To Optimize the Therapeutic Dose and Time Window of Picroside
II in Cerebral Ischemic Injury in Rats by Orthogonal Test
170
gesting a protective role of picroside II on both ische-
mic brain tissue and blood brain barrier.
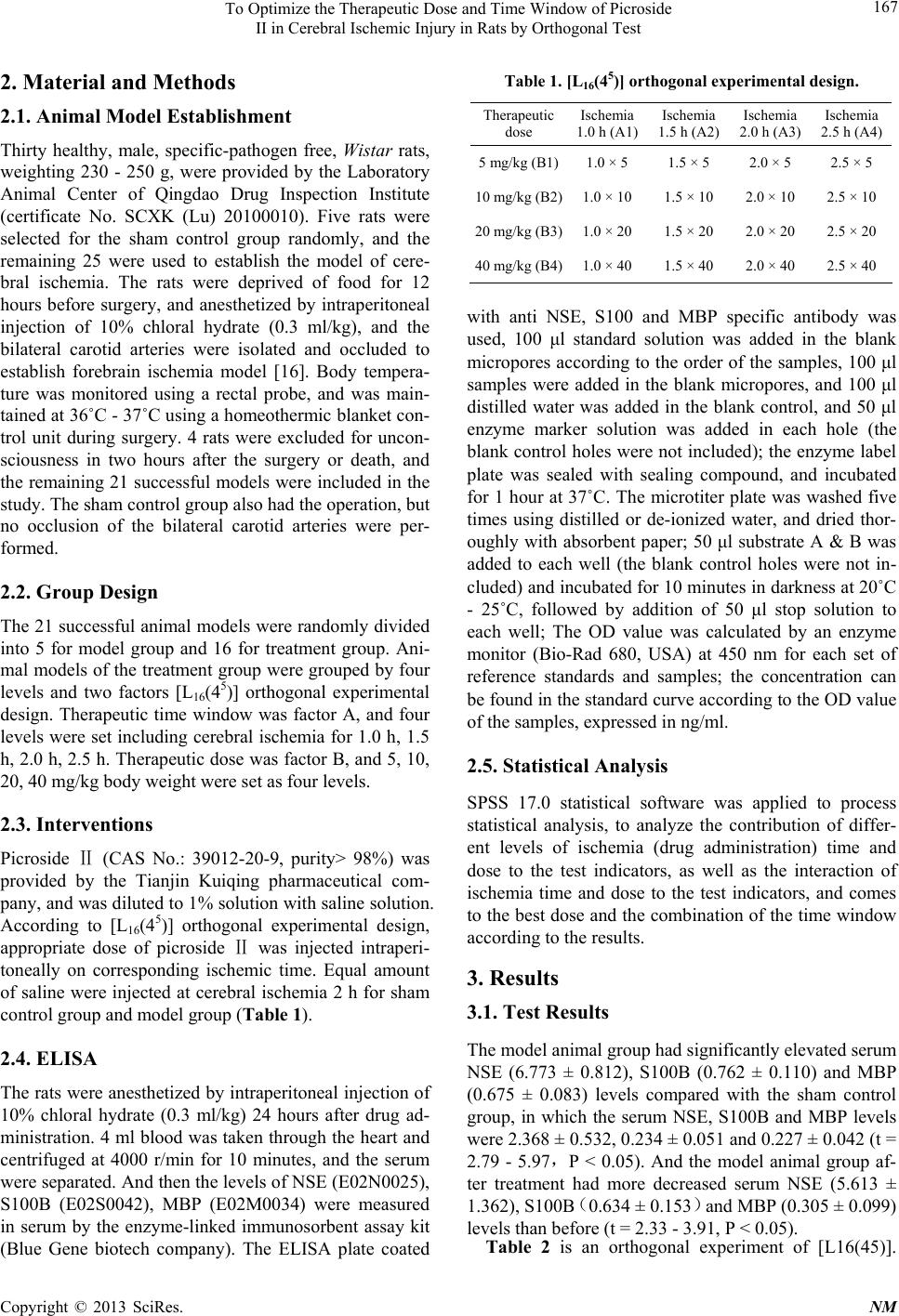
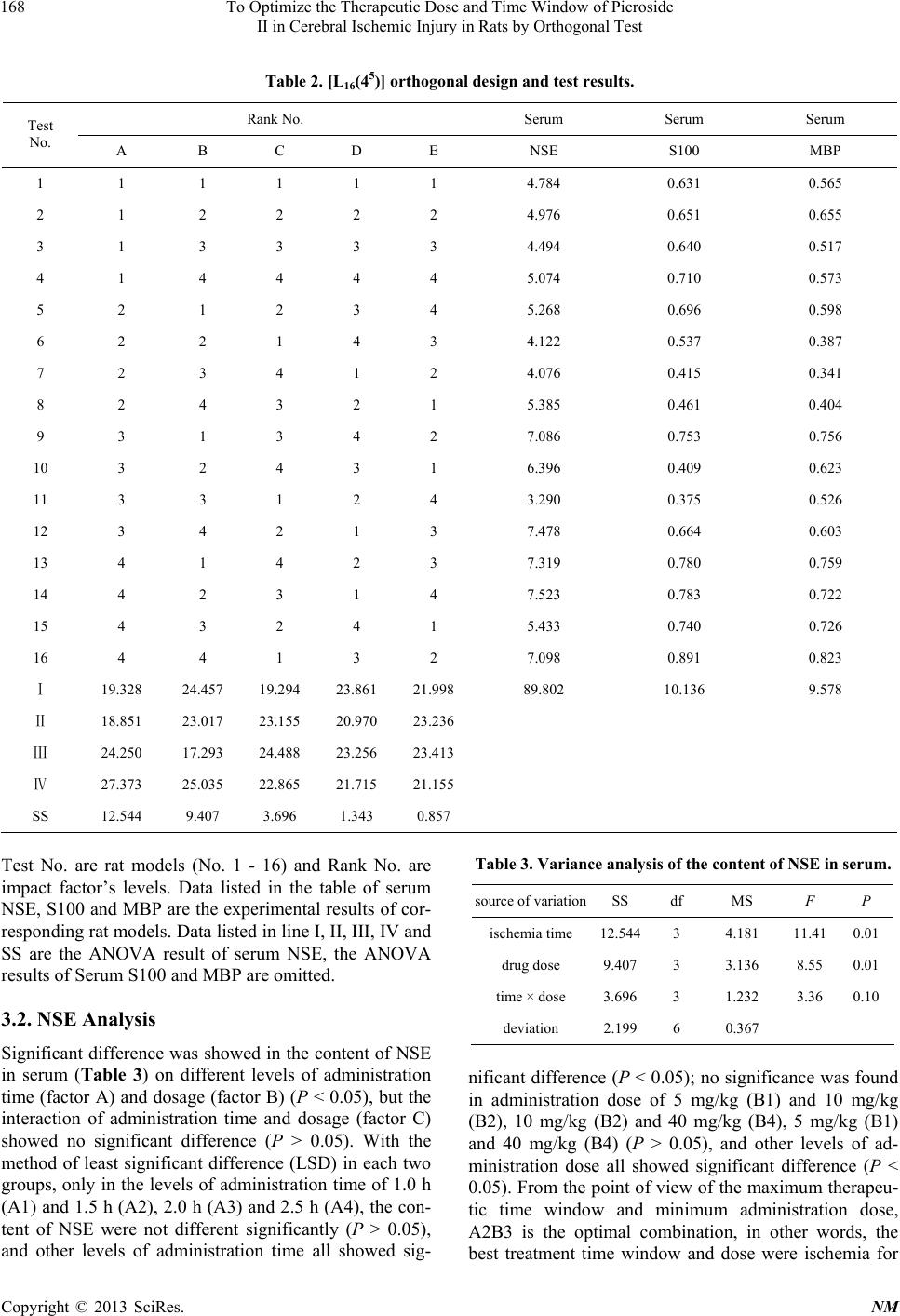
This experiment was a [L16(45)] orthogonal experi-
ment design, in which four time points of 1 h, 1.5 h, 2 h
and 2.5 h after brain ischemia were set and four levels of
picroside II dose were given (5 mg/kg, 10 mg/kg, 20 mg/kg
and 40 mg/kg). The expressions of NSE, S100B and
MBP in serum were measured, and the optimal therapeu-
tic dosage and time window of picroside II were analysed.
These results showed that there was a significant differ-
ence for the therapeutic effects of picroside II in admini-
stration time and the dose. From the principle of the low-
est therapeutic dose with the longest time window, A2B3
was the optimal combination and the best treatment time
window and dose were ischemia for 1.5 h and intraperi-
toneal injection of 20 mg/kg. For the mechanism of cere-
bral ischemic injury was very complicated, only four
indexes, as mentioned here, were observed in this study,
which must bring some variances. Therefore, the exact
mechanism and optimal therapeutic time window and
dosage of picroside II should be evaluated combined
with other detection indexes.
5. Acknowledgements
This study was supported by grant-in-aids for The Na-
tional Natural Science Foundation of China (No. 8104
1092, 81274116).
REFERENCES
[1] J. Joseph, F. F. Cruz-Sánchez and J. Carreras, “Enolase
Activity and Isoenzyme Distribution in Human Brain Re-
gions and Tumors,” Journal of Neurochemistry, Vol. 66,
No. 6, 1996, pp. 2484-2490.
doi:10.1046/j.1471-4159.1996.66062484.x
[2] V. Selakovic, R. Raicevic and L. Radenovic, “The In-
crease of Neuron-Specific Enolase in Cerebrospinal Fluid
and Plasma as a Marker of Neuronal Damage in Patients
with Acute Brain Infarction,” Journal of Clinical Neuro-
science, Vol. 12, No. 5, 2005, pp. 542-547.
doi:10.1016/j.jocn.2004.07.019
[3] R. H. Hatfield and R. M. McKernan, “CSF Neuron-Spe-
cific Enolase as a Quantitative Marker of Neuronal Dam-
age in a Rat Stroke Model,” Brain Research, Vol. 557,
No. 2, 1992, pp. 249-252.
doi:10.1016/0006-8993(92)90280-M
[4] T. X. Niu, Z. Y. Shi, J. J. Luo and X. D. Meng, “Determi-
nation and Clinical Significance of NSE and S-100β Pro-
tein in Hypoxia-Ischemia Brain Injured Rats (in Chinese),”
Chinese Journal of Comprehensive Medical, Vol. 19,
2009, pp. 34-37.
[5] E. C. Jauch, C. Lindsell, J. Broderick, S. C. Fagan, B. C.
Tilley, S. R. Levine and NINDS rt-PA Stroke Study
Group, “Association of Serial Biochemical Markers with
Acute Ischemic Stroke: The National Institute of Neuro-
logical Disorders and Stroke Recombinant Tissue Plasmi-
nogen Activator Stroke Study,” Stroke, Vol. 37, 2006, pp.
2508-2513. doi:10.1161/01.STR.0000242290.01174.9e
[6] T. Yardan, A. K. Erenler, A. Baydin, K. Aydin and C.
Cokluk, “Usefulness of S100B Protein in Neurological
Disorders,” Journal of Pakistan Medical Association, Vol.
61, 2011, pp. 276-281.
[7] M. Üstündağ, M. Orak, C. Güloğlu, Y. Tamam, M. B.
Sayhan and E. Kale, “The Role of Serum Osteoprotegerin
and S-100 Protein Levels in Patients with Acute Ischae-
mic Stroke: Determination of Stroke Subtype, Severity
and Mortality,” Severity and Mortality, Vol. 39, 2011, pp.
780-789.
[8] R. Kazmierski, S. Michalak, A. Wencel-Warot and W. L.
Nowinski, “Serum Tight-Junction Proteins Predict Hem-
orrhagic Transformation in Ischemic Stroke Patients,” Neu-
rology, Vol. 79, 2012, pp. 1677- 1685.
doi:10.1212/WNL.0b013e31826e9a83
[9] M. T. Wunderlich, C. W. Wallesch and M. Goertler, “Re-
lease of Neurobiochemical Markers of Brain Damage Is
Related to the Neurovascular Status on Admission and
the Site of Arterial Occlusion in Acute Ischemic Stroke,”
Journal of the Neurological Sciences, Vol. 227, No. 1,
2004, pp. 49-53. doi:10.1016/j.jns.2004.08.005
[10] K. J. Lamers, P. Vos, M. M. Verbeek, F. Rosmalen, W. J.
van Geel and B. G. van Engelen, “Protein S-100B, Neu-
ron-Specific Enolase (NSE), Myelin Basic Protein (MBP)
and Glial Fibrillary Acidic Protein (GFAP) in Cerebro-
spinal Fluid (CSF) and Blood of Neurological Patients,”
Brain Research Bulletin, Vol. 61, No. 3, 2003, pp. 261-
264. doi:10.1016/S0361-9230(03)00089-3
[11] Y. Z. Chen, Q. Yi, G. Liu, X. Shen, L. H. Xuan and Y.
Tian, “Cerebral White Matter Injury and Damage to Mye-
lin Sheath Following Whole-Brain Ischemia,” Brain Re-
search, Vol. 1495, 2013, pp. 11-17.
doi:10.1016/j.brainres.2012.12.006
[12] Z. Li, Q. Li, W. Shen and Y. L. Guo, “The Interferring
Effects of Picroside II on the Expressions of NF-κB and
I-κB Following Cerebral Ischemia Reperfusion Injury in
Rats,” Chinese Pharmacological Bulletin, Vol. 26, 2010,
pp. 52-55.
[13] Z. Li, Q. Li, Y. L. Guo, L. H. Qin and L. J. Luan, “Inter-
vention Effects of PicrosideⅡ in Cerebral Ischemic In-
jury Rats,” Acta Anat Sinica, Vol. 41, 2010, pp. 9-12.
[14] Y. L. Guo, X. Y. Xu, Q. Li, Z. Li and F. Du, “Anti-In-
flammation Effects of PicrosideⅡ in Cerebral Ischemic
Injury Rats,” Behavioral Brain Function, Vol. 6, 2010, pp.
43-53.
[15] H. T. Pei, X. Su, L. Zhao, H. Y. Li, Y. L. Guo, M. Z.
Zhang and H. Xin, “Primary Study for the Therapeutic
Dose and Time Window of PicrosideⅡ in Treating Cere-
bral Ischemic Injury in Rats,” International Journal of
Molecular Sciences, Vol. 13, 2012, pp. 2551-2562.
[16] A. Márquez-Martín, F. Jiménez-Altayó, A. P. Dantas, L.
Caracuel, A. M. Planas and E. Vila, “Middle Cerebral Ar-
tery Alterations in a Rat Chronic Hypoperfusion Model,”
Journal of Applied Physiology, Vol. 112, 2012, pp. 511-
518. doi:10.1152/japplphysiol.00998.2011
Copyright © 2013 SciRes. NM