Vol.2, No.6, 375-376 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.26100
Laryngeal sarcoidosis—A case report*
Hemanth Kowdley Subrahmanyam#, P. Gana, R. J. Lee
Department of ENT-Head & Neck Surgery, Kettering General Hospital, Kettering, UK; #Corresponding Author: hks175@yahoo.co.uk
Received 19 July 2013; revised 5 August 2013; accepted 12 August 2013
Copyright © 2013 Hemanth Kowdley Subrahmanyam et al. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
ABSTRACT
Laryngeal sarcoidosis while involvement of the
vocal cords in the disease process is excep-
tionally rare. Involvement of the larynx is fre-
quently limited to the supraglottis that is rich in
lympho epithelial tissue and usually presents
with difficulty in breathing of varying severity.
We present a rare case of isolated sarcoidosis
involving the vocal cord in a patient with the
previous history of cutaneous sarcoidosis.
Keywords: Laryngeal Sarcoidosis
1. INTRODUCTION
Sarcoidosis is a chronic granulomatous disease involv-
ing in multiple organs in the body. Common sites of in-
volvement include lungs, hilar & mediastinal lymph
nodes, liver, eyes, skin, bone and the nervous system.
Diagnosis is based on a correlation between the clinical,
radiological and histological findings [1]. Supraglottic
involvement is a very common finding in the larynx.
True vocal cord involvement is a rarity. We present an
interesting case report who presented to us with chronic
cough as the only primary laryngeal symptom.
2. CASE REPORT
A 36-year-old female Caucasian smoker was referred
by respiratory physicians with complaints of hoarseness
for 8 months duration. She had received multiple courses
of antibiotics for a presumed URTI with no effect on her
hoarseness. There was no odynophagia or dysphagia. She
had no loss of weight or appetite. No history of voice
abuse was recorded. She was diagnosed with cutaneous
sarcoidosis in 2002. Her co-morbidities included hay
fever and Type II diabetes. Flexible nasolaryngoscopy
revealed left vocal cord and ventricular band thickening.
Her ACE level was elevated and CXR revealed bilateral
hilar lymph node enlargement signifying an active period
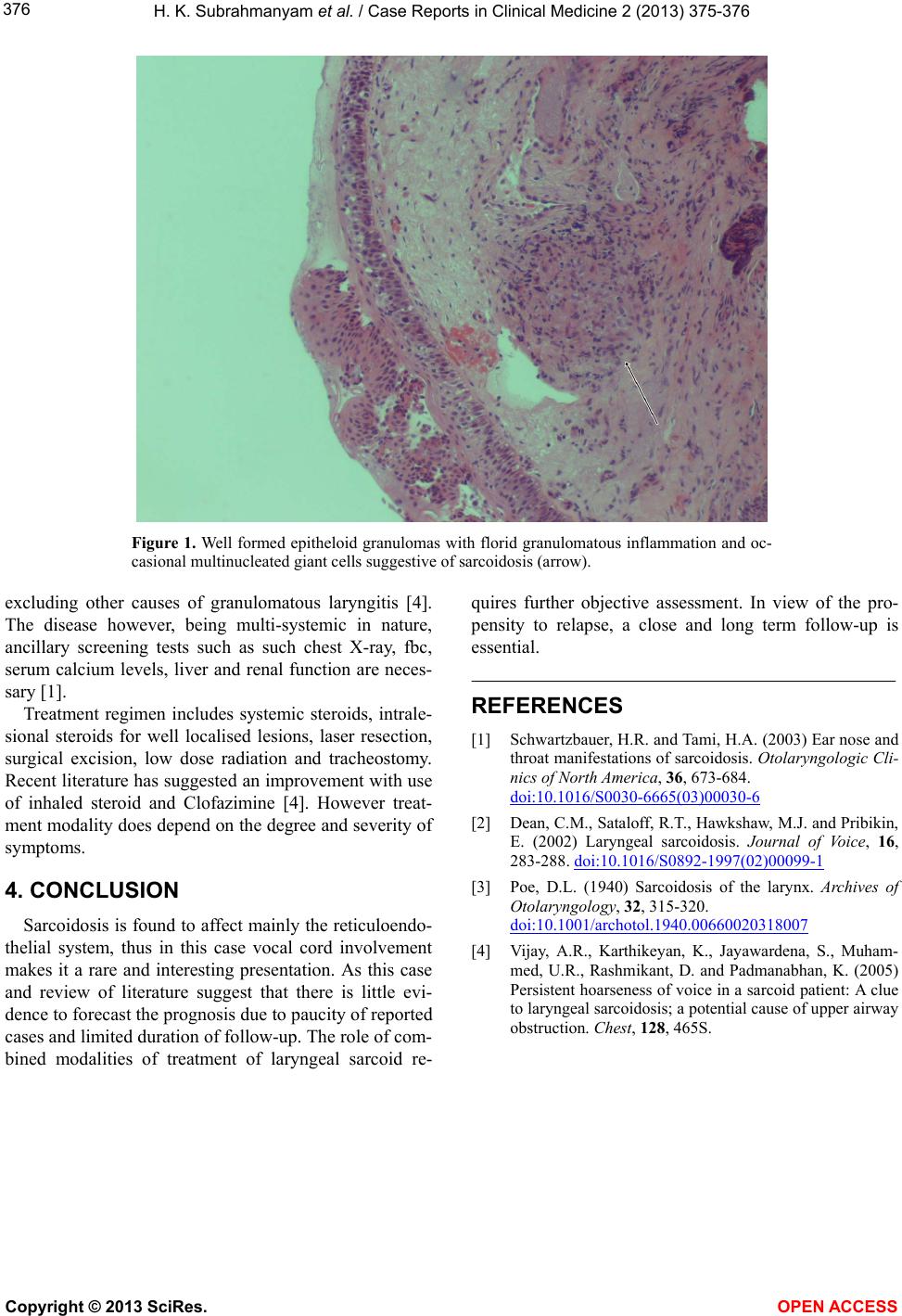
of her systemic sarcoidosis. Microlaryngoscopy and bi-
opsy suggested a narrow glottic area. Biopsy of the left
vocal cord revealed features consistent with Sarcoidosis
showing florid granulomatous inflammation alongside
well formed epitheloid granulomas and occasional mul-
tinucleated giant cells (Figure 1). There was no evidence
of caseous necrosis or malignancy. A diagnosis of laryn-
geal sarcoidosis was made. Treatment with inhalational
and systemic corticosteroids significantly improved her
condition. She has symptomatically remained stable and
on regular follow up.
3. DISCUSSION
The first confirmed case of laryngeal sarcoidosis was
by Poe in 1940 according to the literature [3]. Sarcoido-
sis is an idiopathic phenomenom characterised by non
caseating granulomas. Prevalence does vary in the ethnic
groups and is found to be 50 per 100,000 in Scandina-
vian countries and African Americans. It is a multi sys-
tem disorder which typically affects population between
20 and 40 years of age. Laryngeal sarcoidosis prevalence
is 0.5% to 8.3% in patients with a past history of sarcoi-
dosis [1]. It affects the supraglottis typically with isolated
evidence affecting the glottis. Interestingly it is theorized
that sarcoidosis affects the reticuloendothelial system and
hence vocal fold involvement is relatively uncommon
due to lack of lymphoid tissue [1,4].
Common s ymp toms at pre senta tion ar e hoar senes s and
stridor. Less commonly dysphagia, globus and cough
could be presenting features. Disease does tend to fluctu-
ate between active and latent periods [2] and therefore
calls for prolonged per iod of follow up. In the supraglot-
tis, epiglottis is the most common site of involvement
though any part of larynx could be affected [4]. Hoarse-
ness could be due to direct vocal fold involvement or as a
result of peripheral neuropathy affecting the vocal folds
and can usually be confirmed by laryngeal EMG [1].
Diagnosis is essentially established by histology demon-
trating non caeseous granulomatous inflammation thus s
*Conflict of interest: Nil.
Copyright © 2013 SciRes. OPEN A CCESS