Paper Menu >>
Journal Menu >>
 Surgical Science, 2011, 2, 8-12 doi:10.4236/ss.2011.21003 Published Online January 2011 (http://www.SciRP.org/journal/ss) Copyright © 2011 SciRes. SS Comparison of Histopathology of Transverse Carpal Ligament in Patients with Idiopathic Carpal Tunnel Syndrome and Hemodialysis Patients with Carpal Tunnel Syndrome Erdinc Civelek1, Tufan Cansever1, Serdar Kabatas1, Ebru Demiralay2, Emre Demircay3, Cem Comunoglu2, Cem Yilmaz4, Nur Altınors4 1Department of Neurosurgery, Baskent University Istanbul Hospital, Istanbul, Turkey 2Department of Pathology, Baskent University Istanbul Hospital, Istanbul, Turkey 3Department of Orthopedics, Baskent University Istanbul Hospital, Istanbul, Turkey 4Department of Neurosurgery, Baskent University, Ankara, Turkey E-mail: civsurgeon@yahoo.com Received August 14, 2010; revised September 15, 2010; accepted September 25, 2010 Abstract The aim of this paper is to point out the growing clinical importance of Carpal tunnel syndrome in patients on hemodialysis especially in aspect of the diagnosis, treatment and possible cause of the syndrome. Sixty patients with clinical diagnosis of Carpal Tunnel Syndrome was defined as the presence of two subjective symptoms (numbness, tingling in the median nerve distribution). The diagnosis was confirmed by electro- myography. The patients with rheumatoid arthritis, thalasemia and thyroid dysfunction and the patients hav- ing pain due to arthritis or tenosynovitis were excluded. Fifty patients with clinical diagnosis of idiopathic CTS and seven hemodialysis patients having CTS were analyzed. Of 50 patients (47 female, 3 male) with clinical diagnosis of idiopathic CTS, 11 patients (22%) were involved bilaterally, 25 patients (50%) were affected only on the right and 14 patients (28%) were symptomatic only on the left. Of 7 hemodialysis pa- tients (2 female, 5 male) with CTS, 1 patient (14%) was involved bilaterally (having two-sided A-V fistula), 4 patients (57%) were affected only on the right and 2 patients (28%) were symptomatic only on the left. There was significant correlation between the arteriovenous fistula and subsequent development of CTS. The all patients had fistulas in the affected side (5 of them were patent and 2 were occluded). In the relation be- tween the duration of hemodialysis and development of CTS, 4 patients were over 10 years of hemodialysis, 2 patients were between 5 to 9 years and only 1 patient was below 4 years of duration. Amyloid deposit was demonstrated in 4 of 7 operated hands in the hemodialysis group. When we compared the presence of amy- loid deposits in these groups, the difference between these two groups were found as statistically significant (p < 0.009). Although hemodialysis has no significant effect on development of fibrosis, the incidence of fibrosis was found as statistically significant in idiopathic carpal tunnel syndrome (p < 0.048). It is likely that there are numerous factors that may act either independently or in concert to potentiate the risk for develop- ing CTS in patients on long-term hemodialysis. Keywords: Carpal Tunnel Syndrome, Hemodialysis, Chronic Renal Failure 1. Introduction Neurological complications in patients with renal failure and hemodialysis are well-known. Among them periph- eral nerve involvement has been considered as a toxic polyneuropathy affecting mainly distal parts of the four extremities. Entrapment neuropathy such as Carpal tun- nel syndrome (CTS) could be completely curable with defined diagnosis and proper treatment [1,2]. CTS is divided into two large groups; idiopathic CTS and symptomatic CTS. Symptomatic CTS may range from due to traumas, anomalies, inflammation, neo- 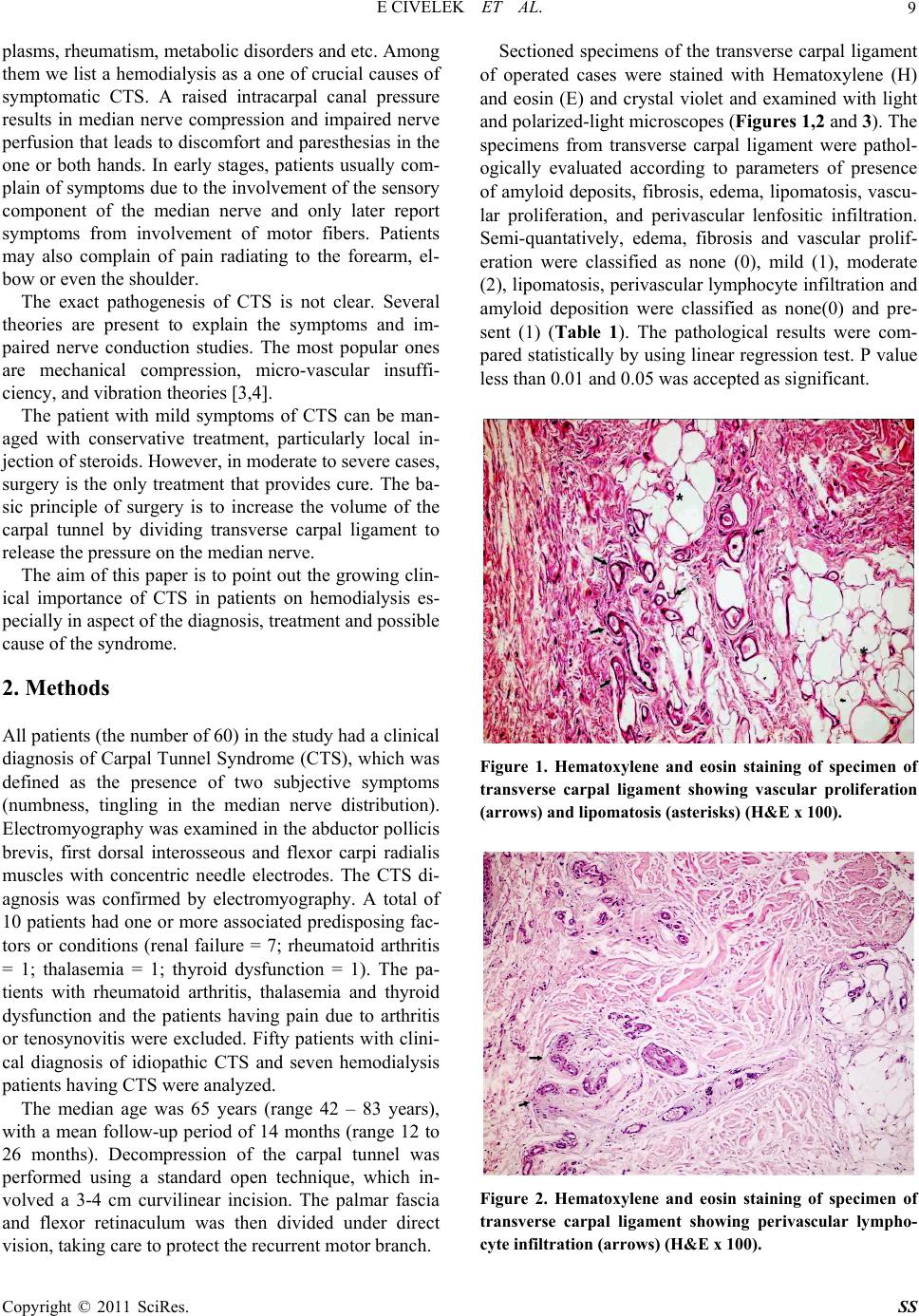 E CIVELEK ET AL. Copyright © 2011 SciRes. SS 9 plasms, rheumatism, metabolic disorders and etc. Among them we list a hemodialysis as a one of crucial causes of symptomatic CTS. A raised intracarpal canal pressure results in median nerve compression and impaired nerve perfusion that leads to discomfort and paresthesias in the one or both hands. In early stages, patients usually com- plain of symptoms due to the involvement of the sensory component of the median nerve and only later report symptoms from involvement of motor fibers. Patients may also complain of pain radiating to the forearm, el- bow or even the shoulder. The exact pathogenesis of CTS is not clear. Several theories are present to explain the symptoms and im- paired nerve conduction studies. The most popular ones are mechanical compression, micro-vascular insuffi- ciency, and vibration theories [3,4]. The patient with mild symptoms of CTS can be man- aged with conservative treatment, particularly local in- jection of steroids. However, in moderate to severe cases, surgery is the only treatment that provides cure. The ba- sic principle of surgery is to increase the volume of the carpal tunnel by dividing transverse carpal ligament to release the pressure on the median nerve. The aim of this paper is to point out the growing clin- ical importance of CTS in patients on hemodialysis es- pecially in aspect of the diagnosis, treatment and possible cause of the syndrome. 2. Methods All patients (the number of 60) in the study had a clinical diagnosis of Carpal Tunnel Syndrome (CTS), which was defined as the presence of two subjective symptoms (numbness, tingling in the median nerve distribution). Electromyography was examined in the abductor pollicis brevis, first dorsal interosseous and flexor carpi radialis muscles with concentric needle electrodes. The CTS di- agnosis was confirmed by electromyography. A total of 10 patients had one or more associated predisposing fac- tors or conditions (renal failure = 7; rheumatoid arthritis = 1; thalasemia = 1; thyroid dysfunction = 1). The pa- tients with rheumatoid arthritis, thalasemia and thyroid dysfunction and the patients having pain due to arthritis or tenosynovitis were excluded. Fifty patients with clini- cal diagnosis of idiopathic CTS and seven hemodialysis patients having CTS were analyzed. The median age was 65 years (range 42 – 83 years), with a mean follow-up period of 14 months (range 12 to 26 months). Decompression of the carpal tunnel was performed using a standard open technique, which in- volved a 3-4 cm curvilinear incision. The palmar fascia and flexor retinaculum was then divided under direct vision, taking care to protect the recurrent motor branch. Sectioned specimens of the transverse carpal ligament of operated cases were stained with Hematoxylene (H) and eosin (E) and crystal violet and examined with light and polarized-light microscopes (Figures 1,2 and 3). The specimens from transverse carpal ligament were pathol- ogically evaluated according to parameters of presence of amyloid deposits, fibrosis, edema, lipomatosis, vascu- lar proliferation, and perivascular lenfositic infiltration. Semi-quantatively, edema, fibrosis and vascular prolif- eration were classified as none (0), mild (1), moderate (2), lipomatosis, perivascular lymphocyte infiltration and amyloid deposition were classified as none(0) and pre- sent (1) (Table 1). The pathological results were com- pared statistically by using linear regression test. P value less than 0.01 and 0.05 was accepted as significant. Figure 1. Hematoxylene and eosin staining of specimen of transverse carpal ligament showing vascular proliferation (arrows) and lipomatosis (asterisks) (H&E x 100). Figure 2. Hematoxylene and eosin staining of specimen of transverse carpal ligament showing perivascular lympho- cyte infiltration (arrows) (H&E x 100). 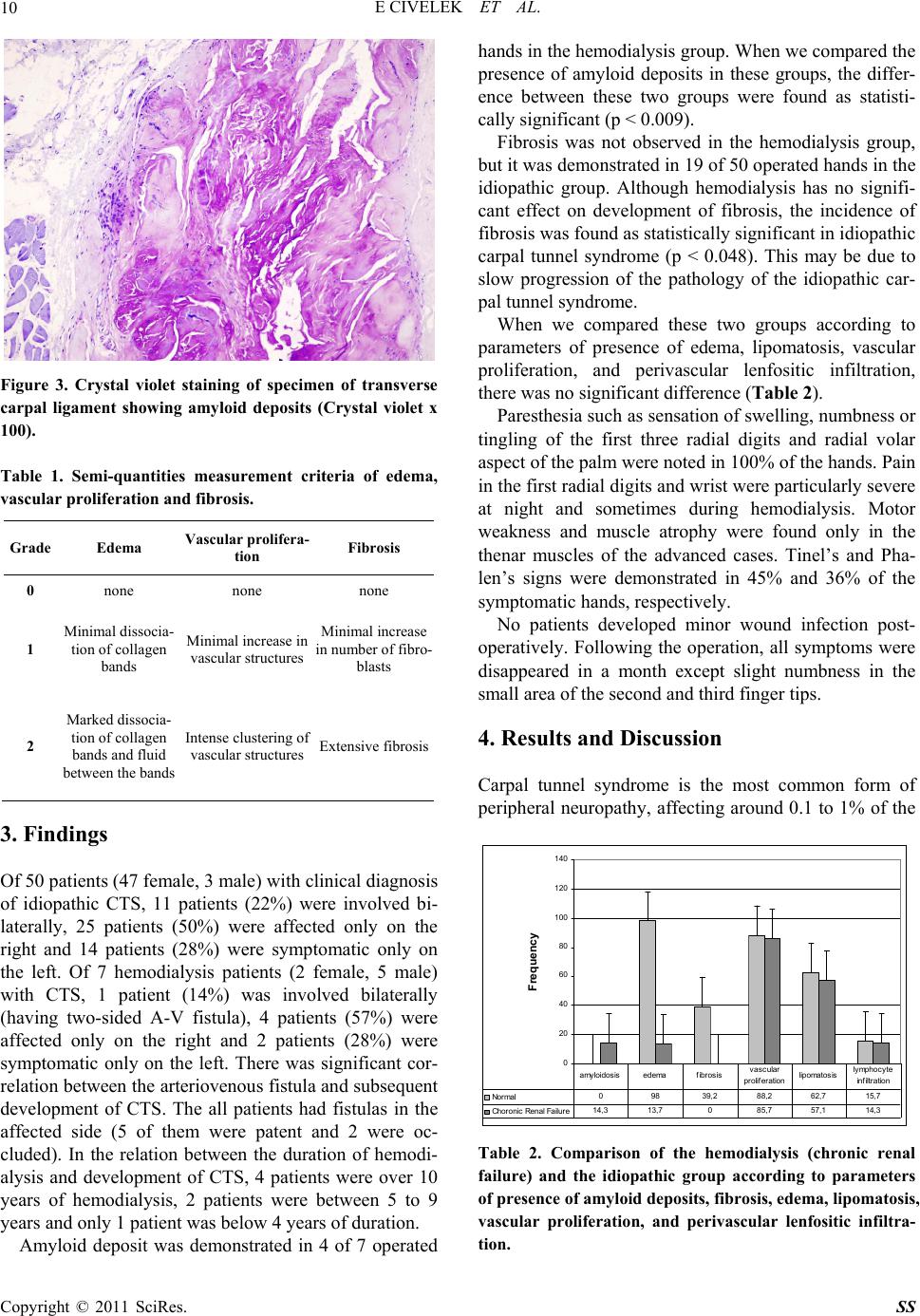 E CIVELEK ET AL. Copyright © 2011 SciRes. SS 10 Figure 3. Crystal violet staining of specimen of transverse carpal ligament showing amyloid deposits (Crystal violet x 100). Table 1. Semi-quantities measurement criteria of edema, vascular proliferation and fibrosis. Grade Edema Vascular prolifera- tion Fibrosis 0 none none none 1 Minimal dissocia- tion of collagen bands Minimal increase in vascular structures Minimal increase in number of fibro- blasts 2 Marked dissocia- tion of collagen bands and fluid between the bands Intense clustering of vascular structures Extensive fibrosis 3. Findings Of 50 patients (47 female, 3 male) with clinical diagnosis of idiopathic CTS, 11 patients (22%) were involved bi- laterally, 25 patients (50%) were affected only on the right and 14 patients (28%) were symptomatic only on the left. Of 7 hemodialysis patients (2 female, 5 male) with CTS, 1 patient (14%) was involved bilaterally (having two-sided A-V fistula), 4 patients (57%) were affected only on the right and 2 patients (28%) were symptomatic only on the left. There was significant cor- relation between the arteriovenous fistula and subsequent development of CTS. The all patients had fistulas in the affected side (5 of them were patent and 2 were oc- cluded). In the relation between the duration of hemodi- alysis and development of CTS, 4 patients were over 10 years of hemodialysis, 2 patients were between 5 to 9 years and only 1 patient was below 4 years of duration. Amyloid deposit was demonstrated in 4 of 7 operated hands in the hemodialysis group. When we compared the presence of amyloid deposits in these groups, the differ- ence between these two groups were found as statisti- cally significant (p < 0.009). Fibrosis was not observed in the hemodialysis group, but it was demonstrated in 19 of 50 operated hands in the idiopathic group. Although hemodialysis has no signifi- cant effect on development of fibrosis, the incidence of fibrosis was found as statistically significant in idiopathic carpal tunnel syndrome (p < 0.048). This may be due to slow progression of the pathology of the idiopathic car- pal tunnel syndrome. When we compared these two groups according to parameters of presence of edema, lipomatosis, vascular proliferation, and perivascular lenfositic infiltration, there was no significant difference (Table 2). Paresthesia such as sensation of swelling, numbness or tingling of the first three radial digits and radial volar aspect of the palm were noted in 100% of the hands. Pain in the first radial digits and wrist were particularly severe at night and sometimes during hemodialysis. Motor weakness and muscle atrophy were found only in the thenar muscles of the advanced cases. Tinel’s and Pha- len’s signs were demonstrated in 45% and 36% of the symptomatic hands, respectively. No patients developed minor wound infection post- operatively. Following the operation, all symptoms were disappeared in a month except slight numbness in the small area of the second and third finger tips. 4. Results and Discussion Carpal tunnel syndrome is the most common form of peripheral neuropathy, affecting around 0.1 to 1% of the 0 20 40 60 80 100 120 140 Frequency Normal 09839,288,2 62,715,7 Choronic Renal Failure14,313,7085,757,114,3 amyloidosis edemafibrosisvascular proliferation lipomatosis l ymphocyte infiltration Table 2. Comparison of the hemodialysis (chronic renal failure) and the idiopathic group according to parameters of presence of amyl oid deposits, fibrosis, edema, lipomatosis, vascular proliferation, and perivascular lenfositic infiltra- tion. 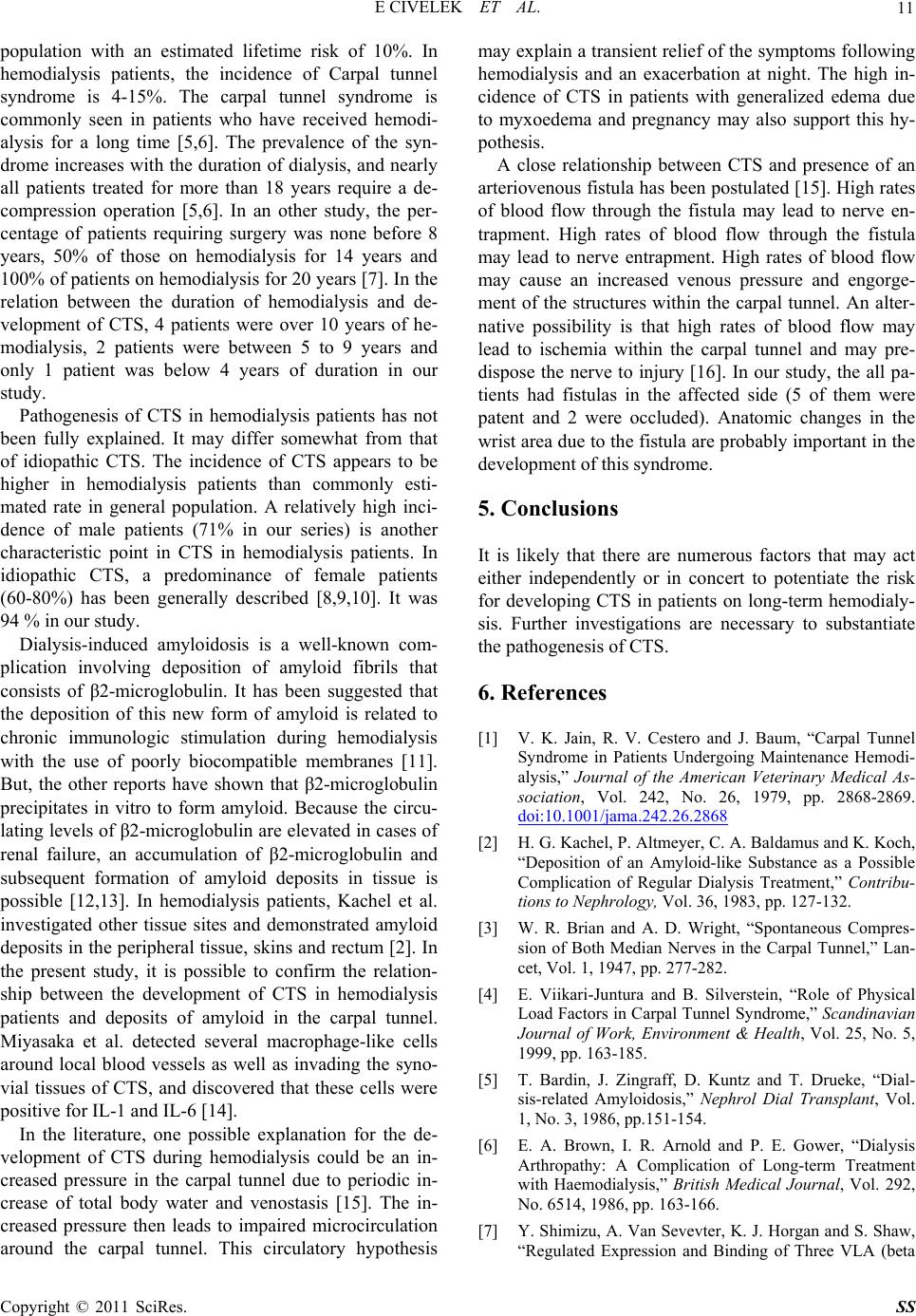 E CIVELEK ET AL. Copyright © 2011 SciRes. SS 11 population with an estimated lifetime risk of 10%. In hemodialysis patients, the incidence of Carpal tunnel syndrome is 4-15%. The carpal tunnel syndrome is commonly seen in patients who have received hemodi- alysis for a long time [5,6]. The prevalence of the syn- drome increases with the duration of dialysis, and nearly all patients treated for more than 18 years require a de- compression operation [5,6]. In an other study, the per- centage of patients requiring surgery was none before 8 years, 50% of those on hemodialysis for 14 years and 100% of patients on hemodialysis for 20 years [7]. In the relation between the duration of hemodialysis and de- velopment of CTS, 4 patients were over 10 years of he- modialysis, 2 patients were between 5 to 9 years and only 1 patient was below 4 years of duration in our study. Pathogenesis of CTS in hemodialysis patients has not been fully explained. It may differ somewhat from that of idiopathic CTS. The incidence of CTS appears to be higher in hemodialysis patients than commonly esti- mated rate in general population. A relatively high inci- dence of male patients (71% in our series) is another characteristic point in CTS in hemodialysis patients. In idiopathic CTS, a predominance of female patients (60-80%) has been generally described [8,9,10]. It was 94 % in our study. Dialysis-induced amyloidosis is a well-known com- plication involving deposition of amyloid fibrils that consists of β2-microglobulin. It has been suggested that the deposition of this new form of amyloid is related to chronic immunologic stimulation during hemodialysis with the use of poorly biocompatible membranes [11]. But, the other reports have shown that β2-microglobulin precipitates in vitro to form amyloid. Because the circu- lating levels of β2-microglobulin are elevated in cases of renal failure, an accumulation of β2-microglobulin and subsequent formation of amyloid deposits in tissue is possible [12,13]. In hemodialysis patients, Kachel et al. investigated other tissue sites and demonstrated amyloid deposits in the peripheral tissue, skins and rectum [2]. In the present study, it is possible to confirm the relation- ship between the development of CTS in hemodialysis patients and deposits of amyloid in the carpal tunnel. Miyasaka et al. detected several macrophage-like cells around local blood vessels as well as invading the syno- vial tissues of CTS, and discovered that these cells were positive for IL-1 and IL-6 [14]. In the literature, one possible explanation for the de- velopment of CTS during hemodialysis could be an in- creased pressure in the carpal tunnel due to periodic in- crease of total body water and venostasis [15]. The in- creased pressure then leads to impaired microcirculation around the carpal tunnel. This circulatory hypothesis may explain a transient relief of the symptoms following hemodialysis and an exacerbation at night. The high in- cidence of CTS in patients with generalized edema due to myxoedema and pregnancy may also support this hy- pothesis. A close relationship between CTS and presence of an arteriovenous fistula has been postulated [15]. High rates of blood flow through the fistula may lead to nerve en- trapment. High rates of blood flow through the fistula may lead to nerve entrapment. High rates of blood flow may cause an increased venous pressure and engorge- ment of the structures within the carpal tunnel. An alter- native possibility is that high rates of blood flow may lead to ischemia within the carpal tunnel and may pre- dispose the nerve to injury [16]. In our study, the all pa- tients had fistulas in the affected side (5 of them were patent and 2 were occluded). Anatomic changes in the wrist area due to the fistula are probably important in the development of this syndrome. 5. Conclusions It is likely that there are numerous factors that may act either independently or in concert to potentiate the risk for developing CTS in patients on long-term hemodialy- sis. Further investigations are necessary to substantiate the pathogenesis of CTS. 6. References [1] V. K. Jain, R. V. Cestero and J. Baum, “Carpal Tunnel Syndrome in Patients Undergoing Maintenance Hemodi- alysis,” Journal of the American Veterinary Medical As- sociation, Vol. 242, No. 26, 1979, pp. 2868-2869. doi:10.1001/jama.242.26.2868 [2] H. G. Kachel, P. Altmeyer, C. A. Baldamus and K. Koch, “Deposition of an Amyloid-like Substance as a Possible Complication of Regular Dialysis Treatment,” Contribu- tions to Nephrology, Vol. 36, 1983, pp. 127-132. [3] W. R. Brian and A. D. Wright, “Spontaneous Compres- sion of Both Median Nerves in the Carpal Tunnel,” Lan- cet, Vol. 1, 1947, pp. 277-282. [4] E. Viikari-Juntura and B. Silverstein, “Role of Physical Load Factors in Carpal Tunnel Syndrome,” Scandinavian Journal of Work, Environment & Health, Vol. 25, No. 5, 1999, pp. 163-185. [5] T. Bardin, J. Zingraff, D. Kuntz and T. Drueke, “Dial- sis-related Amyloidosis,” Nephrol Dial Transplant, Vol. 1, No. 3, 1986, pp.151-154. [6] E. A. Brown, I. R. Arnold and P. E. Gower, “Dialysis Arthropathy: A Complication of Long-term Treatment with Haemodialysis,” British Medical Journal, Vol. 292, No. 6514, 1986, pp. 163-166. [7] Y. Shimizu, A. Van Sevevter, K. J. Horgan and S. Shaw, “Regulated Expression and Binding of Three VLA (beta 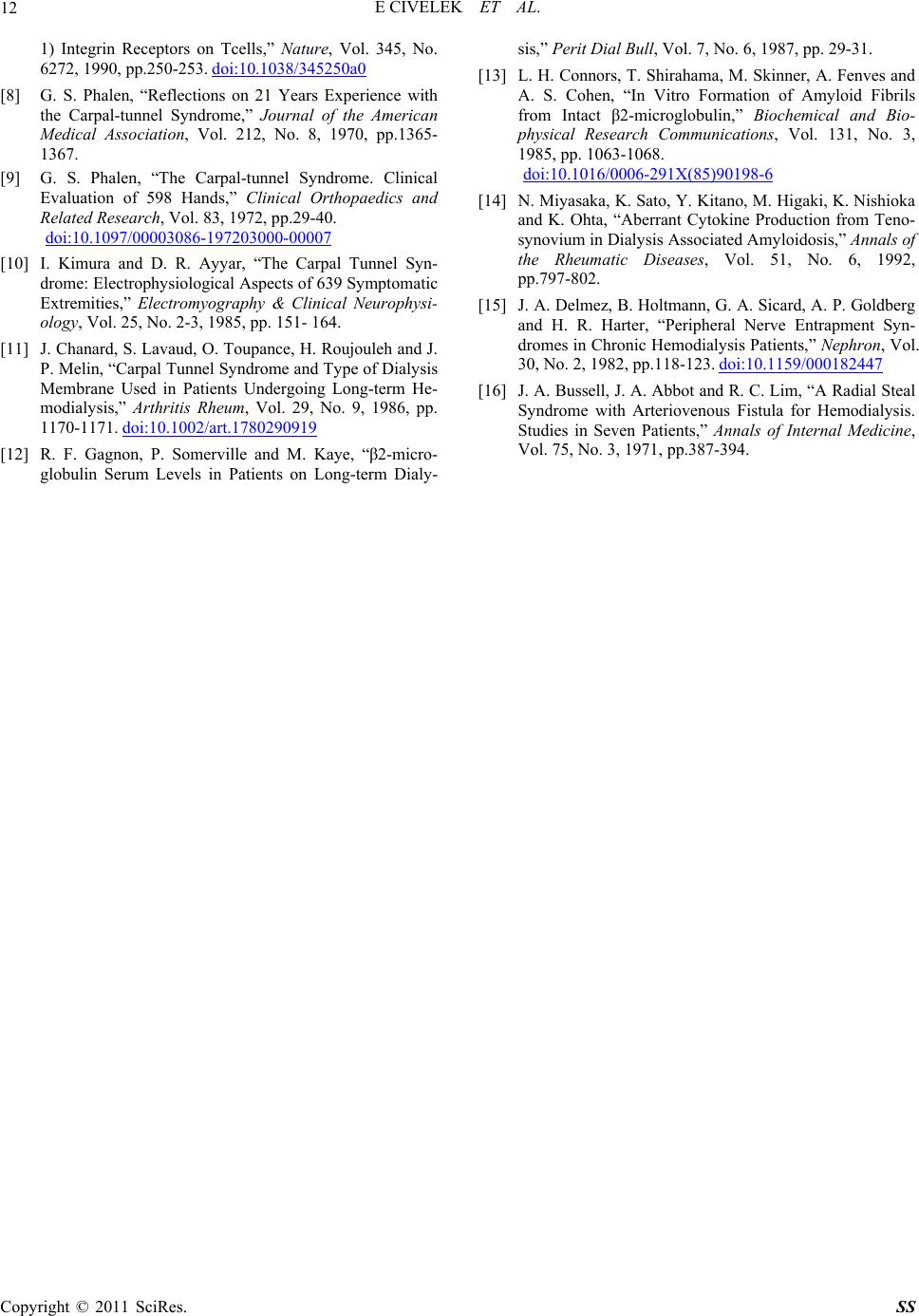 E CIVELEK ET AL. Copyright © 2011 SciRes. SS 12 1) Integrin Receptors on Tcells,” Nature, Vol. 345, No. 6272, 1990, pp.250-253. doi:10.1038/345250a0 [8] G. S. Phalen, “Reflections on 21 Years Experience with the Carpal-tunnel Syndrome,” Journal of the American Medical Association, Vol. 212, No. 8, 1970, pp.1365- 1367. [9] G. S. Phalen, “The Carpal-tunnel Syndrome. Clinical Evaluation of 598 Hands,” Clinical Orthopaedics and Related Re search, Vol. 83, 1972, pp.29-40. doi:10.1097/00003086-197203000-00007 [10] I. Kimura and D. R. Ayyar, “The Carpal Tunnel Syn- drome: Electrophysiological Aspects of 639 Symptomatic Extremities,” Electromyography & Clinical Neurophysi- ology, Vol. 25, No. 2-3, 1985, pp. 151- 164. [11] J. Chanard, S. Lavaud, O. Toupance, H. Roujouleh and J. P. Melin, “Carpal Tunnel Syndrome and Type of Dialysis Membrane Used in Patients Undergoing Long-term He- modialysis,” Arthritis Rheum, Vol. 29, No. 9, 1986, pp. 1170-1171. doi:10.1002/art.1780290919 [12] R. F. Gagnon, P. Somerville and M. Kaye, “β2-micro- globulin Serum Levels in Patients on Long-term Dialy- sis,” Perit Dial Bu l l, Vol. 7, No. 6, 1987, pp. 29-31. [13] L. H. Connors, T. Shirahama, M. Skinner, A. Fenves and A. S. Cohen, “In Vitro Formation of Amyloid Fibrils from Intact β2-microglobulin,” Biochemical and Bio- physical Research Communications, Vol. 131, No. 3, 1985, pp. 1063-1068. doi:10.1016/0006-291X(85)90198-6 [14] N. Miyasaka, K. Sato, Y. Kitano, M. Higaki, K. Nishioka and K. Ohta, “Aberrant Cytokine Production from Teno- synovium in Dialysis Associated Amyloidosis,” Annals of the Rheumatic Diseases, Vol. 51, No. 6, 1992, pp.797-802. [15] J. A. Delmez, B. Holtmann, G. A. Sicard, A. P. Goldberg and H. R. Harter, “Peripheral Nerve Entrapment Syn- dromes in Chronic Hemodialysis Patients,” Nephron, Vol. 30, No. 2, 1982, pp.118-123. doi:10.1159/000182447 [16] J. A. Bussell, J. A. Abbot and R. C. Lim, “A Radial Steal Syndrome with Arteriovenous Fistula for Hemodialysis. Studies in Seven Patients,” Annals of Internal Medicine, Vol. 75, No. 3, 1971, pp.387-394. |