A. GULATI ET AL.
196
added. The suggested risk categories can be derived from
MERI as follows: MERI 0 = Normal; MERI 1 - 3 = Mild
disease; MERI 4 - 6 = Moderate disease; MERI 7 - 12 =
Severe disease.
Being in a developing country with limited economic
and human resources, an important objective of ear sur-
gery is not only to provide good listening to the individ-
ual, but also provide the same at affordable costs. Paucity
of resources and the fact that most patients in our country
present with severe MERI, the use of such costly tita-
nium prostheses becomes limited only to patients where
maximum benefit is expected. Therefore in such a sce-
nario planning, -ossicular, -reconstructions in any patient
undergoing Tympanomastoidectomy requires precise ju-
dgement and population-based studies for the effective
use of limited resources. But even after an extensive re-
view of literature, we found that similar studies are lack-
ing. This study compares the audiological improvement
in patients with moderate/severe MERI undergoing Tym-
panomastoidectomies (Canal Wall Up or Canal Wall
Down) and reconstruction using titan ium TORP or PORP.
We have used Spiggle and Theis titanium TORP and
PORP in this study for the ossicular reconstruction. Avai-
lable length for TORP varies from 7 mm to 3.5 mm, com-
pared to 3.5 mm to 0.5 mm for PORP.
2. Materials and Methods
A retrospective analysis was done for all the patients un-
dergoing tympanomastoidectomy with ossicular chain re-
construction from September 2009 to December 2011
(28 months). Patients of chronic otitis media with Cho-
lesteatoma or granulations with a purely conductive hear-
ing loss were included in the study. Those with history of
complications or have undergone previous ear surgeries
were excluded from the study. Of the total, complete fol-
low up with post operative audiological analysis was
available for 17 cases.
Data was analysed in terms of middle ear risk index,
surgical procedure being done (ICW or CWD), method
of reconstruction (TORP or PORP), single/2nd stage re-
construction, and compared with the audiological im-
provement. Pre operative as well as post operative Air-
Bone gap was calculated at 0.5, 1, 2 and 3 kHz in accor-
dance with the guidelines of American Academy of Oto-
laryngology—Head and Neck Surgery committee on
hearing and equilibrium for hearing evaluation [9].
All the surgeries were performed under General An-
aesthesia via Post aural approach by the same surgeon
(A.S). The MERI index, disease exten t and the condition
of middle ear mucosa were used as criteria by the oper-
ating surgeon intra operatively for deciding whether to
go for canal wall up or canal wall down surgery, and also
for deciding whether the reconstruction would be done as
a primary reconstruction or to subject the patient to a sec-
ond stage reconstruction. Depending on the ossicular sta-
tus, TORP or PORP were placed over the stapes foot-
plate or supra structure respectively. The size of the pros-
thesis was calculated using a measuring gauge. For
TORP, the length of the prostheses required was calcu-
lated from footplate of stapes while for PORP, the stapes
head was used as a reference. The upper limit was taken
till the facial ridge in case of CWD and till the an nulus in
case of ICW surgery for both the prostheses. A small
piece of conchal cartilage (0.3 mm thickness) was har-
vested in all the cases and placed over the prostheses.
3. Results
Of the 17 cases that fulfilled the inclusion criteria, 9 had
moderate MERI and 8 had severe MERI. 7 patients un-
derwent mastoidectomies with canal wall down, while 10
had intact canal wall surgery. 8 underwent reconstru ction
using PORP, whereas 9 cases underwent reconstruction
using TORP. 13 cases were taken up for disease removal
and reconstruction in single setting, whereas 4 cases were
taken up fo r 2 n d stage reconst ru ct ion (Table 1).
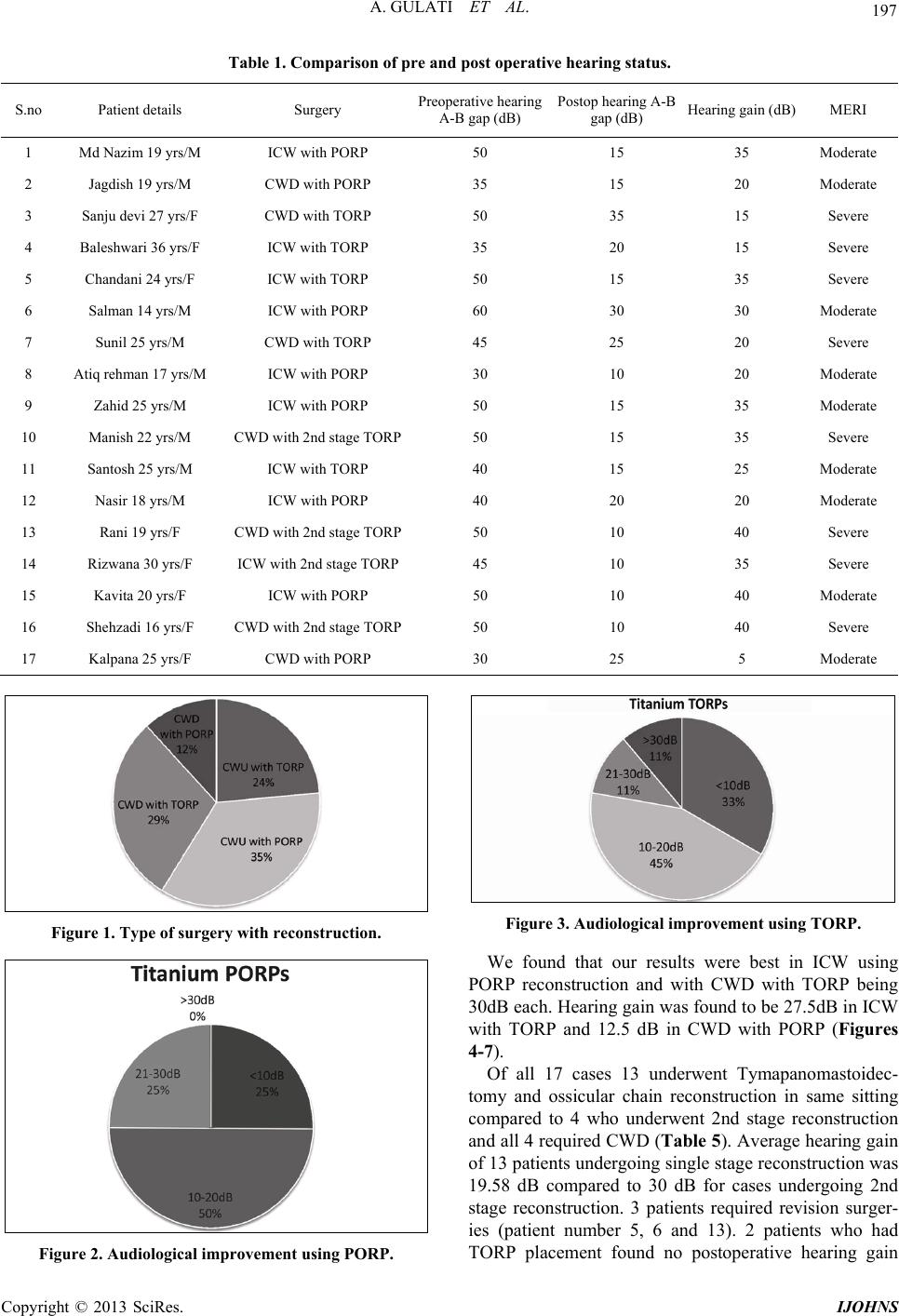
6 cases underwent ICW with PORP reconstruction and
4 cases underwent ICW with TORP reconstruction. In 5
Canal wall down with TORP reconstruction was at-
tempted and 2 cases underwent CWD with PORP recon-
struction (Figure 1). Average hearing gain was found to
be 28.75 dB in 10 cases undergoing ICW, compared to 7
cases undergoing CWD who had average postoperative
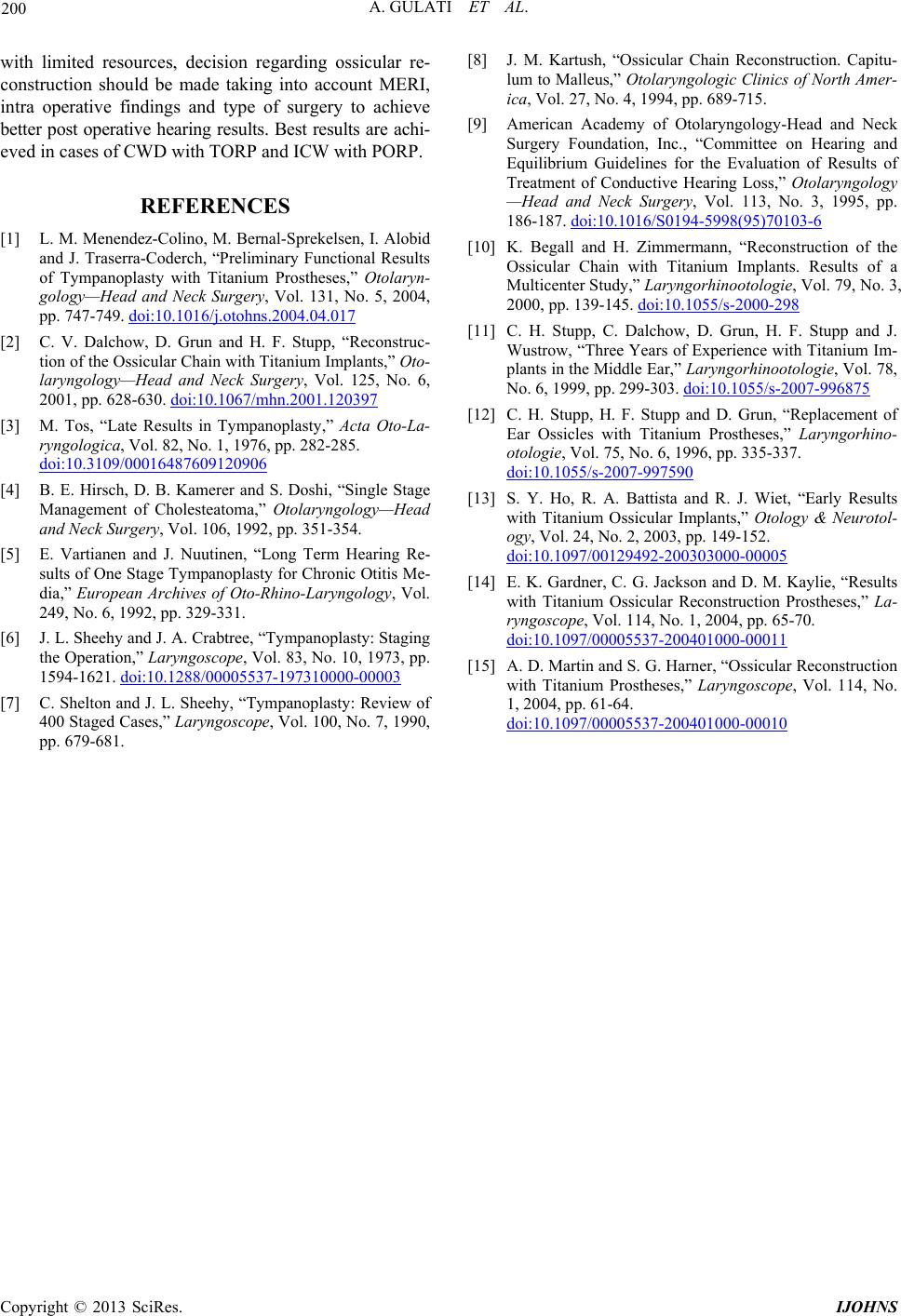
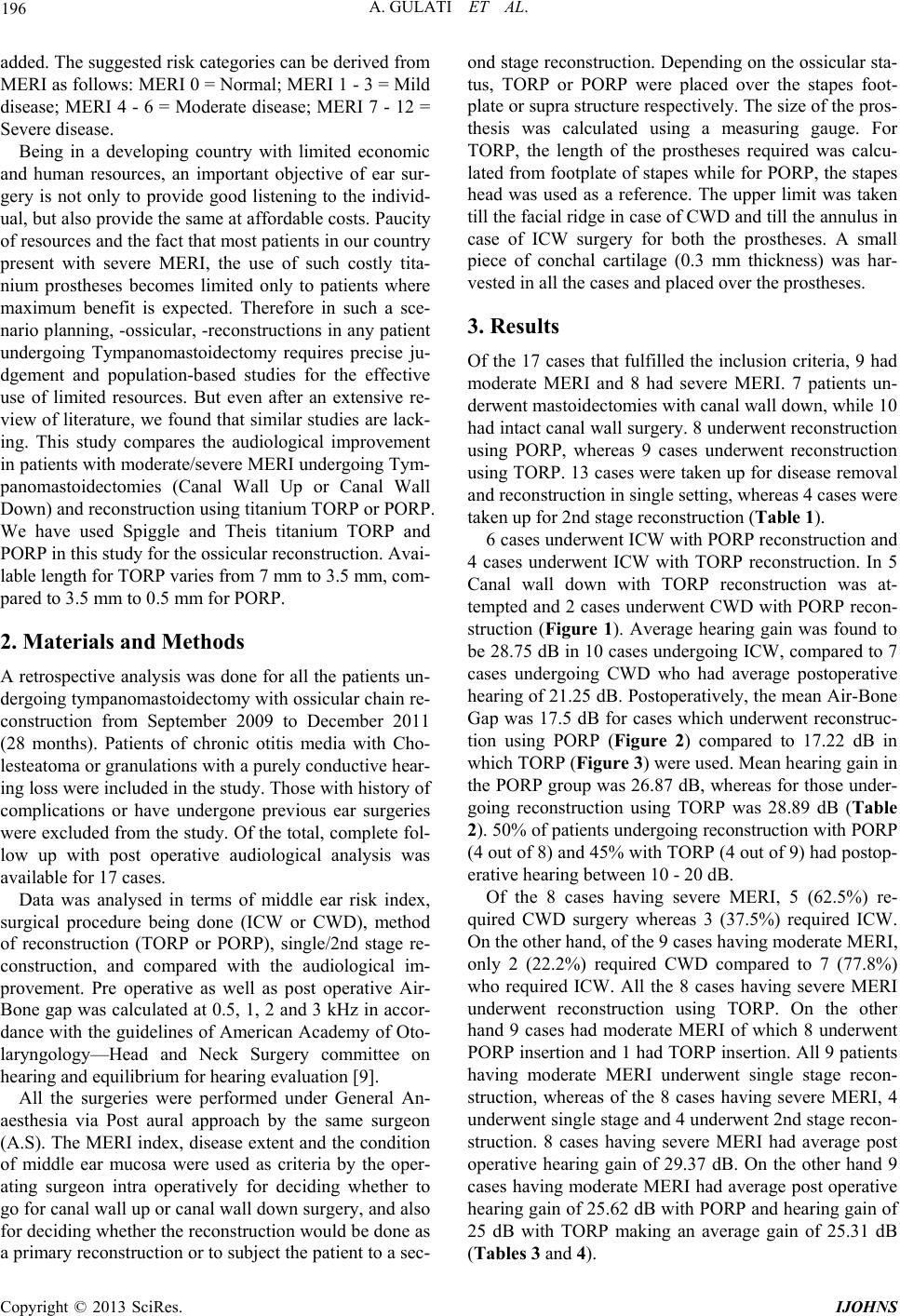
hearing of 21.25 dB. Po stoperatively, the mean Air-Bone
Gap was 17.5 dB for cases which underwent reconstruc-
tion using PORP (Figure 2) compared to 17.22 dB in
which TORP (Figure 3) were used. Mean hearing gain in
the PORP group was 26.87 dB, whereas for those under-
going reconstruction using TORP was 28.89 dB (Table
2). 50% of patients undergoing reconstruction with PORP
(4 out of 8) and 45% with TORP (4 out of 9) had postop-
erative hea r ing between 1 0 - 2 0 dB.
Of the 8 cases having severe MERI, 5 (62.5%) re-
quired CWD surgery whereas 3 (37.5%) required ICW.
On the other hand, of the 9 cases having moderate MERI,
only 2 (22.2%) required CWD compared to 7 (77.8%)
who required ICW. All the 8 cases having severe MERI
underwent reconstruction using TORP. On the other
hand 9 cases had moderate MERI of which 8 underwent
PORP insertion and 1 had TORP insertion. All 9 patients
having moderate MERI underwent single stage recon-
struction, whereas of the 8 cases having severe MERI, 4
underwent single stage and 4 underwent 2nd stage recon-
struction. 8 cases having severe MERI had average post
operative hearing gain of 29.37 dB. On the other hand 9
cases having moderate MERI had average post operative
hearing gain of 25.62 dB with PORP and hearing gain of
25 dB with TORP making an average gain of 25.31 dB
(Tables 3 and 4).
Copyright © 2013 SciRes. IJOHNS