), and of twin B 2165 g
(210-2868 g) in the validation group.
Also estimation of fetal weight by ANN model at the
weight range of (<1500 g) are the most accurate result. It
seems that the prediction birth weight error is known to
increase with increasing weight of twins, week by week.
In conclusion, our study demonstrates that our single
multiplicative neuron model is a well-established model
and can be used to estimate fetal weight. However, more
accuracy of fetal weight estimation is in need of further
studies.
6. ACKNOWLEDGEMENTS
This study was supported in part by grants from university of science
and research branch Islamic Azad University, Tehran. The authors are
grateful to all doctors for the ultrasound measurements; Ms. Fatemeh
Nematollahi and Ms. Fatemeh Bani and their assistance; and Ali
Ghafari at the Department of Obstetrics and gynecology, Madaran
Medical Faculty for equipment supply.
REFERENCES
[1] Hendricks, C.H. (1966) Twinning in relation to birth
weight, mortality and congenital anomalies. Obstetrics
Gynecology, 27, 47-53.
[2] Powers, W.F. (1973) Twin pregnancy, complications and
treatment. Obstetrics Gynecology, 43, 795-808.
[3] Chang, F.M., Liang, R.I., Ko, H.C., Yao, B.L., Chang, C.H.
and Yu, C.H. (1997) Threedimensional ultrasound- as-
sessed fetal thigh volumetry in predictingbirt h weight, Ob-
stetrics Gynecology, 90, 331-339.
doi:10.1016/S0029-7844(97)00280-9
[4] Manlan, G. and Scott, K.E. (1978) Contribution of twin
pregnancy to perinatal mortality and fetal growth, retar-
dation: reversal of growth retardation after birth. Cana-
dian Medical Association Journal, 118, 365-368.
[5] Secher, N.J., Kaern, J., Hansen, P.K., et al. (1985) In-
tra-uterine growth in twin pregnancies: prediction of fetal
growth retardation. Obstetrics Gynecology, 66, 63-68.
[6] Shepard, M.J., Richards, V.A., Berkowitz, R.L. Warsof,
S.L. and Hobbins, J.C. (1982) An evaluation of two
equations for predicting fetal weight by ultrasound.
American Journal of Obstetrics Gynecology, 142, 47-54.
[7] Vintzileos, A.M., Campbell, W.A., Rodis, J.F., Bors-
Koefoed, R. and Nochimson, D.J. (1987) Fetal weight
estimation formulas with head, abdominal, femur, and