R. M. GORDON ET AL.
RC 3 is a measure of Cynicism and not hysterical personality
traits and therefore cannot be considered a substitute for the
MMPI-2 Hy scale.
In the next regression, model 1 contained Pd, with RC 4
added in model 2. For model 1, Pd accounted for 23.9% of the
variance in the OPO scale (R2 = .239). For model 2, this value
increased to .241 or 24.1% (R2 = .241), an increase of only .2%.
This change in R2 produced a non-significant F(1,94) = .249, p
= .619, indicating no predictive improvement with the inclusion
of RC 4.
The fifth regression entered Pa followed by RC 6. For the
first model with Pa entered alone, Pa accounted for 24.2% of
the variance in the OPO scale (R2 = .242). When RC 6 was
added in model 2, this value increased to .289 or 28.9%, pro-
ducing a significant F(1,94) = 6.228, p = .014, indicating im-
provement in predicting the OPO scale compared to using only
Pa. An examination of the beta values for these two predictors
in model 2 suggests, however, that Pa predicts more of the
variance in the OPO scale than does RC 6 (−.317 vs. −.279).
That is, while RC 6 predicts additional variance above and
beyond that predicted by Pa alone, the amount predicted is
small relative to Pa.
We next entered Pt in model 1 followed by RC 7 in model 2.
For model 1, Pt accounted for 18.2% of the variance in the
OPO scale (R2 = .182). For model 2, this value increased
to .184 or 18.4 (R2 = .184), an increase of only .2%. This
change in R2 produced a non-significant F(1,94) = .306, p
= .582, indicating no predictive improvement with the inclusion
of RC 7.
The next regression entered Sc in model 1 and RC 8 in
model 2. For model 1, Sc accounted for 28.3% of the variance
in the OPO scale (R2 = .283). For model 2, this value increased
to .320 or 32.0.1% (R2 = .320), an increase of 3.7%. This
change in R2 produced a significant F(1,94) = 5.036, p = .027,
indicating improvement in predicting in the OPO scale with the
inclusion of RC 8. However, the beta values indicate the Sc
predicts more of the variance in the OPO scale than does the
RC 8 scale (−.366 vs. −.253).
In the final regression, Ma was entered first, followed in
model 2 with RC 9. For model 1, Ma accounted for 11.3% of
the variance in the OPO scale (R2 = .113). Adding RC 9 in
model two increased this value to 24.1% (R2 = .241), producing
a significant F(1,94) = 15.809, p = .001. In this regression, the
beta values indicate that RC 9 in comparison to MA also pre-
dicts more of the variance in the OPO scale (−.476 vs. −.021).
In summary, 5 of the 8 RC scales (RC 1, RC 2, RC 6, RC 8,
and RC 9) added incremental validity to the MMPI-2 clinical
scales in predicting the level of severity in the Overall Person-
ality Organization (OPO) scale. However, an examination of
the beta values indicates that for 2 of the 5 RC scales (RC 6 and
RC 8) the amount of additional predicted variance is relatively
small in comparison to the amount predicted by their corre-
sponding MMPI-2 scales (Pa and SC). Taken together, in terms
of predictive utility, the results suggest that only 3 of the 8 or
37.5% of the RC scales contribute incrementally in predicting
the level of severity in the OPO scale, lending support to hy-
pothesis 3.
Discussion
This study looked at the clinical sensitivity of the MMPI-2
Clinical scales vs. the MMPI-RC scales with 98 clients from
forensic, disability and psychotherapy evaluations, representing
a wide range from psychotic, borderline to neurotic levels of
personality organization as measured by the Psychodiagnostic
Chart. Since the RC scales lack a diversity of items and subtly,
we hypothesized that the MMPI-2 Clinical scales would have
more clinical sensitivity than the RC scales at: 1) all levels of
psychopathology and 2) particularly at the less pathological
levels where subtlety is more of an issue in detecting psycho-
pathology.
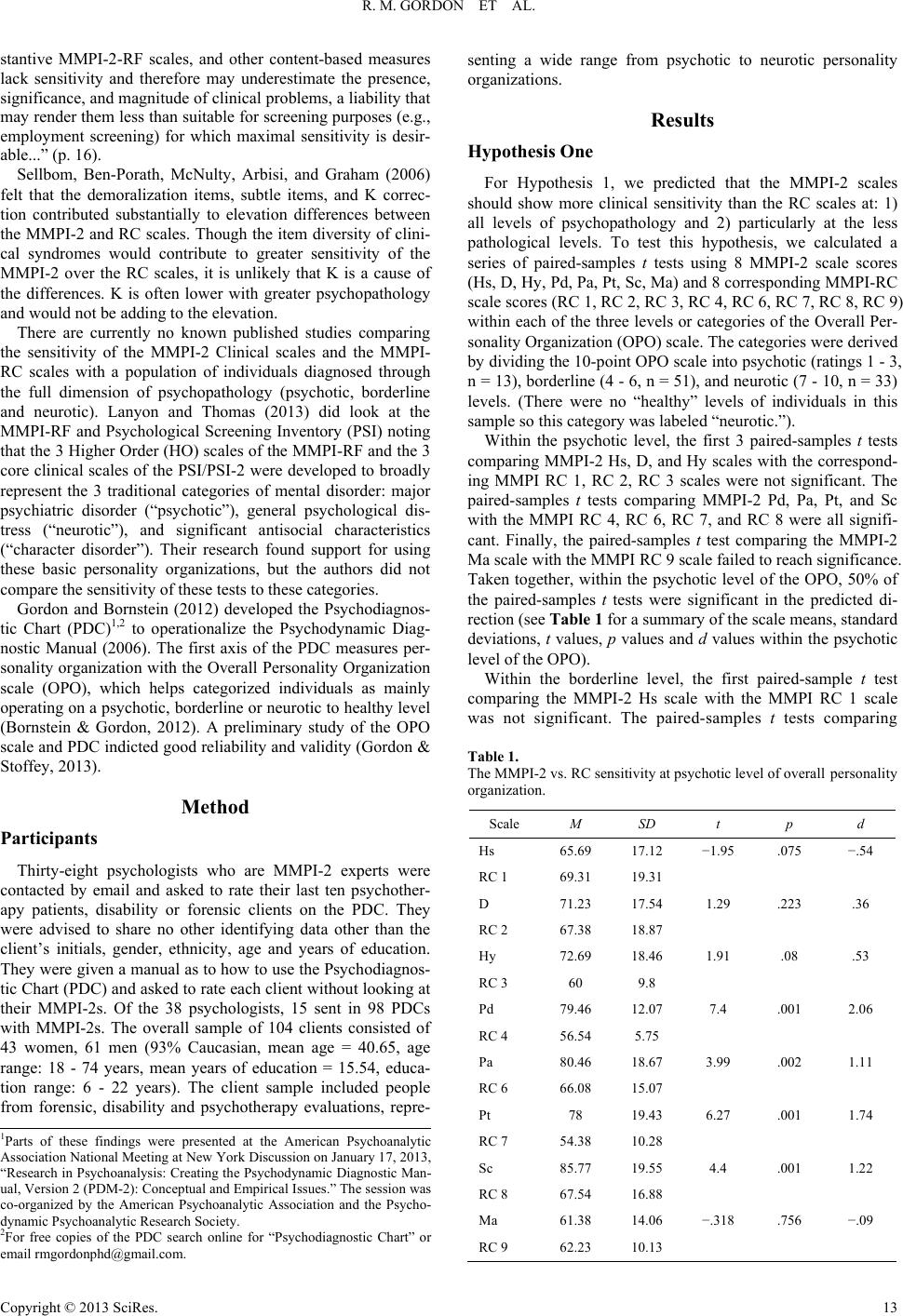
We found that the clients at the psychotic level of personality
organization as measured by the PDC, the MMPI-2 Hs, D, Hy
and Ma scales were not significantly different than the corre-
sponding MMPI RC 1, RC 2, RC 3, RC 9 scales. The MMPI-2
Pd, Pa, Pt, and Sc were all significantly higher than the corre-
sponding RC 4, RC 6, RC 7, and RC 8. Only 4 of the RC scales
reached clinical significance (T 65 or more), while 7 of the 8
MMPI 2 Clinical scales were T 65 or more for clients at the
psychotic level.
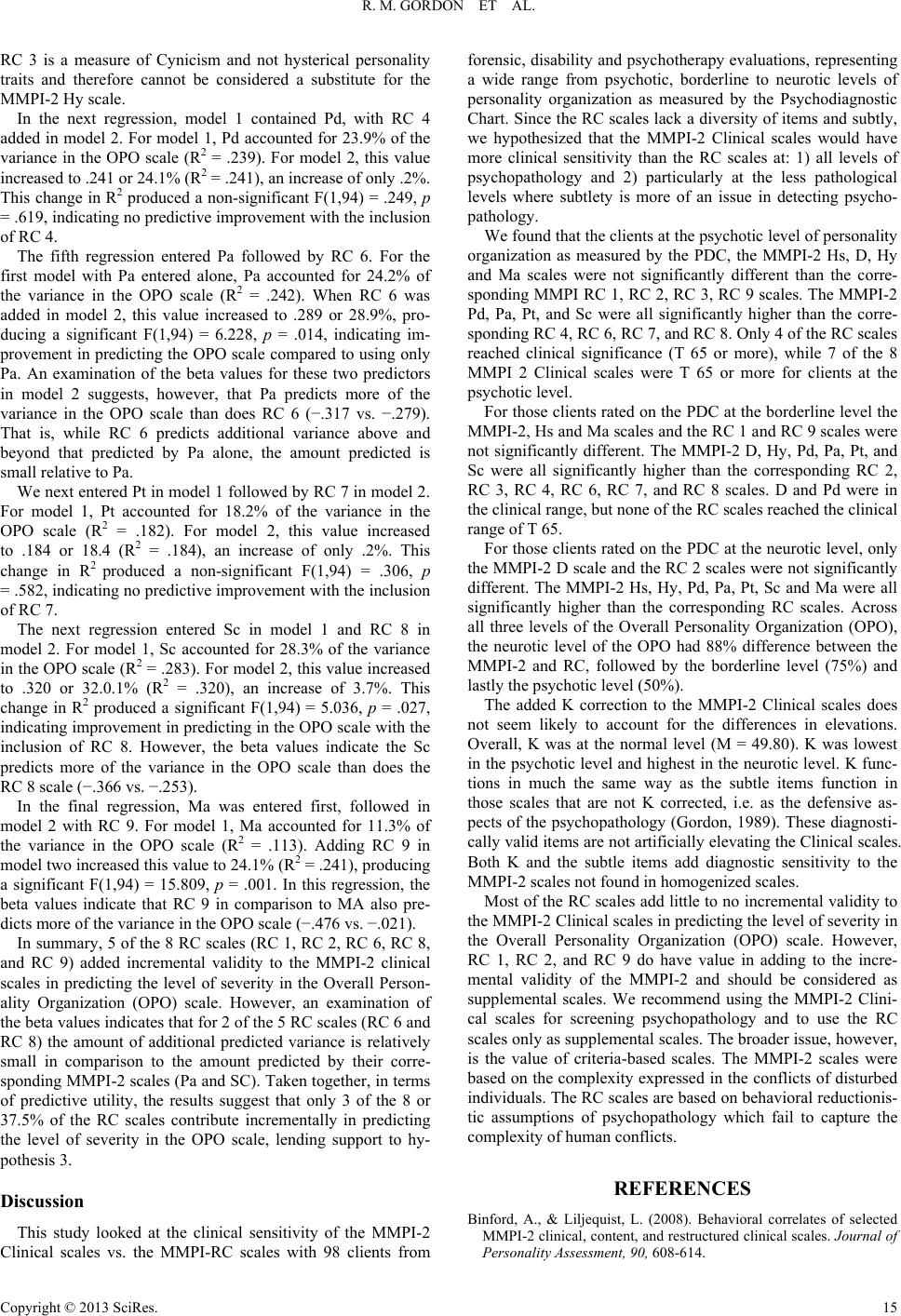
For those clients rated on the PDC at the borderline level the
MMPI-2, Hs and Ma scales and the RC 1 and RC 9 scales were
not significantly different. The MMPI-2 D, Hy, Pd, Pa, Pt, and
Sc were all significantly higher than the corresponding RC 2,
RC 3, RC 4, RC 6, RC 7, and RC 8 scales. D and Pd were in
the clinical range, but none of the RC scales reached the clinical
range of T 65.
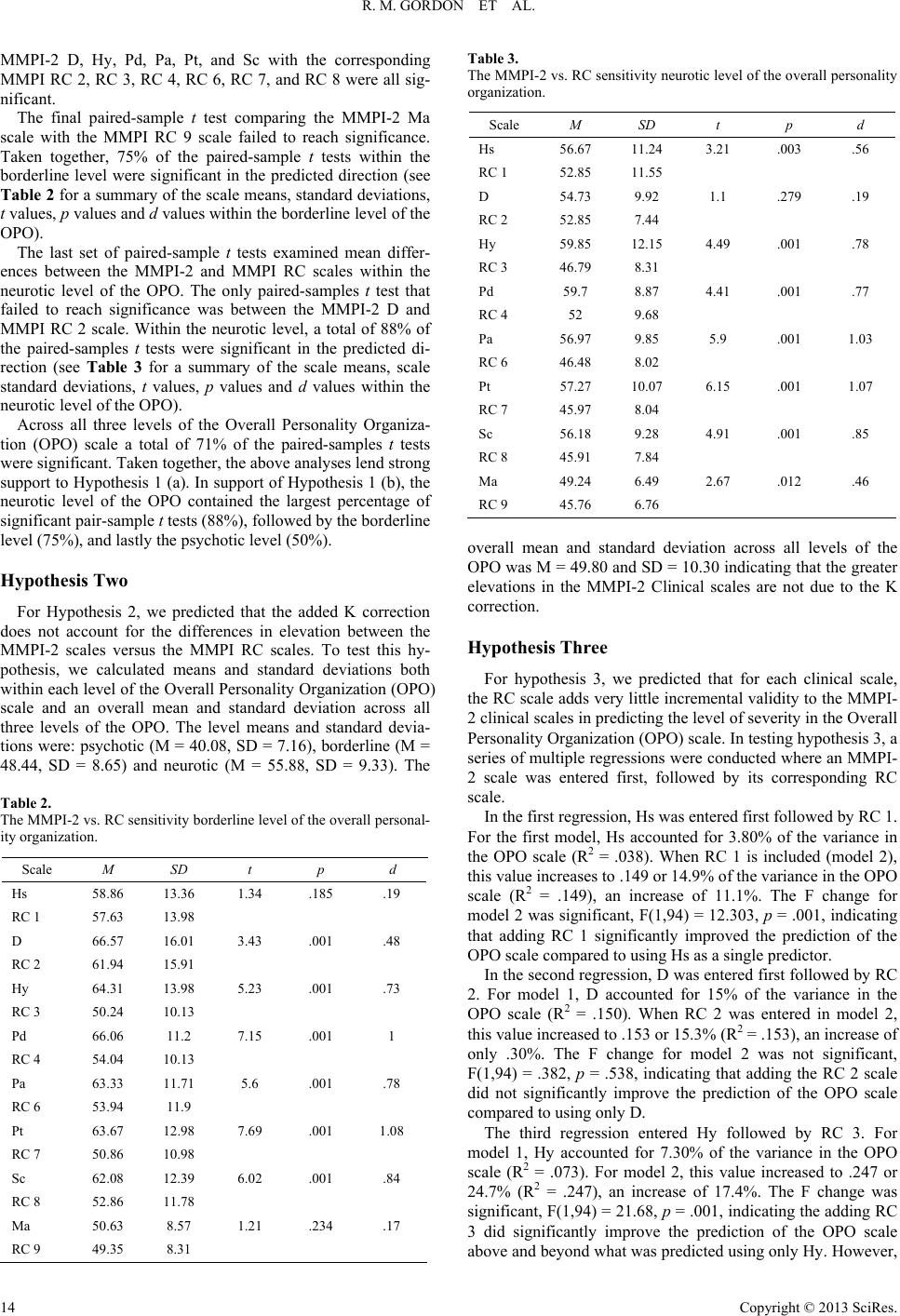
For those clients rated on the PDC at the neurotic level, only
the MMPI-2 D scale and the RC 2 scales were not significantly
different. The MMPI-2 Hs, Hy, Pd, Pa, Pt, Sc and Ma were all
significantly higher than the corresponding RC scales. Across
all three levels of the Overall Personality Organization (OPO),
the neurotic level of the OPO had 88% difference between the
MMPI-2 and RC, followed by the borderline level (75%) and
lastly the psychotic level (50%).
The added K correction to the MMPI-2 Clinical scales does
not seem likely to account for the differences in elevations.
Overall, K was at the normal level (M = 49.80). K was lowest
in the psychotic level and highest in the neurotic level. K func-
tions in much the same way as the subtle items function in
those scales that are not K corrected, i.e. as the defensive as-
pects of the psychopathology (Gordon, 1989). These diagnosti-
cally valid items are not artificially elevating the Clinical scales.
Both K and the subtle items add diagnostic sensitivity to the
MMPI-2 scales not found in homogenized scales.
Most of the RC scales add little to no incremental validity to
the MMPI-2 Clinical scales in predicting the level of severity in
the Overall Personality Organization (OPO) scale. However,
RC 1, RC 2, and RC 9 do have value in adding to the incre-
mental validity of the MMPI-2 and should be considered as
supplemental scales. We recommend using the MMPI-2 Clini-
cal scales for screening psychopathology and to use the RC
scales only as supplemental scales. The broader issue, however,
is the value of criteria-based scales. The MMPI-2 scales were
based on the complexity expressed in the conflicts of disturbed
individuals. The RC scales are based on behavioral reductionis-
tic assumptions of psychopathology which fail to capture the
complexity of human conflicts.
REFERENCES
Binford, A., & Liljequist, L. (2008). Behavioral correlates of selected
MMPI-2 clinical, content, and restructured clinical scales. Journal of
Personality Assessment, 90, 608-614.
Copyright © 2013 SciRes. 15