Stabilization of Circadian Rhythm, Its Augmentation by Bright Light Treatment
and Its Importance for ADHD and Depression of Adolescents 151
sions/week) since one month before the 4 week study
period.
ADHD symptoms were assessed weekly by the Con-
ner scales [6]. This test has an excellent variation sensi-
tivity and an 81% sensitivity and 61% specificity for
ADHD. It consists of 20 items, 10 of which describe in-
attention and 10 describe hyperactivity. The items are to
be rated on a scale from 0 = never existing to 3 = always
existing. Each of the two subscales has a cut-off of 14, i.e.
that scores of >14 are typical for ADHD.
Step 1 (Baseline): 28 Volunteers were admitted and
began with the initial baseline week of the study. The
purpose of the baseline week of the study was to be able
to differentiate change s of the Conner score between out-
and in-patient treatment and to that of placebo and BLT
treatment. Conner scores were measured at the day of
admission and one week after admission (Prae-trial).
Step 2 (Verum): In the second week of the study, the
28 patients were asked to sit alone in front of the bright
light box (2500 lux) from 09:00 to 10:00 a.m. In this time,
patients played or listened to a story. Conner scores were
measured after the second week.
Step 3 (Placebo): In the third week of the study, the 28
volunteers were asked to sit alone in front of the placebo
light box for (50 lux) 60 minutes in the morning, from
09:00 to 10:00 a.m, In this time, patients played or lis-
tened to a story. This aspect of the design followed the
general principle of clinical trial design that better con-
trasts between active and placebo. As reviewed by East-
man [7], the issue of placebo responses has been a seri-
ous problem in clinical bright light studies, though the
placebo problem has been negligible in studies of the
physiologic effects of light. Conner scores were meas-
ured after the third week.
Step 4 (Post): In the fourth week of the study, the 28
patients received neither placebo nor BLT. The purpose
of this week of the study was again to be able to differ-
entiate changes of the Conner score related to ADHD to
that of placebo and BLT treatment. Conner scores were
measured after the fourth week.
Saliva samples were collected one week before (Base-
line) and one day be fore placebo treatment (Prae), on the
day between verum and placebo treatment (Verum), on
the day after placebo treatment (Placebo) and one week
after placebo treatment (Post), at each time at 08:00 a.m.
and 08:00 p.m., and assayed for melatonin to characterize
the circadian phase of the subject’s melatonin rhythms
(ELISA, Immuno Biological Laqboratories, Hamburg,
Germany). Saliva samples were used because of the con-
venience for the patients.
The subjects completed a weekly Assess ment for Treat-
ment Emergent Events (SAFTEE) symptom scale. Four
weeks of treatment were carried out with weekly symp-
tom assessments. The investigators visited su bjects weekly
to assure their safety and their compliance with the study,
and to administer and collect rating forms.
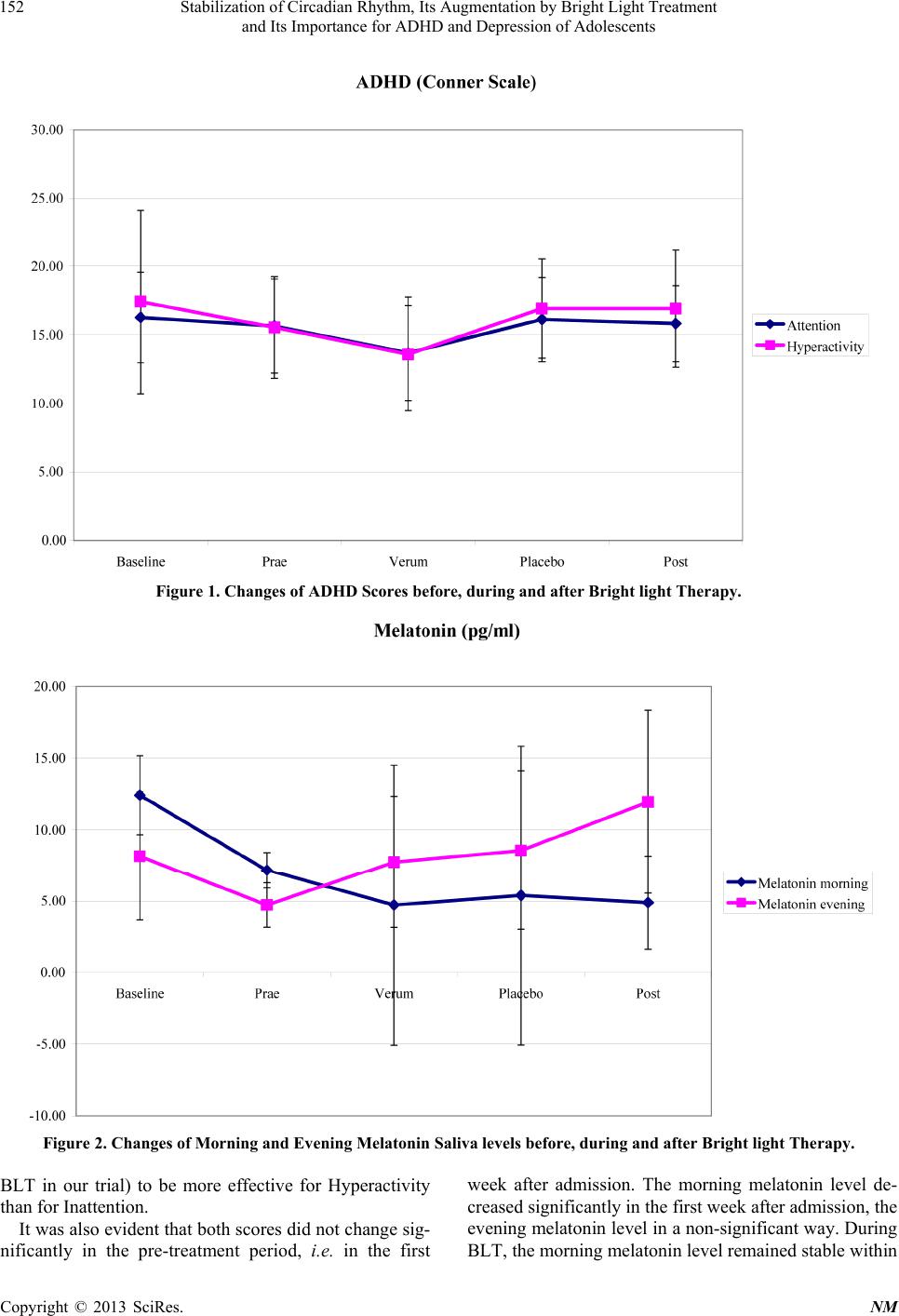
3. Results
Subjects’ moods and salivary melatonin levels improved
under both treatments (Table 1). With respect to inatten-
tion, Conner scores were stable in the pre-treatment pe-
riod (Score 16.3, cut-off 14), improved during treatment
with bright light therapy to the score of 12.7. In the pla-
cebo and post-treatment period, the score rose again up
to 15.8 (Figure 1).
Regarding hyperactivity, Conner scores dropped in the
pre-treatment period from 17.4 to 16, improved during
treatment with bright light therapy to the score of 13.6. In
the placebo and post-treatment period, the score rose
again up to 16.9 (Figure 1).
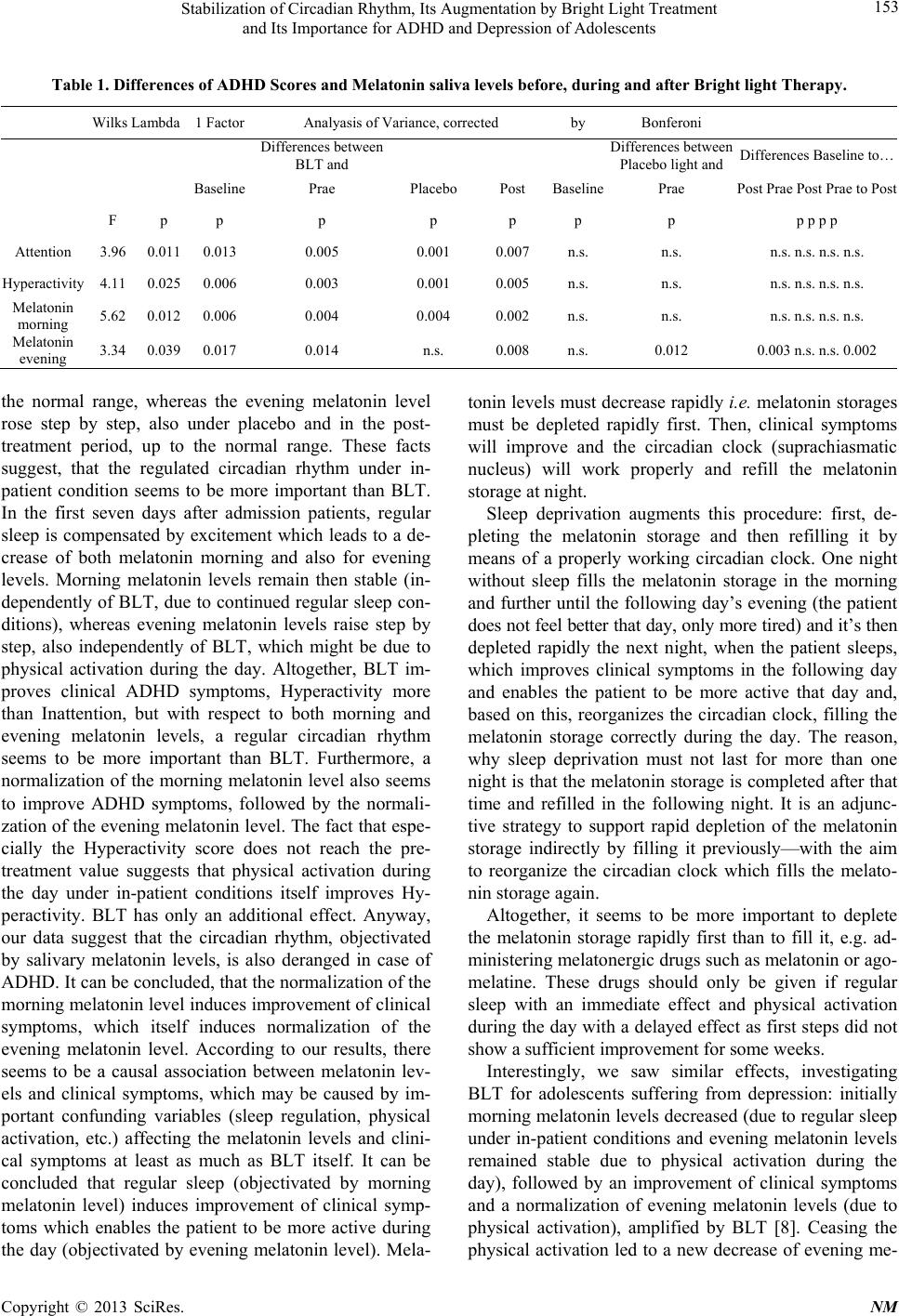
Salivary melatonin, measured in the morning, showed
a remarkable decrease from the pre-treatment period (13
pg/ml-range < 10 pg/ml) to the BLT, placebo-, and the
post-treatment period (4pg/ml). Salivary melatonin,
measured in the evening, also decreased slightly in the
pre-treatment period from 8 pg/ml to 5 pg/ml (range > 10
pg/ml), and increased after placebo to again 8pg/ml, after
BLT even to 9 pg/ml, and to 12 pg/ml in the post-treat-
ment week (Figure 2).
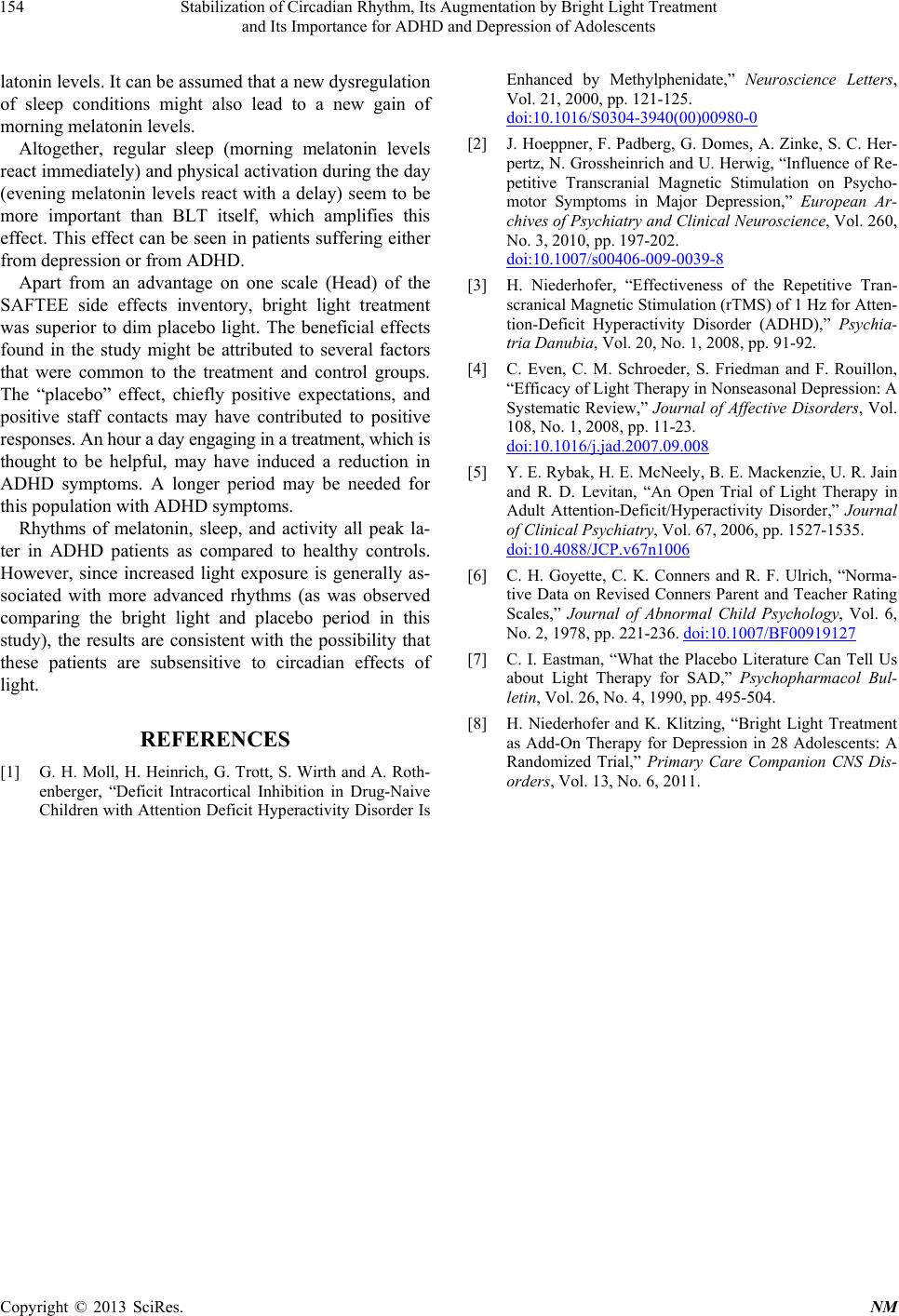
Significant differences of Conner scores and melatonin
levels are depicted in Table 1.
Participants experienced no suicide attempts. There
were no incidents of mania or hypomania during the light
treatment.
The weekly SAFTEE physical symptom inventory
(range: severe-moderate-mild-minimal-not existing) was
examined for adverse reactions. The symptom Headache
improved with bright light in one patient from mild to
minimal, and with dim light, nausea and vomiting im-
proved in the other patient also from mild to minimal.
This improvement lasted until th e end of the study. With
respec t to the other symptoms, patient did not repo rt any
change, i.e. they were always scored as “minimal” or
“not existing”, without any changes in the four weeks.
4. Discussion
BLT led to a significant reduction of the Con ner Inatten-
tion score and also showed an improvement in the Con-
ner Hyperacivity Score. In addition, the social structure
and regularized sleep might be beneficial. Interestingly,
there was a more significant decrease in the Hyperactiv-
ity than in the Inattention Score, which suggested that
BLT was more effective in case of Hyperactivity than of
Inattention. This corresponds to recent findings which
suggest biological therapies (such as sleep regulation and
Copyright © 2013 SciRes. NM