 Vol.5, No.10, 1659-1666 (2013) Health http://dx.doi.org/10.4236/health.2013.510224 Moderators of occupational pressure in female health professionals—Individual differences and coping skills Siew Yim Loh*, Kia Fatt Quek Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; *Corresponding Author: syloh@um.edu.my Received 8 July 2013; revised 8 August 2013; accepted 8 September 2013 Copyright © 2013 Siew Yim Loh, Kia Fatt Quek. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Individual differences and coping skills have influential impacts on stress process by influ- encing the eventual outcomes of the stressors, contributing to either wellbeing, or illness and negative experiences. The aim of this paper is to explore the individual differences and coping strategies of a cohort of women w ith health pro- fessionals’ occup ational pressure. This is a cross- sectional survey, informed by the transactional model of stress and coping framework, and car- ried out on women health professionals (n = 203) from the Kuala Lumpur Hospit al. Multiple regres- sions were conducted to examine the potential moderators of stress. Women Health Profes- sionals reported stress with six out of eight or- ganizational sources of pressure, with relation- ship being a key stressor. Their individual dif- ferences (mean + SD) were characterised by low drive (7.6 + 1.9 - 8.2 + 2.0), low personal influ- ence (10.8 + 2.0 to 11.7 + 2.3), moderate control (13.4 + 3.4 to 16.3 + 2.4), and high impatience behaviour (19.1 + 3.8 to 20.4 + 3.3). With Coping strategy, the Life-work-balance coping is a sig- nificant positive predictor for five out of the nine outcomes of occupational pressure [state of mind (p < 0.001), level of resilience (p = 0.01), level of confidence (p = 0.003), physical symp- toms (p = 0.001) and energy level (p < 0.001)]. The findings show relationship as a key stres- sor, with a less favourable pattern of individual- differences and an over-reliance on lifework ba- lance coping. Female health professionals, stre- ssed at work, have an undesirable profile of in- dividual difference and a coping strategies, sug- gestive of attempts to balance the demands of their dual work role. The increasing female into the workforce, warrants more research to inform stress management guideline to ameliorate stress amongst those vulnerable workers. Future stu- dies to examine individual differences of these female-dominated professions across health setting are needed to better inform the pressure- at-work issues for the increasing Asian women health professionals. Keywords: Occupational Pressure; Women; Individual Differences; Coping 1. INTRODUCTION Stress at work has been the number one reason behind sickness from work, with more than two thirds of people suffering from work-related stress [1]. Stress literature showed that specific, enduring work-related stressful experiences contribute to depression [2,3], predicted as one of the three leading causes of burden of disease worldwide [4-6]. Individual differences and variability and/or reactivity may be an appropriate concept to un- derstand and ameliorate work pressure and reduce its debilitating effects [7]. The study uses the Transactional Model of Stress and Coping framework to understand the multi-factorial causes of work stress. Stress is mediated by people’s appraisal of the stressor and, by the so- cial-cultural resources at their disposal [7,8]. Significant differences exist in terms of physical and psychological wellbeing amongst the male and female workers [9,10]. Comic et al. [11] explain that role demands such as that of being wife, mother and professional provoke role con- flicts for female workers. In order to help female health professionals manage work stress, an understanding of their social and occupational role and the individual dif- ferences is fundamental. These individual differences (i.e. type-behaviour, level of patience, perception of control and personal-influence) and coping strategies (i.e. prob- Copyright © 2013 SciRes. OPEN ACCESS 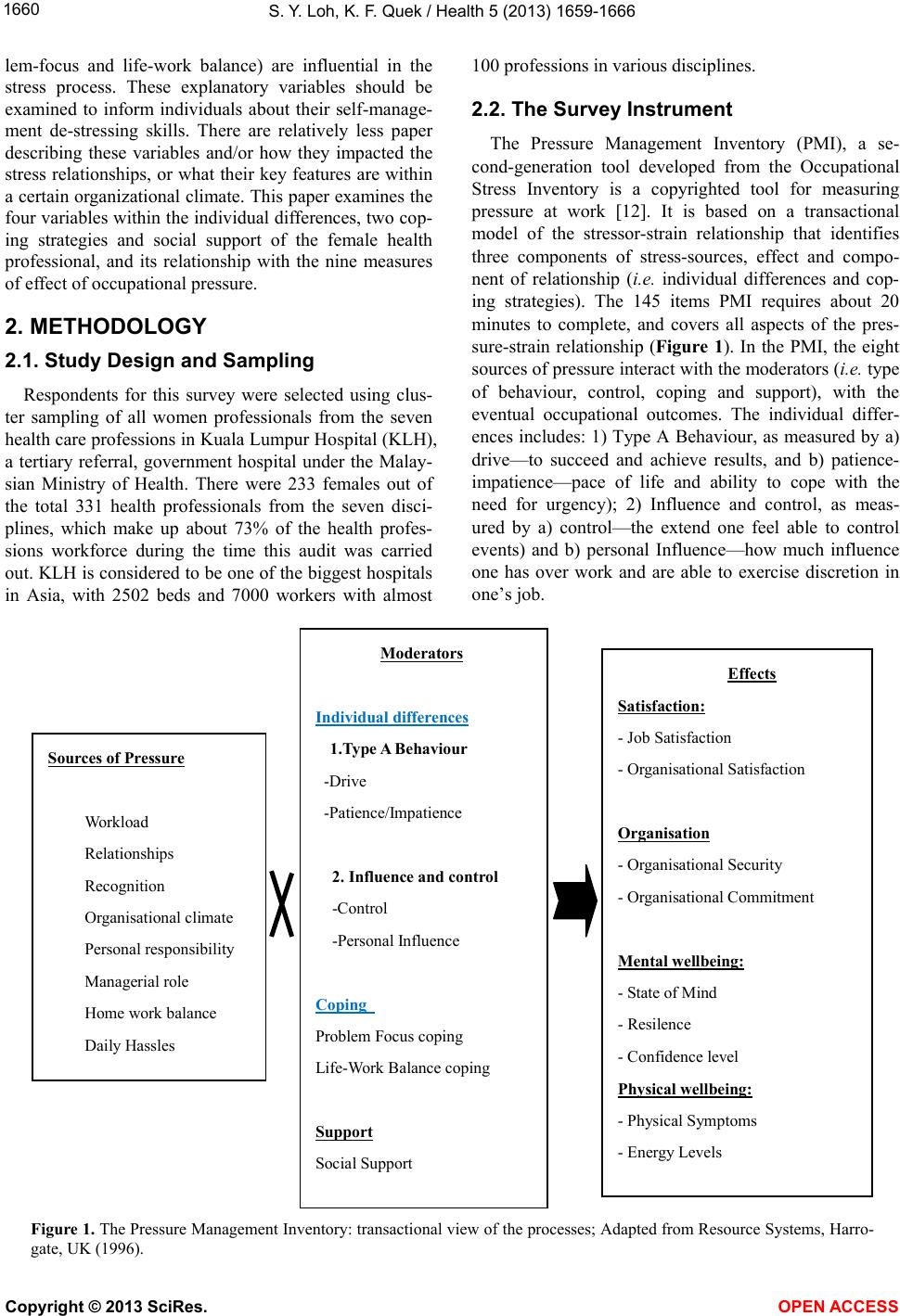 S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 1660 lem-focus and life-work balance) are influential in the stress process. These explanatory variables should be examined to inform individuals about their self-manage- ment de-stressing skills. There are relatively less paper describing these variables and/or how they impacted the stress relationships, or what their key features are within a certain organizational climate. This paper examines the four variables within the individual differences, two cop- ing strategies and social support of the female health professional, and its relationship with the nine measures of effect of occupational pressure. 2. METHODOLOGY 2.1. Study Design and Sampling Respondents for this survey were selected using clus- ter sampling of all women professionals from the seven health care professions in Kuala Lumpur Hospital (KLH), a tertiary referral, government hospital under the Malay- sian Ministry of Health. There were 233 females out of the total 331 health professionals from the seven disci- plines, which make up about 73% of the health profes- sions workforce during the time this audit was carried out. KLH is considered to be one of the biggest hospitals in Asia, with 2502 beds and 7000 workers with almost 100 professions in various disciplines. 2.2. The Survey Instrument The Pressure Management Inventory (PMI), a se- cond-generation tool developed from the Occupational Stress Inventory is a copyrighted tool for measuring pressure at work [12]. It is based on a transactional model of the stressor-strain relationship that identifies three components of stress-sources, effect and compo- nent of relationship (i.e. individual differences and cop- ing strategies). The 145 items PMI requires about 20 minutes to complete, and covers all aspects of the pres- sure-strain relationship (Figure 1). In the PMI, the eight sources of pressure interact with the moderators (i.e. type of behaviour, control, coping and support), with the eventual occupational outcomes. The individual differ- ences includes: 1) Type A Behaviour, as measured by a) drive—to succeed and achieve results, and b) patience- impatience—pace of life and ability to cope with the need for urgency); 2) Influence and control, as meas- ured by a) control—the extend one feel able to control events) and b) personal Influence—how much influence one has over work and are able to exercise discretion in one’s job. Sour ces o f Pr essur e Workload Relationships Recognition Organisational climate Personal responsibility Managerial role Home work balance Daily Hassles Moderators Individual differences 1.Typ e A Behavi our -Drive -Patience/Impatience 2. Influence and control -Control -Personal Influence Coping Problem Focus coping Life-Work Balance coping Support Social Support Effects Satisfaction: - Job Satisfaction - Organisational Satisfaction Organisation - Organisational Security - Organisational Commitment Mental wellbeing: - State of Mind - Resilence - Confidence level Physi ca l w ellbeing: - Physical Symptoms - Energy Levels Figure 1. The Pressure Management Inventory: transactional view of the processes; Adapted from Resource Systems, Harro- gate, UK (1996). Copyright © 2013 SciRes. OPEN ACCESS  S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 1661 The Coping Strategies consist of two types: 1) Prob- lem Focus coping—the extend one is able to plan ahead and manage time to deal with problems) and 2) Life- Work Balance coping—the extend one is able to separate home from work and not let things gets to oneself). So- cial Support refers to the help one gets by discussing problems or situations with other people. The instrument have been validated and showed good internal consisten- cies (alpha < 0.7) for most subscales. The test-retest cor- relation coefficients were significant at the level of p < 0.001 for almost all scale. The ICC coefficients were also high (>0.7) particularly for Pressure, Health and Coping Scales (Loh, 2004). 2.3. Data Collection Upon ethical approval from the Kuala Lumpur Hospi- tal Ethics Committee, briefings were conducted on the key representatives of seven health disciplines (Occupa- tional Therapy, Physiotherapy, Medical Laboratory Technology, Medical Dispenser, Radiotherapy and Ra- diography and Counselling, and Social work), to explain the purpose of the study. Confirmation of the where about of the health professionals were checked with the census obtained from the human resource office of each individual department. From the list, the female health professionals were identified and those servicing outside the Hospital premise were excluded to ensure the pres- sure was within the organisation. The women were in- formed of the study and were given the consent form. Those who signed the consent form were followed up with the PMI questionnaire. 2.4. Data Analyses Data analysis was performed using the SPSS version 16 (SPSS Inc., Ill., Chicago, USA. Statistical tests such as descriptive statistic, analyses of variance, independent t tests, correlations and analyses of variance (ANOVA) were used. Multiple linear regressions were performed to examine the variables on the individual differences as predictors of the effect of occupational pressure as (Fig- ure 1). 3. RESULTS 3.1. Psychometrics of PMI All items on the stressors, and outcome were found to be statistically significant. In the influential item vari- ables variable, only individual differences (r = 0.12, p > 0.05) was not found to be significant. The Cronbach Al- pha (internal consistencies) of 0.7 and above was noted for most scales (except for job satisfaction, α = 0.61, type A drive, α = 0.62; patience-impatience, α = 0.21; social support, α = 0.59) suggesting the reliability of most of the scales are acceptable. This supports most subscales met the required coefficient of 0.7 and above [13]. Items such as social support (0.59), type A (0.62), patient im- patience (0.21) and control (0.64) were all below 0.7, and thus have to be interpreted with caution. The panel of six psychiatrists provided the consensus that the PMI has face validity. However, in terms of content, the panel concurred that the PMI may pose some difficulty for the average Malaysian because of some of the ambiguous and difficult wordings in the PMI. This was the reason why PMI was supplemented with a Malay version. In addition, in term of appropriateness for measuring occu- pational pressure of female, the panel also highlighted some women-specific health-related issues and home-en- vironment issues that were not highlighted in the PMI. However, this was not included in this study where PMI was used. 3.2. Socio-Demographic Characteristic of Female Health Professionals Table 1 showed the response rate of the various pro- fessions this study, while Table 2 showed the demo- graphic background of the women. The seven profes- sions comprising of 330 workers, out of which, 72% are female workers. The response rate for this survey was 84% (Table 1). Non respondents also included those who were on leave and those servicing outside the HKL premise. About 68% were within the age range of 20 - 39 years old. Almost 80% were assigned to the lowest grade -basic entry grade (U8) within the profession. Thus, only 20% are holding the higher managerial tasks of oversee- ing these 80% workforce. In terms of ethnic group, the majority (82%) were Malays followed by the Chinese, Indians, Sikh, Eurasians and Others. About 60% were married and about half of these married women have children. Overall, only 27% claimed to engage in some form of regular exercise at least three days a week. 3.3. The Occupational Pressure of Women Health Professionals Tabl e 3 shows the mean scores for all the five group- ings of profession. Three stressors-relationship, per- sonal responsibility and organizational climate were rated consistently as the highest stressors across these professions. Standardization of mean-score of the stress- sor over the number of items within the scale, were computed to describe the ranking of stressors within the seven professions. The top three work stressors within the five clusters of professionals were presented in Table 3. Three stressors (relationship, personal responsibility and organizational climate) were rated consistently high across the various professions. There were significant differences in five of the eightsources of pressure, across Copyright © 2013 SciRes. OPEN ACCES S 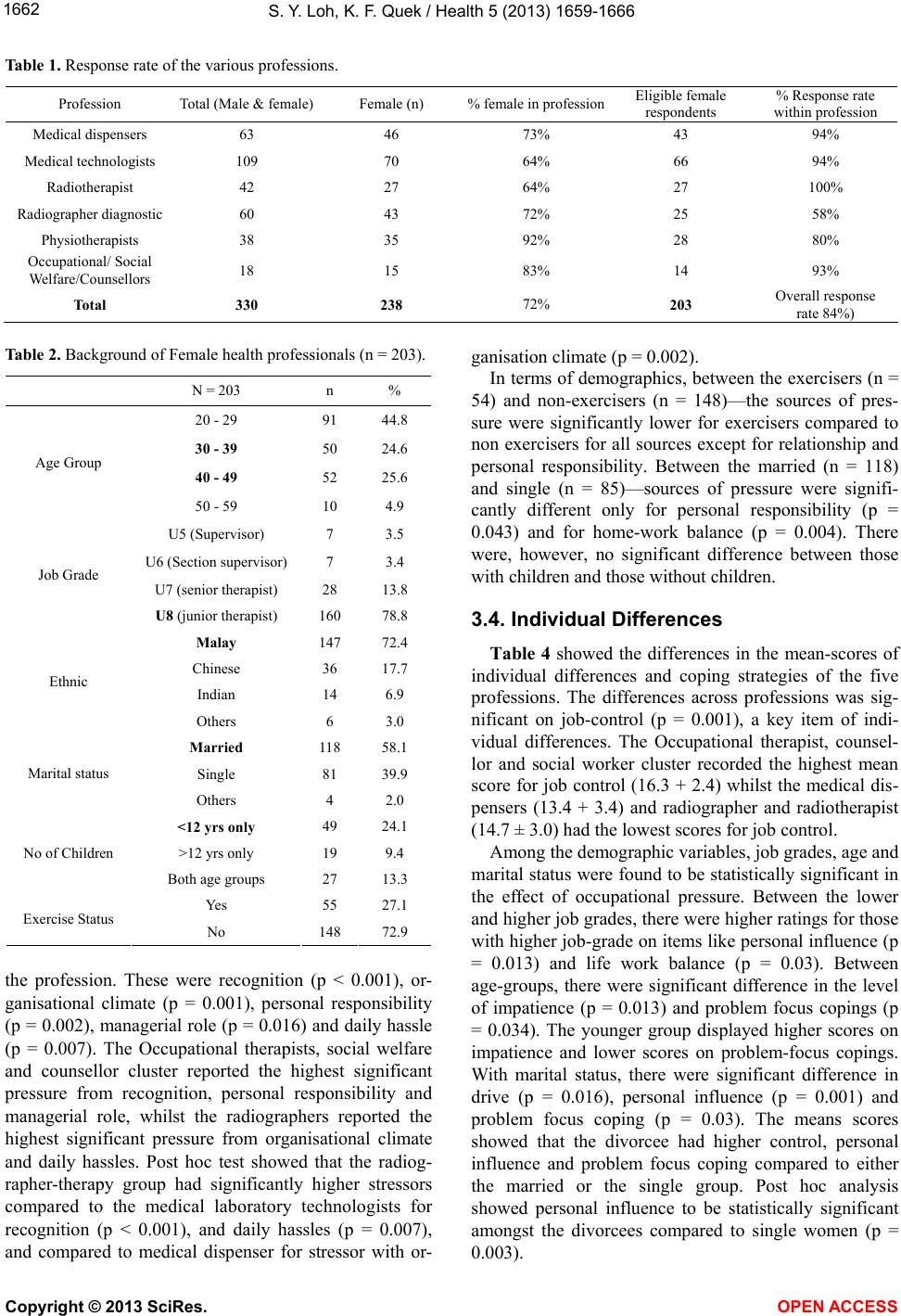 S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 1662 Table 1. Response rate of the various professions. Profession Total (Male & female) Female (n) % female in professionEligible female respondents % Response rate within profession Medical dispensers 63 46 73% 43 94% Medical technologists 109 70 64% 66 94% Radiotherapist 42 27 64% 27 100% Radiographer diagnostic 60 43 72% 25 58% Physiotherapists 38 35 92% 28 80% Occupational/ Social Welfare/Counsellors 18 15 83% 14 93% Total 330 238 72% 203 Overall response rate 84%) Table 2. Background of Female health professionals (n = 203). N = 203 n % 20 - 29 91 44.8 30 - 39 50 24.6 40 - 49 52 25.6 Age Group 50 - 59 10 4.9 U5 (Supervisor) 7 3.5 U6 (Section supervisor) 7 3.4 U7 (senior therapist) 28 13.8 Job Grade U8 (junior therapist) 160 78.8 Malay 147 72.4 Chinese 36 17.7 Indian 14 6.9 Ethnic Others 6 3.0 Married 118 58.1 Single 81 39.9 Marital status Others 4 2.0 <12 yrs only 49 24.1 >12 yrs only 19 9.4 No of Children Both age groups 27 13.3 Yes 55 27.1 Exercise Status No 148 72.9 the profession. These were recognition (p < 0.001), or- ganisational climate (p = 0.001), personal responsibility (p = 0.002), managerial role (p = 0.016) and daily hassle (p = 0.007). The Occupational therapists, social welfare and counsellor cluster reported the highest significant pressure from recognition, personal responsibility and managerial role, whilst the radiographers reported the highest significant pressure from organisational climate and daily hassles. Post hoc test showed that the radiog- rapher-therapy group had significantly higher stressors compared to the medical laboratory technologists for recognition (p < 0.001), and daily hassles (p = 0.007), and compared to medical dispenser for stressor with or- ganisation climate (p = 0.002). In terms of demographics, between the exercisers (n = 54) and non-exercisers (n = 148)—the sources of pres- sure were significantly lower for exercisers compared to non exercisers for all sources except for relationship and personal responsibility. Between the married (n = 118) and single (n = 85)—sources of pressure were signifi- cantly different only for personal responsibility (p = 0.043) and for home-work balance (p = 0.004). There were, however, no significant difference between those with children and those without children. 3.4. Individual Differences Table 4 showed the differences in the mean-scores of individual differences and coping strategies of the five professions. The differences across professions was sig- nificant on job-control (p = 0.001), a key item of indi- vidual differences. The Occupational therapist, counsel- lor and social worker cluster recorded the highest mean score for job control (16.3 + 2.4) whilst the medical dis- pensers (13.4 + 3.4) and radiographer and radiotherapist (14.7 ± 3.0) had the lowest scores for job control. Among the demographic variables, job grades, age and marital status were found to be statistically significant in the effect of occupational pressure. Between the lower and higher job grades, there were higher ratings for those with higher job-grade on items like personal influence (p = 0.013) and life work balance (p = 0.03). Between age-groups, there were significant difference in the level of impatience (p = 0.013) and problem focus copings (p = 0.034). The younger group displayed higher scores on impatience and lower scores on problem-focus copings. With marital status, there were significant difference in drive (p = 0.016), personal influence (p = 0.001) and problem focus coping (p = 0.03). The means scores showed that the divorcee had higher control, personal influence and problem focus coping compared to either the married or the single group. Post hoc analysis showed personal influence to be statistically significant amongst the divorcees compared to single women (p = 0.003). Copyright © 2013 SciRes. OPEN ACCESS 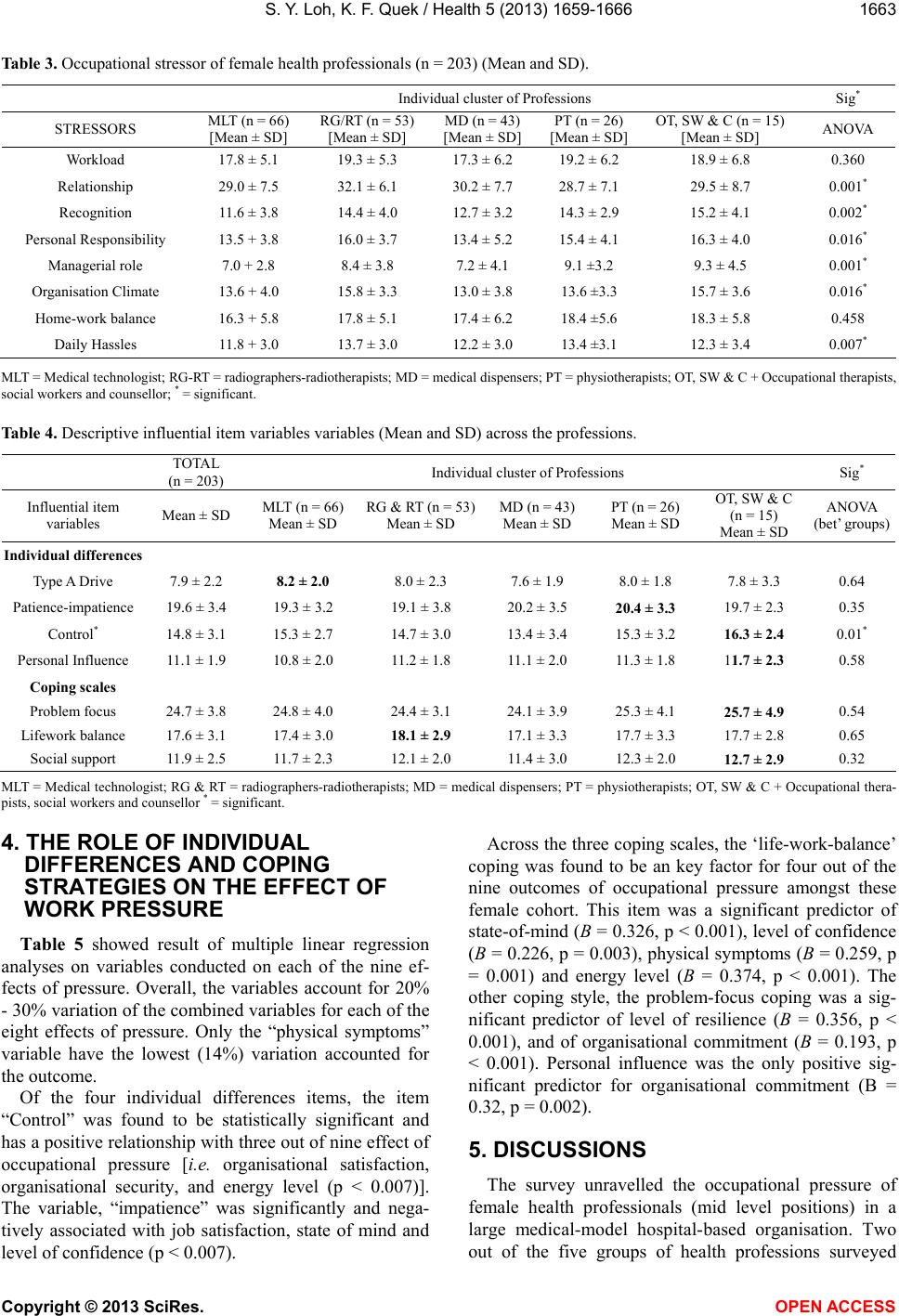 S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 1663 Table 3. Occupational stressor of female health professionals (n = 203) (Mean and SD). Individual cluster of Professions Sig* STRESSORS MLT (n = 66) [Mean ± SD] RG/RT (n = 53) [Mean ± SD] MD (n = 43) [Mean ± SD] PT (n = 26) [Mean ± SD] OT, SW & C (n = 15) [Mean ± SD] ANOVA Workload 17.8 ± 5.1 19.3 ± 5.3 17.3 ± 6.2 19.2 ± 6.2 18.9 ± 6.8 0.360 Relationship 29.0 ± 7.5 32.1 ± 6.1 30.2 ± 7.7 28.7 ± 7.1 29.5 ± 8.7 0.001* Recognition 11.6 ± 3.8 14.4 ± 4.0 12.7 ± 3.2 14.3 ± 2.9 15.2 ± 4.1 0.002* Personal Responsibility 13.5 + 3.8 16.0 ± 3.7 13.4 ± 5.2 15.4 ± 4.1 16.3 ± 4.0 0.016* Managerial role 7.0 + 2.8 8.4 ± 3.8 7.2 ± 4.1 9.1 ±3.2 9.3 ± 4.5 0.001* Organisation Climate 13.6 + 4.0 15.8 ± 3.3 13.0 ± 3.8 13.6 ±3.3 15.7 ± 3.6 0.016* Home-work balance 16.3 + 5.8 17.8 ± 5.1 17.4 ± 6.2 18.4 ±5.6 18.3 ± 5.8 0.458 Daily Hassles 11.8 + 3.0 13.7 ± 3.0 12.2 ± 3.0 13.4 ±3.1 12.3 ± 3.4 0.007* MLT = Medical technologist; RG-RT = radiographers-radiotherapists; MD = medical dispensers; PT = physiotherapists; OT, SW & C + Occupational therapists, social workers and counsellor; * = significant. Table 4. Descriptive influential item variables variables (Mean and SD) across the professions. TOTAL (n = 203) Individual cluster of Professions Sig* Influential item variables Mean ± SD MLT (n = 66) Mean ± SD RG & RT (n = 53) Mean ± SD MD (n = 43) Mean ± SD PT (n = 26) Mean ± SD OT, SW & C (n = 15) Mean ± SD ANOVA (bet’ groups) Individual differences Type A Drive 7.9 ± 2.2 8.2 ± 2.0 8.0 ± 2.3 7.6 ± 1.9 8.0 ± 1.8 7.8 ± 3.3 0.64 Patience-impatience 19.6 ± 3.4 19.3 ± 3.2 19.1 ± 3.8 20.2 ± 3.5 20.4 ± 3.3 19.7 ± 2.3 0.35 Control* 14.8 ± 3.1 15.3 ± 2.7 14.7 ± 3.0 13.4 ± 3.4 15.3 ± 3.2 16.3 ± 2.4 0.01* Personal Influence 11.1 ± 1.9 10.8 ± 2.0 11.2 ± 1.8 11.1 ± 2.0 11.3 ± 1.8 11.7 ± 2.3 0.58 Coping scales Problem focus 24.7 ± 3.8 24.8 ± 4.0 24.4 ± 3.1 24.1 ± 3.9 25.3 ± 4.1 25.7 ± 4.9 0.54 Lifework balance 17.6 ± 3.1 17.4 ± 3.0 18.1 ± 2.9 17.1 ± 3.3 17.7 ± 3.3 17.7 ± 2.8 0.65 Social support 11.9 ± 2.5 11.7 ± 2.3 12.1 ± 2.0 11.4 ± 3.0 12.3 ± 2.0 12.7 ± 2.9 0.32 MLT = Medical technologist; RG & RT = radiographers-radiotherapists; MD = medical dispensers; PT = physiotherapists; OT, SW & C + Occupational thera- pists, social workers and counsellor * = significant. 4. THE ROLE OF INDIVIDUAL DIFFERENCES AND COPING STRATEGIES ON THE EFFECT OF WORK PRESSURE Table 5 showed result of multiple linear regression analyses on variables conducted on each of the nine ef- fects of pressure. Overall, the variables account for 20% - 30% variation of the combined variables for each of the eight effects of pressure. Only the “physical symptoms” variable have the lowest (14%) variation accounted for the outcome. Of the four individual differences items, the item “Control” was found to be statistically significant and has a positive relationship with three out of nine effect of occupational pressure [i.e. organisational satisfaction, organisational security, and energy level (p < 0.007)]. The variable, “impatience” was significantly and nega- tively associated with job satisfaction, state of mind and level of confidence (p < 0.007). Across the three coping scales, the ‘life-work-balance’ coping was found to be an key factor for four out of the nine outcomes of occupational pressure amongst these female cohort. This item was a significant predictor of state-of-mind (B = 0.326, p < 0.001), level of confidence (B = 0.226, p = 0.003), physical symptoms (B = 0.259, p = 0.001) and energy level (B = 0.374, p < 0.001). The other coping style, the problem-focus coping was a sig- nificant predictor of level of resilience (B = 0.356, p < 0.001), and of organisational commitment (B = 0.193, p < 0.001). Personal influence was the only positive sig- nificant predictor for organisational commitment (B = 0.32, p = 0.002). 5. DISCUSSIONS The survey unravelled the occupational pressure of female health professionals (mid level positions) in a large medical-model hospital-based organisation. Two out of the five groups of health professions surveyed Copyright © 2013 SciRes. OPEN ACCES S 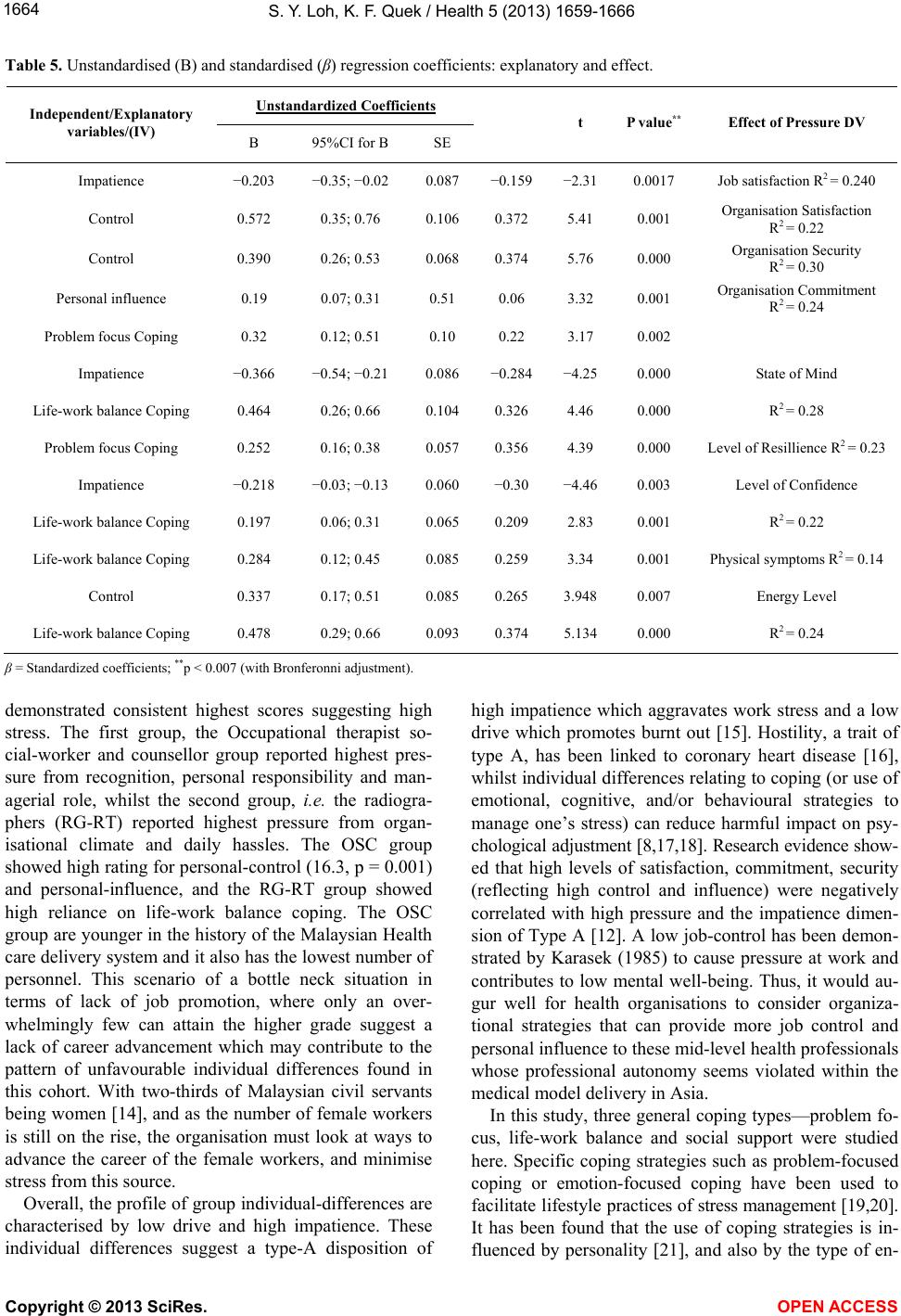 S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 1664 Table 5. Unstandardised (B) and standardised (β) regression coefficients: explanatory and effect. Unstandardized Coefficients Independent/Explanatory variables/(IV) B 95%CI for B SE t P value** Effect of Pressure DV Impatience −0.203 −0.35; −0.02 0.087 −0.159 −2.31 0.0017 Job satisfaction R2 = 0.240 Control 0.572 0.35; 0.76 0.106 0.372 5.41 0.001 Organisation Satisfaction R2 = 0.22 Control 0.390 0.26; 0.53 0.068 0.374 5.76 0.000 Organisation Security R2 = 0.30 Personal influence 0.19 0.07; 0.31 0.51 0.06 3.32 0.001 Organisation Commitment R2 = 0.24 Problem focus Coping 0.32 0.12; 0.51 0.10 0.22 3.17 0.002 Impatience −0.366 −0.54; −0.21 0.086 −0.284 −4.25 0.000 State of Mind Life-work balance Coping 0.464 0.26; 0.66 0.104 0.326 4.46 0.000 R2 = 0.28 Problem focus Coping 0.252 0.16; 0.38 0.057 0.356 4.39 0.000 Level of Resillience R2 = 0.23 Impatience −0.218 −0.03; −0.13 0.060 −0.30 −4.46 0.003 Level of Confidence Life-work balance Coping 0.197 0.06; 0.31 0.065 0.209 2.83 0.001 R2 = 0.22 Life-work balance Coping 0.284 0.12; 0.45 0.085 0.259 3.34 0.001 Physical symptoms R2 = 0.14 Control 0.337 0.17; 0.51 0.085 0.265 3.948 0.007 Energy Level Life-work balance Coping 0.478 0.29; 0.66 0.093 0.374 5.134 0.000 R2 = 0.24 β = Standardized coefficients; **p < 0.007 (with Bronferonni adjustment). demonstrated consistent highest scores suggesting high stress. The first group, the Occupational therapist so- cial-worker and counsellor group reported highest pres- sure from recognition, personal responsibility and man- agerial role, whilst the second group, i.e. the radiogra- phers (RG-RT) reported highest pressure from organ- isational climate and daily hassles. The OSC group showed high rating for personal-control (16.3, p = 0.001) and personal-influence, and the RG-RT group showed high reliance on life-work balance coping. The OSC group are younger in the history of the Malaysian Health care delivery system and it also has the lowest number of personnel. This scenario of a bottle neck situation in terms of lack of job promotion, where only an over- whelmingly few can attain the higher grade suggest a lack of career advancement which may contribute to the pattern of unfavourable individual differences found in this cohort. With two-thirds of Malaysian civil servants being women [14], and as the number of female workers is still on the rise, the organisation must look at ways to advance the career of the female workers, and minimise stress from this source. Overall, the profile of group individual-differences are characterised by low drive and high impatience. These individual differences suggest a type-A disposition of high impatience which aggravates work stress and a low drive which promotes burnt out [15]. Hostility, a trait of type A, has been linked to coronary heart disease [16], whilst individual differences relating to coping (or use of emotional, cognitive, and/or behavioural strategies to manage one’s stress) can reduce harmful impact on psy- chological adjustment [8,17,18]. Research evidence show- ed that high levels of satisfaction, commitment, security (reflecting high control and influence) were negatively correlated with high pressure and the impatience dimen- sion of Type A [12]. A low job-control has been demon- strated by Karasek (1985) to cause pressure at work and contributes to low mental well-being. Thus, it would au- gur well for health organisations to consider organiza- tional strategies that can provide more job control and personal influence to these mid-level health professionals whose professional autonomy seems violated within the medical model delivery in Asia. In this study, three general coping types—problem fo- cus, life-work balance and social support were studied here. Specific coping strategies such as problem-focused coping or emotion-focused coping have been used to facilitate lifestyle practices of stress management [19,20]. It has been found that the use of coping strategies is in- fluenced by personality [21], and also by the type of en- Copyright © 2013 SciRes. OPEN ACCESS  S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 1665 vironment [22]. This study found that the female profes- sionals rely a lot on life-work balance coping which has a significant positive relationship with four out of the nine outcomes of work pressure. This study found that women professionals with low confidence, low resilience and low energy level are in- clined to resort to high social support strategy. Studies have showed that in self perceived stress is an indicator of psychosocial impairment at the workplace [7]. Also, in times of stress, women tend and befriend rather than fight or flight [23], whereby the use of social support is a critical coping resource for women [24]. Evidence sug- gest that social support with qualities of hardiness (commitment and control) can moderate the relationship between stress and depression [25]. Drawing from recent finding on women and stress, researchers suggest that women displayed a “tend and befriend” rather than “fight-or-flight” behaviour [26,27]. This finding have implications on intervention program to ensure that skills on getting support and maintaining support should be incorporated into the stress management program par- ticularly for women with low confidence, low resilience and low energy level. A strategy to increase organisa- tional commitments is to improve the personal influence of these women health professionals; whilst to increase organisational satisfaction, organisational security and energy levels, women perceived themselves as having high job control over their work do perform better. There is an unfavourable pattern of individual differ- ences (characterized by low-drive or low desires to suc- ceed and achieve results), and this does not augur well for the occupational performance of the workers nor of the hospital organization. Job reorganizations involving increasing employee influence and increased job-control were less frequently practice for women and older work- ers [28], but may be so pertinent in Asian health care organisations, a sector largely led by male medical clini- cians who are predominantly, the hierarchical and auto- cratic decision makers. Lastly, this paper raises other interesting questions re- garding items of stress response, such as social support which showed a tendency towards significance item pressure for four outcomes of pressure. The critical query remains, do women fair better with social support be- cause of the tend-and-befriend stress response [23], since it has a negative relationship to four of the outcomes of pressure. As more and more women today need to bal- ance home and work roles, rehabilitation strategies should be put in place to ameliorate women stressed at work, and to identify which subgroup are most vulner- able in order to provide preventive strategies? The find- ing support the view that individual differences play a role in the function of job control [28,29], although the role of self efficacy and its relationship to the de- mands-control model needs to be further studied. Future studies should look at comparison with males staff even thought there are relatively fewer males in this mid management jobs. It would also be interesting to do mul- tisite studies on various hospitals to determine if stress is significantly different. 6. CONCLUSION Occupational pressure may be a characteristic burden in the middle management positions that needs to incor- porate strategies directed at individuals, or at the organi- sation as a whole. Individual differences (particularly the level of perceived job-control) and the use of coping strategies (particularly life-work balance) were signifi- cant items of occupational pressure of female health professionals. The findings suggest that individual dif- ference act as key correlate to work pressure, with an unfavourable pattern of individual-differences found in these middle management health professionals. Regular audit of Occupational Pressure should be set up so that any evaluation can be carried out immediately or annu- ally for detecting, monitoring and intervening occupa- tional pressure of these middle management health workers. A comprehensive understanding of the transac- tional process of stress is needed to understand the spe- cific pressure of female health employees within the healthcare delivery system, in order to implement user- friendly policy to enhance occupational and organisa- tional performance and wellbeing at work REFERENCES [1] Vaez, M., Rylander, G., Nygren, A., Asberg, M. and Alex- anderson, K. (2007) Sickness absence and disability pen- sion in a cohort of employees initially on long-term sick leave due to psychiatric disorders in Sweden. Social Psy- chiatry and Psychiatric Epidemiology, 42, 381-388. http://dx.doi.org/10.1007/s00127-007-0189-9 [2] Tennant, C. (2001) Work-related stress and depressive disorders. Journal of Psychosomatic Research, 51, 697- 704. http://dx.doi.org/10.1016/S0022-3999(01)00255-0 [3] Bartolomucci, A. and Leopardi, R. (2009) Stress and depression: Preclinical research and clinical implications. PLoS ONE, 4, e4265. http://dx.doi.org/10.1371/journal.pone.0004265 [4] WHO (2005) Preventing chronic diseases: A vital invest- ment. World Health Organisation, Geneva. |http://www.who.int/chp/chronic_disease_report/full_repo rt.pdf; [5] Mathers, C. and Loncar, D. (2006) Projections of global mortality and burden of disease from 2002 to 2030. PLoS Medicine, 3, 2011-2030. http://dx.doi.org/10.1371/journal.pmed.0030442 [6] Lu, L., Cooper, C., Kao, S. and Zhou, Y. (2003) Work stress, control beliefs and well-being in Greater China— Copyright © 2013 SciRes. OPEN ACCES S  S. Y. Loh, K. F. Quek / Health 5 (2013) 1659-1666 Copyright © 2013 SciRes. OPEN ACCES S 1666 An exploration of sub-cultural differences between the PRC and Taiwan. Journal of Managerial Psychology, 18, 479-510. http://dx.doi.org/10.1108/02683940310494359 [7] Limm, H., Angerer, P., Heinmueller, M., Marten-Mittag, B., Nater, U. and Guendel, H. (2010) Self-perceived stress reactivity is an indicator of psychosocial impair- ment at the workplace. BMC Public Health, 10, 252. [8] Lazarus, R.S. and Cohen, J.B. (1977) Environmental stress. Plenum, New York. [9] Fotinatos-Ventouratos, R. and Cooper, C. (2005) The role of gender and social class in work stress. Journal of Man- agerial Psychology, 20, 14-23. http://dx.doi.org/10.1108/02683940510571612 [10] Rydmark, I., Wahlberg, K., Ghatan, P., Modell, S., Ny- gren, A., et al. (2006) Neuroendocrine, cognitive and structural imaging characteristics of women on longterm sickleave with job stress-induced depression. Biological Psychiatry, 60, 867-873. http://dx.doi.org/10.1016/j.biopsych.2006.04.029 [11] Comish, R., Daboval, J. and Swindle, B. (1994) Manag- ing stress in the workplace. The National Public Accoun- tant, 39, 24-27. [12] William, S. and Cooper, C. (1998) Measuring occupa- tional pressure: Development of the pressure management indicator. Journal of Occupational Health Psychology, 3, 306-321. http://dx.doi.org/10.1037/1076-8998.3.4.306 [13] Loh, S.Y. (2004) Reliability and validity of the pressure management inventory in a Malaysian population. Medi- cal Journal Malaysia, 59, 199. [14] Singh, S. (1999) Women power rising in civil service. New Straits Time, Malaysia. NST Press, Kuala Lumpur, 1. [15] Keinan, G. and Melamed, S. (1987) Personality charac- teristics and proneness to burnout: A study among inter- nists. Stress Medicine, 3, 307-315. http://dx.doi.org/10.1002/smi.2460030412 [16] Roseman, R. (1978) The interview method of assessment of the coronary-prone behavior pattern. Springer-Verlag, New York. [17] Lazarus, R. (1993) Coping theory and research: Past, pre- sent, and future. Psychosomatic Medicine, 55, 234-247. [18] Lazarus, R. (2000) Toward better research on stress and coping. American Psychologist, 55, 665-673. http://dx.doi.org/10.1037/0003-066X.55.6.665 [19] Glanz, K., Rimer, B. and Sharyn, S. (2005) Theory at a glance: A guide for health promotion practice. 2nd Edi- tion, United States National Cancer Institute, New York. [20] Glanz, K., Rimer, B. and Lewis, F. (2002) Health behav- ior and health education. Theory, research and practice. Wiley & Sons, San Fransisco. [21] Bolger, N. (1990) Coping as a personality process: A pro- spective study. Journal of Personality and Social Psy- chology, 59, 525-537. http://dx.doi.org/10.1037/0022-3514.59.3.525 [22] Mattlin, J., Wethington, E. and Kessler, R.C. (1990) Situ- ational determinants of coping and coping effectiveness. Journal of Health and Social Behavior, 31, 103-122. http://dx.doi.org/10.2307/2137048 [23] Taylor, S.E., Klein, L.C., Lewis, B.P., Gruenewald, T.L., Gurung, R. and Updegraff, J. (2000) Biobehavioral re- sponses to stress in females: Tend-and-befriend, not fight- or-flight. Psychological Review, 107, 411-429. http://dx.doi.org/10.1037/0033-295X.107.3.411 [24] Greenglass, E. (2002) Work stress, coping and social support: Implications for women’s occupational well-be- ing. APA, Washington DC, 85-96. [25] Pengilly, J. and Dowd, E. (2000) Hardiness and social support as moderators of stress. Journal of Clinical Psy- chology, 56, 813-820 http://dx.doi.org/10.1002/(SICI)1097-4679(200006)56:6< 813::AID-JCLP10>3.0.CO;2-Q [26] Taylor, S., Klein, L., Lewis, B., Gruenewald, T., Gurung, R. and Updegraff, J. (2000) Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107, 441-429 http://dx.doi.org/10.1037/0033-295X.107.3.411 [27] Taylor, S., Klein, L., Lewis, B., Gruenewald, T., Gurung, R. and Updegraff, J. (2002) Sex differences in biobehav- ioral responses to threat: Reply to Geary and Flinn. Psy- chological Review, 109, 751-753. [28] Karasek, R. (1990) Lower health risk with increased job control among white collar workers. Journal of Organ- izational Behavior, 11, 171-185. http://dx.doi.org/10.1002/job.4030110302 [29] Karasek, R. (1979) Job demands, job decision latitude and mental strain. Administrative Science Quarterly, 24, 129-144. http://dx.doi.org/10.2307/2392498 [30] Loh, S.Y. (2004) Reliability and validity of the pressure management inventory in a Malaysian population. Medi- cal Journal of Malaysia, 59, 199-206.
|