Estimation of Physiologic Ability and Surgical Stress Scoring System Appraises Laparoscopy-Assisted and Open
Distal Gastrectomy in Treatment of Early Gastric Cancer
4
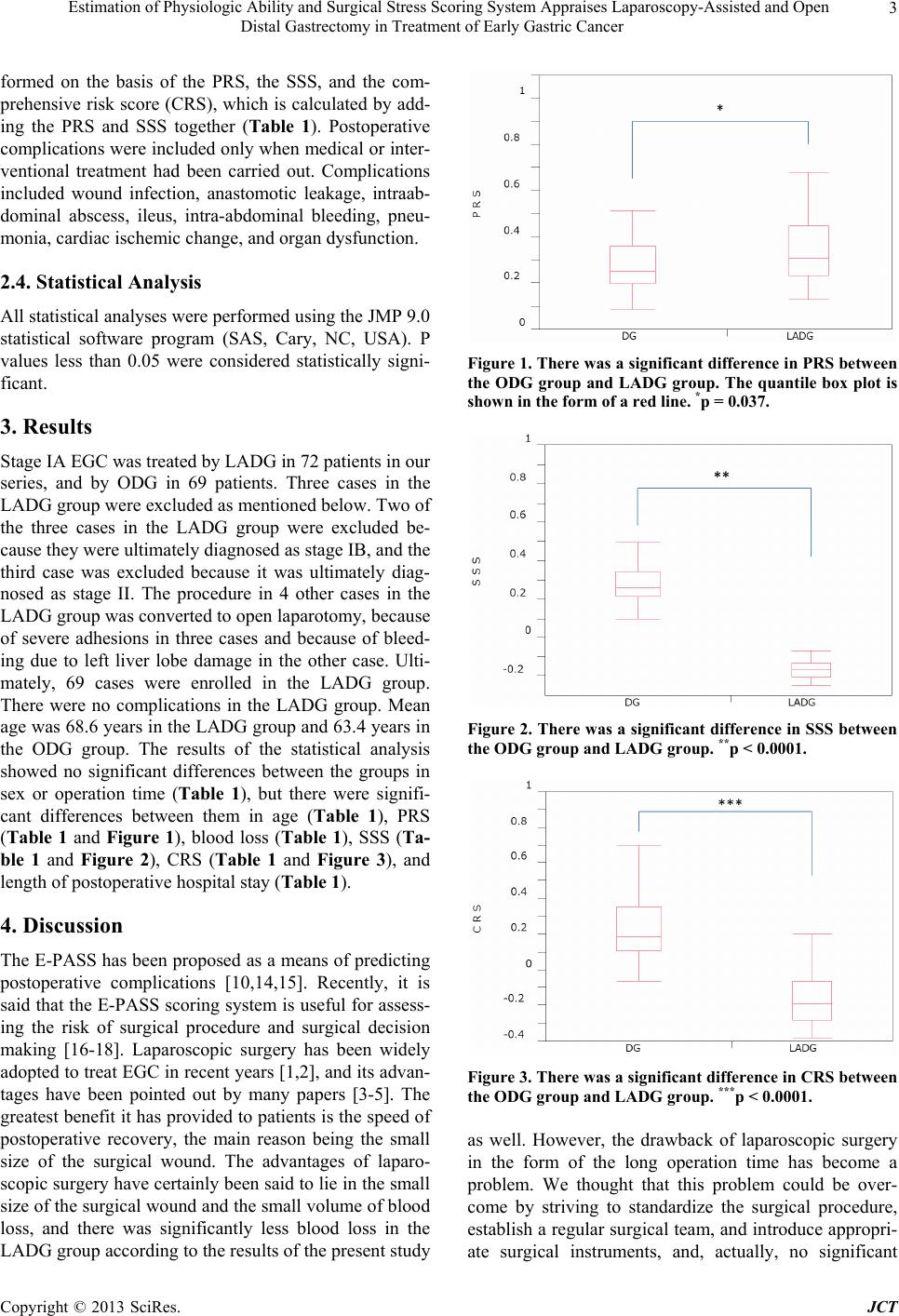
difference in operation time was observed in this study,
and as a result the SSS was significantly lower in the
LADG group. On the other hand, surgical risk cannot be
concluded to be decreased just because the PRS is lower,
because in elderly patients and patients who have high-
risk complications the operation sometimes ends in pal-
liative surgery rather than seeking curative surgery [16-
18]. In our present study mean age was higher in the
LADG group, and the PRS was higher. This means that
the preoperative risk was higher in the LADG group, but
since the aforementioned SSS was lower, the overall
evaluation in the form of the CRS was significantly
lower in the LADG group. This also seems to suggest
that laparoscopic surgery is more beneficial as a treat-
ment for EGC, even if there is some risk. A CRS of 1.0 is
said to be the threshold score for postoperative fatal com-
plications increasing [10]. In the present study the CRS
was significantly lower in the LADG group, but neither
score exceeded the threshold. Moreover, the postopera-
tive hospital stay was also significantly shorter in the
LADG group. Laparoscopic surgery has been described
as more beneficial in many papers [1-4], but few of them
have reported a comparative study in which the E-PASS
was used. In the present study we used the E-PASS to
perform an overall evaluation of the surgical treatment
for EGC, and based on the results we concluded that sur-
gical treatment in the LADG group was more beneficial.
This corroborates what has been widely claimed, and it is
a result that it was obtained according to an overall eval-
uation of the patients’ risk and the risk of surgery itself, a
different viewpoint from the past. Based on the above,
the E-PASS scoring system is useful for assessing the
risks of the operation procedure of EGC. We appreciate
that LADG is more feasible than ODG as a surgical
treatment for EGC.
REFERENCES
[1] S. Kitano, N. Shiraishi, I. Uyama, K. Sugihara, N. Ta-
nigawa and Japanese Laparoscopic Surgery Study Group,
“A Multicenter Study on Oncologic Outcome of Laparo-
scopic Gastrectomy for Early Cancer in Japan,” Annals of
Surgery, Vol. 245, No. 1, 2007, pp. 68-72.
http://dx.doi.org/10.1097/01.sla.0000225364.03133.f8
[2] H. Yano, et al., “The Usefulness of Laparoscopy-Assisted
Distal Gastrectomy in Comparison with That of Open
Distal Gastrectomy for Early Gastric Cancer,” Gastric
Cancer, Vol. 4, No. 2, 2001, pp. 93-97.
http://dx.doi.org/10.1007/PL00011730
[3] C. G. Huscher, et al., “Laparoscopic versus Open Subto-
tal Gastrectomy for Distal Gastric Cancer: Five-Year Re-
sults of a Randomized Prospective Trial,” Annals of Sur-
gery, Vol. 241, No. 2, 2001, pp. 232-237.
http://dx.doi.org/10.1097/01.sla.0000151892.35922.f2
[4] S. Kitano, et al., “A Randomized Controlled Trial Com-
paring Open vs Laparoscopy-Assisted Distal Gastrectomy
for the Treatment of Early Gastric Cancer: An Interim
Report,” Surgery, Vol. 131, Supplement 1, 2002, pp. S306-
S311. http://dx.doi.org/10.1067/msy.2002.120115
[5] K. J. Weber, Reyes CD, Gagner M, Divino CM, “Com-
parison of Laparoscopic and Open Gastrectomy for Ma-
lignant Disease,” Surgical Endoscopy, Vol. 17, No. 6,
2003, pp. 968-971.
http://dx.doi.org/10.1007/s00464-002-8738-5
[6] K. Yasuda, et al., “Rate of Detection of Lymph Node
Metastasis Is Correlated with the Depth of Submucosal
Invasion in Early Stage Gastric Carcinoma,” Cancer, Vol.
85, No. 10, 1999, pp. 2119-2123.
http://dx.doi.org/10.1002/(SICI)1097-0142(19990515)85:
10<2119::AID-CNCR4>3.0.CO;2-M
[7] S. Miura, et al., “Laparoscopy-Assisted Distal Gastrec-
tomy with Systemic Lymph Node Dissection: A Critical
Reappraisal from the Viewpoint of Lymph Node Re-
trieval,” Journal of the American College of Surgeons,
Vol. 198, No. 6, 2004, pp. 933-938.
http://dx.doi.org/10.1016/j.jamcollsurg.2004.01.021
[8] M. Fujiwara, et al., “Laparoscopy-Assisted Distal Gas-
trectomy with Systemic Lymph Node Dissection for
Early Gastric Carcinoma: A Review of 43 Cases,” Jour-
nal of the American College of Surgeons Vol. 196, No. 1,
2003, pp. 75-81.
http://dx.doi.org/10.1016/S1072-7515(02)01539-9
[9] K. Fujii, et al., “T Lymphocyte Subsets and Th1/Th2 Bal-
ance after Laparoscopy-Assisted Distal Gastrectomy,”
Surg Endosc, Vol. 17, No. 9, 2003, pp. 1440-1444.
http://dx.doi.org/10.1007/s00464-002-9149-3
[10] Y. Haga, et al., “Estimation of Physiologic Ability and
Surgical Stress (E-PASS) for a Surgical Audit in Elective
Digestive Surgery,” Surgery, Vol. 135, No. 6, 2004, pp.
586-594. http://dx.doi.org/10.1016/j.surg.2003.11.012
[11] D. Hashimoto, et al., “Can the Physiologic Ability and
Surgical Stress (E-PASS) Scoring System Predict Opera-
tive Morbidity after Distal Pancreatectomy?” Surgery
Today, Vol. 40, No. 7, 2004, pp. 632-637.
http://dx.doi.org/10.1007/s00595-009-4112-8
[12] Y. Haga, K. Ikejiri, H. Takeuchi, M. Ikenaga and Y.
Wada, “Value of General Surgical Risk Models for Pre-
dicting Postoperative Liver Failure and Mortality Fol-
lowing Liver Surgery,” Journal of Surgical Oncology,
Vol. 106, No. 7, 2012, pp. 898-904.
http://dx.doi.org/10.1002/jso.23160
[13] A. Kotera, Y. Haga, J. Kei, M. Okamoto and K. Seo,
“Evaluation of Estimation of Physiologic Ability and Sur-
gical Stress to Predict In-Hospital Mortality in Cardiac
Surgery,” Journal of Anesthesia, Vol. 25, No. 4, 2011, pp.
481-491. http://dx.doi.org/10.1007/s00540-011-1162-z
[14] V. M. Banz, P. Studer, D. Inderbitzin and D. Candinas,
“Validation of the Estimation of Physiologic Ability and
Surgical Stress (E-PASS) Score in Liver Surgery,” World
Journal of Surgery, Vol. 33, No. 6, 2009, pp. 1259-1265.
http://dx.doi.org/10.1007/s00268-009-9989-2
[15] Y. Oka, et al., “Usefulness of an Estimation of Physiol-
ogic Ability and Surgical Stress (E-PASS) Scoring Sys-
Copyright © 2013 SciRes. JCT